

Abstract
INTRODUCTION
Obturator hernia is an extremely rare type of hernia with relatively high mortality and morbidity. Its early diagnosis is challenging since the signs and symptoms are non specific.
PRESENTATION OF CASE
Here in we present a case of 70 years old women who presented with complaints of intermittent colicky abdominal pain and vomiting. Plain radiograph of abdomen showed acute dilatation of stomach. Ultrasonography showed small bowel obstruction at the mid ileal level with evidence of coiled loops of ileum in pelvis. On exploration, Right Obstructed Obturator hernia was found. The obstructed Intestine was reduced and resected and the obturator foramen was closed with simple sutures. Postoperative period was uneventful.
DISCUSSION
Obturator hernia is a rare pelvic hernia and poses a diagnostic challenge. Obturator hernia occurs when there is protrusion of intra-abdominal contents through the obturator foramen in the pelvis. The signs and symptoms are non specific and generally the diagnosis is made during exploration for the intestinal obstruction, one of the four cardinal features. Others are pain on the medial aspect of thigh called as Howship Rombergs sign, repeated attacks of Intestinal Obstruction and palpable mass on the medial aspect of thigh.
CONCLUSION
Obturator hernia is a rare but significant cause of intestinal obstruction especially in emaciated elderly woman and a diagnostic challenge for the Doctors. CT scan is valuable to establish preoperative diagnosis. Surgery either open or laproscopic, is the only treatment. The need for the awareness is stressed and CT scan can be helpful.
Keywords: Obturator hernia, Intestinal obstruction, Computed Tomography scan, Laproscopy
1. Introduction
Obturator hernia is a rare pelvic hernia with incidence of 1%1 and most commonly presents as Acute Intestinal Obstruction with contents being small bowel in majority of cases. It can also contain Appendix, Meckels Diverticulum or Omentum. The hernia sac passes through the obturator foramen, following the path of obturator nerves and muscles. Patients can present with pain on the medial aspect of thigh,3 recurrent episodes of intestinal obstruction or palpable mass on the medial aspect of thigh. CT scan has superior sensitivity and accuracy.4 Here we present a case of obturator hernia which was operated in emergency and was performed successfully.
2. Presentation of case
A 70-year old women admitted in surgical ward with vomiting, intermittent colicky pain in abdomen since 5 days. She experienced generalized weakness and constipation since few days. For the past 2–3 years, she had severe intermittent colicky lower abdominal pain that usually lasted several hours but resolved spontaneously. Clinical examination showed a moderate built patient, generally unwell with a temperature of 38.4 °C, pulse of 96 min–1 low volume and blood pressure of 90/60 mm Hg with dry tongue and sunken eyes. Local Examination showed central distension of abdomen with generalized tenderness and guarding present. Other Systems were essentially normal. Per rectal and Per vaginal examinations were normal. Investigations revealed increased white blood cell count with deranged renal function tests. X-ray Abdomen showed Acute Dilatation of stomach and Chest X-ray showed Interstitial Lung Disease. A Provisional Diagnosis of Gastric Outlet Obstruction was done.
Patient was managed with Nil by mouth, Ryles tube aspiration continuous and 2 hourly aspirate, and Broad spectrum Antibiotics. Pt was adequately hydrated and Renal function tests were repeated which were normal. Oesophagogastroduodenoscopy revealed normal study. She was started on oral feeds and later she again developed symptoms of vomiting and pain in abdomen. Ultrasonography showed Small Bowel Obstruction at mid-ileal level with evidence of coiled up loop of ileum in pelvis. She was again kept Nil by mouth. Pt remained unwell and decision was made to carry out Exploratory Surgery.
On Exploration, Right Sided Obstructed Obturator Hernia with dilated proximal and mid ileal loop with prolapsed distal ileal loop was found (Fig. 1). Obstruction segment was reduced and resected. Ileo-Ileal Resection Anastomosis with repair of obturator hernia with simple sutures was done (Fig. 2). Patient was kept in ICU for 2 days. She was treated with Broad spectrum antibiotics, rational nutritional support and careful monitoring of vital organs was done. Her post-operative period was uneventful. She was discharged after 10 days. Pt remained well without any complications during subsequent outpatient follow up and has since been discharged.
Fig. 1.
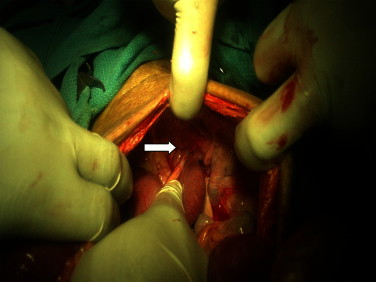
Gross photograph of Right Sided Obstructed Obturator Hernia with dilated proximal and mid-ileal loop with prolapsed distal ileal loop.
Fig. 2.
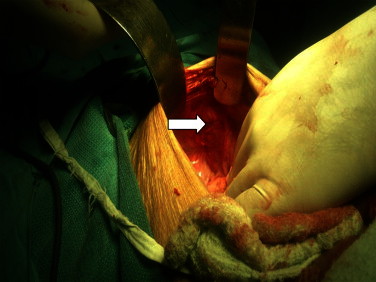
Gross photograph of Repair of the Rt. Sided Obturator Hernia.
3. Discussion
Obturator hernia is a very rare pelvic hernia.1 With the nickname “little old lady's hernia”, it usually occurs in multiparous and elderly emaciated women It is 9 times more common in females due to their wider pelvis, more triangular obturator canal opening, and greater transverse diameter. The other risk factors include chronic obstructive pulmonary disease, chronic constipation and ascites. Obturator hernia is a diagnostic challenge because the signs and symptoms are usually non-specific. The cardinal clinical symptom is Acute Intestinal Obstruction. The clinical course is usually manifested by acute small bowel obstruction, pain on the medial aspect of thigh due to compression of obturator nerve. This is called as Howships Romberg sign, past history of recurrent attacks of intestinal obstruction, palpable mass in groin.3 This patient presented with complaints of Acute Intestinal Obstruction, with past history of recurrent attacks of intestinal obstruction. The early diagnosis is challenging when the symptoms and signs are nonspecific. Various imaging modalities have been applied to establish the diagnosis, including ultrasonography, herniography, CT scan. Among them, CT scan has superior sensitivity and accuracy.4
The only treatment for obturator hernia is surgery. There are a variety of operative approaches including inguinal, retropubic and transperitoneal approach.4,5 In the emergency setting, the abdominal approach via a low midline incision is most commonly favoured, as it allows adequate exposure of the obturator ring as well as the identification and resection of any ischaemic bowel. Laparotomy via low midline incision was done in this case. Recently, Laparoscopic surgery for obturator hernia became another alternative approach 7. The advantages of laparoscopic surgery include less postoperative pain, shorter hospital stay and lower complications. However, it is usually reserved for the nonstrangulated hernia because of more challenging techniques and longer learning curve. Both transabdominal and extraperitoneal approaches have been described. Transabdominal approach is appropriate for the emergency setting, as it allows exploration of the abdominal cavity, diagnosis of the cause of the bowel obstruction, reduction of the hernia, thorough inspection and identification of ischaemic bowel, and resection of bowel if required.2 The laparoscopic total extraperitoneal (TEP) approach is more feasible if the diagnosis is established before surgery in symptomatic patients. More often than not, obturator hernia is detected during TEP repair for inguinal hernias. This reflects the importance of inspecting all the myopectineal orifices during the TEP approach to allow for the diagnosis and repair of asymptomatic obturator hernias.6 Methods of repair include simple suture closure, closure of the obturator with adjacent tissue, and mesh replacement during laparotomy.8 Many authors preferred a simple closure of the hernial defect with one or more interrupted sutures, in case of bowel resection.4,7 In this case we did the simple suture and outcome was satisfying.
4. Conclusion
Obturator hernia is a rare but significant cause of intestinal obstruction especially in emaciated elderly woman and a diagnostic challenge for the Doctors. CT scan is valuable to establish preoperative diagnosis. The need for the awareness of early diagnosis is stressed with emphasis on surgical management.
Conflicts of interest statement
None.
Funding
None.
Ethical approval
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Author contributions
Dr. Sanjeev R. Kulkarni: Abstract; Dr. Aditya R. Punamiya: Presentation of case and Discussion; Dr. Ramchandra G. Naniwadekar: Introduction; Dr. Hemant B. Janugade: Conclusion; Dr. Tejas D. Chotai: References; Dr. T. Vimal Singh: Figures; Dr. Arafath Natchair: Figures.
Acknowledgement
We are thankful to Mrs. M.C. Deshingkar from Surgery Dept. Office for her secretarial help.
References
- 1.Lo C.Y., Lorentz T.G., Lau P.W. Obturator hernia presenting as small bowel obstruction. American Journal of Surgery. 1994;167:396–398. doi: 10.1016/0002-9610(94)90123-6. [DOI] [PubMed] [Google Scholar]
- 2.Bryant T.L., Umstot R.K., Jr. Laparoscopic repair of an incarcerated obturator hernia. Surgical Endoscopy. 1996;10(4):437–438. doi: 10.1007/BF00191635. [DOI] [PubMed] [Google Scholar]
- 3.Hernia A.J. In: Maingot's abdominal operations. 10th ed. Zinner M.J., Schwartz S.I., Ellis H., editors. Appleton & Lange; London, GB: 1997. pp. 540–541. [Google Scholar]
- 4.Shipkov C.D., Uchikov A.P., Grigoriadis E. The obturator obtu-rator hernia. Hernia: difficult to diagnose, easy to repair. Hernia. 2004;8:155–157. doi: 10.1007/s10029-003-0177-2. [DOI] [PubMed] [Google Scholar]
- 5.Shapiro K., Patel S., Choy C., Chaudry G., Khalil S., Ferzli G. Totally extraperitoneal re-pair of obturator hernia. Surgical Endoscopy. 2004;18:954–956. doi: 10.1007/s00464-003-8212-z. [DOI] [PubMed] [Google Scholar]
- 6.Shapiro K., Patel S., Choy C., Chaudry G., Khalil S., Ferzli G. Totally extraperitoneal repair of obturator hernia. Surgical Endoscopy. 2004;18(6):954–956. doi: 10.1007/s00464-003-8212-z. [DOI] [PubMed] [Google Scholar]
- 7.Yau K.K., Siu W.T., Fung K.H., Li M.K. Small-bowel obstruction secondary to incarcerated obturator hernia. American Journal of Surgery. 2006;192:207–208. doi: 10.1016/j.amjsurg.2006.01.014. [DOI] [PubMed] [Google Scholar]
- 8.Pandey R., Maqbool A., Jayachandran N. Obturator hernia: a diagnostic challenge. Hernia. 2009;13:97–99. doi: 10.1007/s10029-008-0406-9. [DOI] [PubMed] [Google Scholar]