

In agreement with the study by Fazekas and colleagues [1] in a recent issue of Critical Care, an increase in the concentration of carbon monoxide (CO) has been observed after surgery and cardiopulmonary bypass and during sepsis [2]. Although inflammation induces heme oxygenase and the above-mentioned conditions do lead to inflammation, a clear association in humans has not been established, underlining the relevance of the remarks made by Cove and Pinsky [3] in the same issue of Critical Care. We would like to present data that illustrate that inflammation does increase CO in humans in vivo.
During experimental endotoxemia in humans, a controlled immune response is evoked, leading to increased levels of several pro- and anti-inflammatory markers [4]. Recent experiments demonstrated that, in 38 healthy male volunteers infused with US Standard Reference Endotoxin (National Institutes of Health, Bethesda, USA) obtained from Escherichia coli O:113 at a dose of 2 ng/kg, tumor necrosis factor-alpha concentrations increase at t = 2 hours to a median of 610 pg/mL (interquartile range of 400 to 853 pg/mL; Friedman test P <0.001) and arterial carboxyhemoglobin levels increase by 42% at 4 hours after lipopolysaccharide infusion (Friedman test P = 0.0057) (Figure 1). During these experiments, subjects breathed ambient air in a climate-controlled room; therefore, Cove and Pinsky's claim that an increase of CO is due to an increase in inhalation is unlikely.
Figure 1.
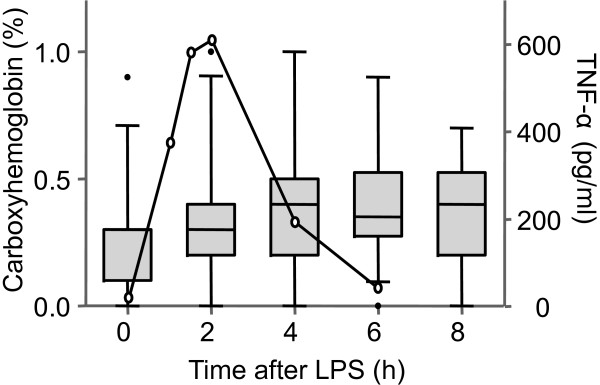
Tumor necrosis factor-alpha (TNF-α) and carboxyhemoglobin levels in arterial blood during experimental human endotoxemia. At t = 0 hours, 38 healthy male subjects were infused with 2 ng/kg Escherichia coli endotoxin. Arterial blood was sampled serially to determine concentrations of carboxyhemoglobin (Siemens Rapidlab 348 blood gas analyzer; Siemens Medical Solutions, Munich, Germany) and plasma TNF-α (Bio-plexcytokine assay; Bio-Rad Laboratories, Inc., Hercules, CA, USA, at a Luminex 100; Luminex Corporation, Oosterhout, The Netherlands). Carboxyhemoglobin levels are presented by boxplots, and whiskers indicate 5th to 95th percentiles. TNF-α is presented as median (black line); for clarity, interquartile range is omitted. Statistical analysis was performed by using the Friedman test (carboxyhemoglobin: P = 0.0057; TNF-α: P <0.001). LPS, lipopolysaccharide.
Interestingly, the anti-inflammatory effects of CO have also been studied in this model. Although CO has had clear beneficial effects in several animal studies, inhaled CO during experimental endotoxemia failed to influence the inflammatory response in humans [5], making it unclear whether the artificial increase of CO could benefit critically ill patients.
Abbreviations
CO: carbon monoxide.
Competing interests
MJD is a recipient of an AGIKO grant of the Netherlands Organization for Health Research and Development (ZonMw).
See related research by Fazekas et al., http://ccforum.com/content/16/1/R6
Contributor Information
Mirrin Josefien Dorresteijn, Email: m.dorresteijn@ic.umcn.nl.
Peter Pickkers, Email: p.pickkers@ic.umcn.nl.
References
- Fazekas AS, Wewalka M, Zauner C, Funk GC. Carboxyhemoglobin levels in medical intensive care patients: a retrospective, observational study. Crit Care. 2012;16:R6. doi: 10.1186/cc11138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morimatsu H, Takahashi T, Matsusaki T, Hayashi M, Matsumi J, Shimizu H, Matsumi M, Morita K. An increase in exhaled CO concentration in systemic inflammation/sepsis. J Breath Res. 2010;16:047103. doi: 10.1088/1752-7155/4/4/047103. [DOI] [PubMed] [Google Scholar]
- Cove ME, Pinsky MR. Carboxyhemoglobin levels in medical intensive care patients. Crit Care. 2012;16:411. doi: 10.1186/cc11018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Suffredini AF, Hochstein HD, McMahon FG. Dose-related inflammatory effects of intravenous endotoxin in humans: evaluation of a new clinical lot of Escherichia coli O:113 endotoxin. J Infect Dis. 1999;16:1278–1282. doi: 10.1086/314717. [DOI] [PubMed] [Google Scholar]
- Mayr FB, Spiel A, Leitner J, Marsik C, Germann P, Ullrich R, Wagner O, Jilma B. Effects of carbon monoxide inhalation during experimental endotoxemia in humans. Am J Respir Crit Care Med. 2005;16:354–360. doi: 10.1164/rccm.200404-446OC. [DOI] [PubMed] [Google Scholar]