

Abstract
Background:
Subthalamic nucleus deep brain stimulation is effective in reducing motor symptoms in appropriately selected patients with Parkinson's disease. We identified factors that contribute to poor outcomes during early, middle and late stages of stimulation management in a series of patients that were referred for troubleshooting poor outcomes.
Methods:
We performed a retrospective review of 50 patients with bilateral STN DBS seen in our movement disorders clinic with unsatisfactory clinical response and/or patient dissatisfaction with deep brain stimulation outcome. All patients underwent a systematic evaluation to assess the primary cause of suboptimal outcome including lead position, hardware integrity, patient selection, patient expectations, effective use of stimulation settings, and pre- and postoperative levodopa responsive symptoms. The data was also analyzed by duration of stimulation to determine if these factors varied by stage of DBS management.
Results:
Our series included patients implanted 4-68 months. We identified the following primary factors impacting outcome: Suboptimal stimulation settings (52%), disease progression (16%), inappropriate patient selection (10%), hardware damage (8%), lead malposition (8%), met expected motor outcomes (6%). Lead revision surgery occurred in 14%. Reversible factors accounted for dissatisfaction in 74%. Suboptimal stimulation was the dominant factor affecting outcomes in early and long-term management phases.
Conclusion:
STN DBS outcomes can be improved even years after implantation. Stimulation parameters warrant investigation throughout the continuum of DBS management as a reversible cause of poor outcomes.
Keywords: Deep brain stimulation, long-term management, outcomes, Parkinson's disease, subthalamic nucleus
INTRODUCTION
Subthalamic nucleus (STN) deep brain stimulation (DBS) can improve Parkinson's disease (PD) tremor and motor complications such as fluctuations and dyskinesia robustly in the initial years postimplantation with sustained efficacy noted over 10 years.[2–5] Published guidelines for patient selection, management,[1] and assessment of factors affecting outcomes[7,8] are available to clinicians. In this series, we describe the reversible and irreversible factors causing dissatisfaction with DBS outcomes. We separated our series into early optimization phase, early maintenance phase, and later maintenance phase of clinical management to determine if any factor was more common during any of the postoperative stages and whether motor symptoms could still be improved despite disease progression years after DBS implantation.
MATERIALS AND METHODS
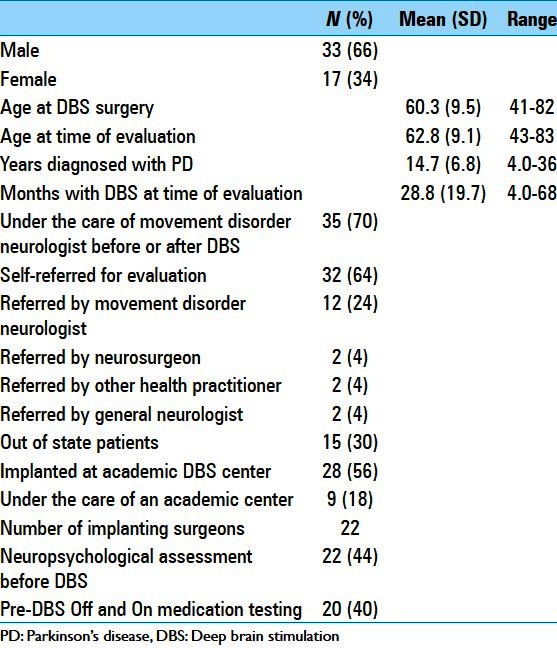
We performed a retrospective chart review of 50 consecutive PD patients with bilateral STN DBS evaluated due to patient or clinician dissatisfaction with DBS that prompted a referral. Table 1 describes patient characteristics and chart review data. After a review of past medical records, patients were scheduled for intensive troubleshooting if they had reported known stimulation side effects (paresthesia, speech slurring), signs of hardware damage (heating sensation, shocks), unexpected symptom deterioration (abrupt postoperative gait or balance declines), or lack of response to stimulation (no or poor improvement in preoperative tremor, rigidity, bradykinesia, motor fluctuations or dyskinesia). These patients underwent 2-4 days evaluation to include a neurologic evaluation by a movement disorders specialist and a Unified Parkinson's disease Rating Scale motor (mUPDRS) evaluation on and off presenting stimulation settings, system integrity check, and a systematic review of stimulation side effect and efficacy threshold testing of each electrode in the medication off state. Plain X-ray or brain computed tomography (CT) was obtained if hardware damage was suspected or lead placement was in question. Primary factors affecting DBS outcomes were defined by categories identified in prior studies,[7,8] namely patient selection, lead location, hardware malfunction, suboptimal programming settings, disease progression, and patient expectations. Factors were further analyzed by stage of clinical management defined as (1) stimulation optimization phase (1-12 months during which stimulation settings and medication doses are optimized), (2) early maintenance phase (13-24 months during which time the optimal beneficial effects of stimulation are noted), and (3) late maintenance phase (>24 months when hardware integrity and battery status are monitored and levodopa responsive symptoms have sustained benefit from stimulation).
Table 1.
Patient demographics
RESULTS
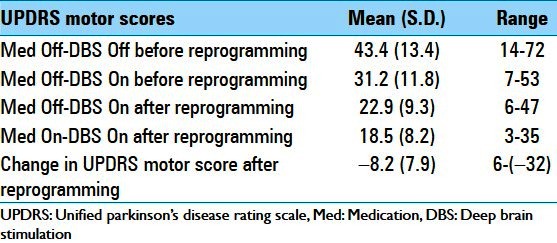
Fifty patients were evaluated between 2007 and 2010 and are described in Table 1. The group had PD for a mean of 14.7 (range 4-36) years and DBS for a mean of 28.8 (range 4-68) months. Thirty-two patients were self-referred. Worsening of axial symptoms (gait, imbalance, freezing, and speech) was the main reason for assessment and noted as a chief complaint in 74% of patients. Table 2 lists the reasons for referral as noted by self-referral vs. clinician referral. Table 3 illustrates the mUPDRS scores before and after programming adjustments.
Table 2.
Referral source and reasons stated for referral
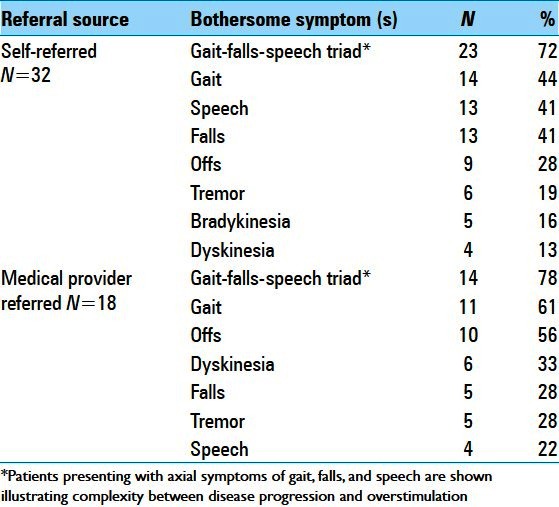
Table 3.
Evaluation results: UPDRS motor scores
The primary factors impacting outcome for the group were suboptimal stimulation settings in 52%, hardware damage in 24%, disease progression in 16%, lead malposition in 8%, and inappropriate presurgical patient selection in 10%. Six percent met the benchmarks for benefit,[5] although unhappy with DBS due to stimulation side effects involving speech and untreated anxiety. Forty percent had more than one factor impacting outcomes and 74% had reversible factors impacting outcomes. Figure 1 illustrates the factors affecting outcome for the group compared with each clinical management phase.
Figure 1.

Primary problem at time of evaluation DBS: Deep brain stimulation
Stimulation optimization phase (up to 12 months postimplantation)
Fourteen patients had DBS for up to 1 year. Axial symptoms were the reason for referral in nine patients. Of the five patients deemed poor candidates, two had multisystem atrophy with symptom onset less than 5 years prior to surgery, one had dementia, and two had dopaminergic nonresponsive motor symptoms with severe gait freezing. Five patients had wire damage but only two required lead replacement as programming options remained for the remaining three patients. Stimulation adjustment in the remaining eight patients (including the patient with dementia) further improved mUPDRS. Off medication on stimulation mUPDRS scores improved from 26% to 48% after reprogramming. Of note, axial symptoms improved in five patients when stimulation side effects (presumably internal capsule) were eliminated.
Early maintenance phase (second year postoperative)
Of the 12 patients in the early maintenance phase, 1 had multiple system atrophy (MSA) and not a surgical candidate, 3 had malpositioned leads, and 2 had hardware damage requiring surgical referral for revision. In total, five patients were referred to a surgeon for lead revision. Stimulation adjustment improved mUPDRS scores in the remaining seven patients. Off medication on stimulation mUPDRS scores improved from 24% to 51% after reprogramming. Of note, gait improved objectively in the patient with MSA through reduction in internal capsule stimulation affecting lower extremities.
Late maintenance phase (more than 2 years postoperative)
Twenty-four patients were evaluated in this phase. Twenty patients had a primary complaint of axial symptoms of which eight were diagnosed with disease progression as determined by the nonlevodopa responsive symptoms also unresponsive to stimulation. Reprogramming did improve mUPDRS scores in 11 patients. The off medication on stimulation mUPDRS scores improved from 22% to 54% after reprogramming. Four had hardware damage requiring lead replacement in two and frailty prevented lead replacement in the other two. The remaining three patients were meeting expectations at mUPDRS 52% when compared with benchmarks for motor outcomes in the literature[5] but were experiencing stimulation-induced speech slurring and anxiety, which prompted the referral. Reprogramming eliminated the speech slurring and anxiety without compromising their motor score.
DISCUSSION
Similar to others, we have found the use of a systemic approach[6] and a classification system for factors that can cause suboptimal DBS outcomes invaluable to long-term management.[8]
There are marked differences in the cause for suboptimal DBS response in our series compared with prior reporting.[8] Okun et al. reported the results from 41 patients with PD, essential tremor or dystonia evaluated in two movement disorder centers. Fewer patients (8%) had malpositioned leads in our series compared with 46% in their series. The reason for this difference could be due to improvements in surgical placement over the decade and/or the added influence of multiple target sites in their original series vs. PD and STN DBS only in our series. In addition, suboptimal stimulation settings and hardware malfunction represented the most common problem in our group, affecting 52% and 24%, respectively. This is in stark contrast to the 37% noted in the Okun et al. study.
Patients were further separated into three groups as defined by the duration of DBS stimulation to gain a better understanding of contributing factors over time. The definition of the groups was chosen by the authors to represent different stages of clinical management. The DBS optimization phase is defined as the first 12 months postsurgery as supported by DBS consensus[1] and thereafter patients were defined as entering the maintenance phase. Since both disease progression and hardware integrity is expected to play a greater role over time, the maintenance phase was divided into an early and late phase.
Analyzing the patient data in this way revealed some important findings. As expected patient selection, lead malposition, and suboptimal stimulation settings were significant factors in the earliest phase and disease progression coupled with incongruent patient expectations more prevalent in later stages of management. Of interest, stimulation side effects and subtherapeutic settings were prevalent in each of the clinical management phases regardless of whether patient was in the optimization phase or maintenance phases.
Over half (N = 26) of the patients had DBS within 2 years when benefit is expected to be robust,[4,5] yet stimulation-induced motor improvement in these patients was only 25% (mUPDRS off medication). In these patients, reprogramming led to significant and sustained improvement in motor outcomes to 48% (mUPDRS off medication) approximating expected clinical outcomes in the first 2 years. Monitoring outcomes during the optimization and early maintenance phase may prompt an evaluation for factors known to cause suboptimal outcomes. Of concern is that despite several long-term papers providing expected outcomes for STN DBS since 2003[5] and guidance for failed DBS from 2005,[8] patients continue to experience less than expected outcomes as was noted in our series of patients evaluated from 2007 and 2010 with the subtherapeutic stimulation setting as the predominant factor.
The majority of our programming changes involved strategies to reduce the field of stimulation to avoid side effects of overstimulation. Internal capsule stimulation was a noted reversible cause of worsening axial symptoms (gait, balance, and speech) where reprogramming improved axial symptoms in patients (N = 22) reporting worsening gait, balance, and speech after DBS. This finding is important since the majority of patients were self-referred and dissatisfied with therapy due primarily to problems of gait freezing, imbalance, and speech. Axial symptoms are typically nonresponsive to medication or DBS therapy and thought to be a marker of irreversible disease progression in a DBS patient. Improved axial symptoms with reprogramming was noted in each of the clinical phases including the group with longest duration DBS stimulation, highlighting the importance of threshold testing and levodopa responsiveness as valuable data in guiding long-term management.
Although our analysis was not intended to identify the root cause of suboptimal programming, there are likely many reasons that suboptimal programming was found to be the most prevalent factor in early and long-term management. Patients’ high and evolving expectations for surgery, frustrations with disease progression and nonresponsive axial symptoms prompting changes in stimulation, tendency to continue to tweak and overstimulate over time and difficulty differentiating motor symptoms from internal capsule stimulation vs. disease progression can play a role. In addition, DBS therapy in itself is complex and represents only one of a multitude of treatment decisions required to tailor treatment to an individual that and must be coordinated with medication changes, rehabilitative services, and behavioral counseling.
These findings reflect the need for greater programming expertise, which will become even more important as the number and type of implanted devices increases, indications broaden, and patient implantation years increases.
Difficulties inherent to a retrospective chart review and population biases are clear limitations of this study. Nonetheless, our experience provides valuable information that can guide long-term DBS care and serve as a lens for further study.
ACKNOWLEDGMENT
The authors thank Jay Nutt, MD, Professor of Neurology at Oregon Health and Science University, Portland Oregon, for guidance and review of the original manuscript.
Footnotes
Available FREE in open access from: http://www.surgicalneurologyint.com/text.asp?2013/4/1/69/112612
Disclaimer: The authors of this article have no conflicts of interest to disclose, and have adhered to SNI's policies regarding human/animal rights, and informed consent. Advertisers in SNI did not ask for, nor did they receive access to this article prior to publication
Contributor Information
Sierra Farris, Email: sierrafarris@gmail.com.
Monique Giroux, Email: moniquegiroux@gmail.com.
REFERENCES
- 1.Bronstein JM, Tagliati M, Alterman RL, Lozano AM, Volkmann J, Stefani A, et al. Deep brain stimulation for Parkinson disease: An expert consensus and review of key issues. Arch Neurol. 2011;68:165. doi: 10.1001/archneurol.2010.260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Castrioto A, Lozano AM, Poon YY, Lang AE, Fallis M, Moro E. Ten-year outcome of subthalamic stimulation in Parkinson disease: A blinded evaluation. Arch Neurol. 2011;68:1550–6. doi: 10.1001/archneurol.2011.182. [DOI] [PubMed] [Google Scholar]
- 3.Deep-brain stimulation for Parkinson's disease study group. Deep-brain stimulation of the subthalamic nucleus or the pars interna of the globus pallidus in Parkinson's disease. N Engl J Med. 2001;345:956–63. doi: 10.1056/NEJMoa000827. [DOI] [PubMed] [Google Scholar]
- 4.Kleiner-Fisman G, Fisman DN, Sime E, Saint-Cyr JA, Lozano AM, Lang AE. Long-term follow up of bilateral deep brain stimulation of the subthalamic nucleus in patients with advanced Parkinson disease. J Neurosurg. 2003;99:489–95. doi: 10.3171/jns.2003.99.3.0489. [DOI] [PubMed] [Google Scholar]
- 5.Krack P, Batir A, Van Blercom N, Chabardes S, Fraix V, Ardouin C, et al. Five-year follow-up of bilateral stimulation of the subthalamic nucleus in advanced Parkinson's disease. N Engl J Med. 2003;349:1925–34. doi: 10.1056/NEJMoa035275. [DOI] [PubMed] [Google Scholar]
- 6.Moro E, Poon YY, Lozano AM, Saint-Cyr JA, Lang AE. Subthalamic nucleus stimulation: Improvements in outcome with reprogramming. Arch Neurol. 2006;63:1266–72. doi: 10.1001/archneur.63.9.1266. [DOI] [PubMed] [Google Scholar]
- 7.Okun MS, Rodriguez RL, Foote KD, Sudhyadhom A, Bova F, Jacobson C, et al. A case-based review of troubleshooting deep brain stimulator issues in movement and neuropsychiatric disorders. Parkinsonism Relat Disord. 2008;14:532–8. doi: 10.1016/j.parkreldis.2008.01.001. [DOI] [PubMed] [Google Scholar]
- 8.Okun MS, Tagliati M, Pourfar M, Fernandez HH, Rodriguez RL, Alterman RL, et al. Management of referred deep brain stimulation failures: A retrospective analysis from 2 movement disorders centers. Arch Neurol. 2005;62:1250–5. doi: 10.1001/archneur.62.8.noc40425. [DOI] [PubMed] [Google Scholar]