

Abstract
Occupational exposure to silica occurs at workplaces in factories like quartz crushing facilities (silica flour milling), agate, ceramic, slate pencil, glass, stone quarries and mines, etc., Non-occupational exposure to silica dust can be from industrial sources in the vicinity of the industry as well as non-industrial sources. Recently, public concern regarding non-occupational or ambient exposure to crystalline silica has emerged making it important to gather information available on non-occupational exposures to silica dust and non-occupational silicosis. This paper reviews various non-occupational exposures reported in literature including some studies by the author. Methodology used in assessment of non-occupational exposures, standards for non-occupational exposures to silica dust and indirect estimation of cumulative risk % are also discussed.
Keywords: Non-occupational exposure, quartz, silica, silicosis
INTRODUCTION
Silica (SiO2, CAS No. 7631-86-9) is found in abundance in nature. Pure crystalline silica that is not combined with any other elements is called free silica. When combined with other elements, the compound is called silicate. Free silica occurs in different polymorphic forms like quartz, cristobalite, tridymite, and tripoli. Although identical chemically, they differ from each other in their crystal structure. Crystoballite and tridymite are products of high temperatures and may be observed in volcanic ash[1] and are rarely found in industrial samples.[2] The exposure to silica dust produces lung diseases like silicosis and silico-tuberculosis. It also increases the risk of tuberculosis, nonmalignant renal disease, and autoimmune diseases. Silica has also been classified as a carcinogen by International Agency for Research on Cancer (IARC).[3] The exposure to crystalline silica can be occupational or non-occupational.
Workers are exposed to dust containing crystalline silica for about 8 h per day and are at the risk of developing silicosis and silico-tuberculosis.
Recently, public concern regarding non-occupational or ambient exposure to crystalline silica has emerged, making it important to gather information available on non-occupational exposures and non-occupational silicosis. Non-occupational exposures are rarely estimated or measured in community environment or in the vicinity of silica-based industry. Non-occupational exposure to silica dust can be from industrial as well as nonindustrial sources. Non-occupational exposure from non-industrial sources occurs naturally due to desert dust and sand storms in hilly areas.[4,5] Some farming, construction, and demolition activities also contribute to the environmental exposure.[6] Non-occupational exposure from industrial sources occurs when dust emitted from factories like quartz crushing, agate grinding, ceramics, slate pencil, mining and milling of sand stones, silica flour milling, granite, etc., goes to the environment and people staying in the vicinity are affected.[7] Relation between occupational exposure and prevalence of silicosis and silico-tuberculosis has been established beyond doubt in many occupations.[8–11] But, there have been very few studies which suggest that there can be non-occupational silicosis also. Silicosis is a very well-established disease, but the importance of this disease has been underestimated as an environmental disease. Several cases of non-occupational silicosis from non-industrial sources have recently been reported which are summarized below.
NON-OCCUPATIONAL EXPOSURE TO SILICA DUST FROM NON-INDUSTRIAL SOURCES
Sepke[12] reported silicosis from street dust in 1961. Afterwards, Farina and Gambini[13] reported a rare case of silicosis from inhalation of desert sand. The first major study of environmental exposure to silica dust in India was reported by Saiyed et al.[5] An epidemiological survey was carried out by them to investigate the occurrence of non-occupational pneumoconiosis in central Ladakh, India, where there are no mines or industries. A total of 449 subjects were studied from three villages called Saboo, Shey, and Chushot, the prevalence of pneumoconiosis in these villages was 2.0, 20.1, and 45.3%, respectively.[5] The causative factors were suggested to be dust storms in spring and summer and an indoor air pollution but information regarding the frequency, duration and severity of dust storms, dust concentrations, particle size distributions, and the relation between soot and the pneumoconiosis is clearly lacking.[14] The disease was classified as pneumoconiosis instead of silicosis, probably due to a different interpretation when reading the chest X-ray films or due to lack of environmental data confirming silica dust exposure. Norboo et al.,[4] reported silicosis in a Himalayan village population. The Himalayan villages of Chuchot, Shamma, and Stok were surveyed because silicosis had been suspected from radiographs of some of the habitants. The villages are agricultural and Chuchot is exposed to frequent dust storms. In Chuchot, five of seven men and all the nine women examined, showed varying grades of silicosis compared with three of 13 men and seven of 11 women in Stok which lies 300 m higher and is exposed to fewer dust storms. Chemical analysis of inorganic dust in the lung showed that 54.4% was elemental silicon. This was similar to silicon content of dust collected from houses in Chuchot, which included many particles of respirable size (0.5–5 μm diameter). X-ray microanalysis showed that quartz formed 16-21% of inorganic lung dust. Franco and Massola[15] reported 6–9% quar tz in sedimented dust from the same Himalayan villages. These observations are consistent with the geological nature of Himalayan range in Ladakh.[15] In the same area, however, quartz content of 42.8% has been reported.[16] Patial[17] reported silicosis in nine males and eight females in the highlanders of a Himalayan desert and called the disease as mountain desert silicosis. Silicosis developed in these people even without working in silicosis prone workplace. He concluded that people were exposed to silica from the non-workplace silica-rich environment.
In all the above studies, cases of silicosis have been reported and the disease has been attributed to silica content in sedimented dust and/or lungs but there has been no attempt to measure silica dust (quartz) concentrations in the environment. However, there are studies where silica dust concentrations have been measured in community environment. Davis et al.,[1] reported that average quartz levels in US metropolitan areas are in the range of 1.1–8.0 μg/m3 with an average of 3.2 μg/m3. The percentage of quartz in total dichotomous mass (less than 15 μm aerodynamic equivalent diameter) varied from 2.5 to 8.2.[6]
Dust exposure is a major source of respiratory morbidity and mortality among agricultural workers.[18] In most of the developing countries farmers generally stay in the farms or in the vicinity of farms. Their dust exposures are partly occupational and partly non-occupational. In general, agricultural dusts may be divided into those of organic and inorganic origin. Organic dusts originate from plant and animal sources and are commonly the source of allergic diseases such as asthma. Inorganic dusts originate predominantly from the soil, and tend to result in non-allergic reactions in the lung.[19] Respirable quartz is found in soil dust, although weathering and chemical reactions may make it less fibrogenic than freshly fractured quartz in other operations like quarrying and sandblasting.[19,20] Silicosis has also been reported in agricultural workers. A case of silicosis was reported by Fennerty et al.,[21] in a Pakistani farmer who had been a peasant farmer in west Pakistan all his life and had worked in the fields from early childhood. Most of his time had been spent in cultivation. Results of bulk chemical analysis of the dust deposits indicated that silica content was 58.4%. The highest dust exposures occur during soil preparation activities. Tractors pulling soil preparation equipments like plowing, discing, and planing generate large dust clouds. Median total particle exposures in an open cab range from 2-20 mg/m3, but exposures up to 100 mg/m3 have been reported.[19]
The respirable fraction of dusts in tractor cabs is generally 5–40%, with total respirable concentrations commonly observed between 1 and 5 mg/m3. These exposures may be called occupational for tractor drivers, but dust generated goes to the environment and others working in the farms or residing in the vicinity of farms are also exposed. A study of dust samples from 12 farms in Alberta, Canada, found 0.8–17.5% crystalline silica.[22] Silicosis has also been reported in tractor drivers working on sandy soils on tree farms.[23]
NON-OCCUPATIONAL EXPOSURE TO SILICA DUST FROM INDUSTRIAL SOURCES
As mentioned earlier, non-occupational exposure from industrial sources occurs when dust emitted from silica-based industries goes to the environment and people staying in the vicinity are affected. There have been very few studies in the vicinity of the industry where non-occupational exposures to crystalline silica and nonoccupational silicosis have been reported[7,24–26] in slate pencil and agate industries.
Sand quarry, near California
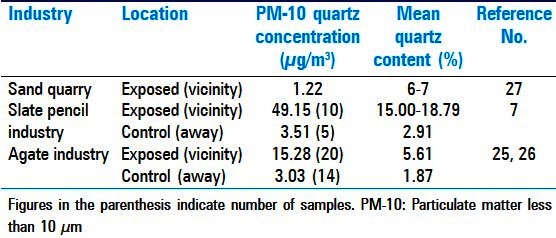
It has been mentioned by Ruble and Goldsmith[27] that Goldsmith[24] reported particulate matter less than 10 μm (PM-10) and silica levels measured at two sites near a sand quarry, near California. Mean PM-10 concentrations for sites were 18.9 and 18.2 μg/m3, and mean silica concentrations were 1.33 and 1.11 μg/m3, respectively from 6–7% silica content in the PM-10 dust. Mean silica concentration at the two sites is 1.22 μg/m3 [Table 1]. No cases of silica-related diseases were reported.
Table 1.
Non-occupational exposure to silica dust in vicinity of different industries
Slate pencil industry, India
Slate pencil industry is an unorganized small-scale industry mainly located in and around Mandsaur, Madhya Pradesh, India. A small village called Multanpura about 6 km away from Mandsaur having 6 km2 area has about 100 slate pencil manufacturing facilities. Cutting of the stone is carried out manually with electrically operated saws. The subsequent operations of collecting, sorting, and packing are carried out manually near the cutting machine. Saiyed et al.,[9] reported that total and respirable dust levels near cutting machine were 46.47 and 10.41 mg/m3, respectively. Medical survey revealed that prevalence of silicosis in this industry was 54.6%, of these 17.7% of workers had progressive massive fibrosis. Consequently, they installed local exhaust ventilation with the cutting machine in order to reduce dust concentration in the work environment. Efficacy of the dust control devices was tested by Ghodasara et al.,[28] and was reported to be 95–97%. During our visit to slate pencil industry in 2005, it was observed that dust-laden air is sucked by a fan and is thrown out in the community environment. There were no bag filters. Lot of dust is emitted from chimneys. The height of the chimney is just 10–12′ from the ground. People residing in the village are also exposed to the airborne silica dust, although they are not engaged in this occupation. Bhagia[7] reported high concentrations of quartz in ambient environment of the village using PM-10 high volume samplers and vertical elutriators. Vertical elutriators have a median cut off at 10 μm and a maximum cut off at 15 μm.[7] Dust collected by vertical elutriator was used for analyzing percentage of quartz in dust samples using Fourier transform infrared spectroscopy. The percentage of quartz was multiplied by PM-10 dust concentration to get ambient quartz concentration. The average quartz concentration in the vicinity of slate pencil industry are in the range of 41.07 to 57.22 μg/m3 at two locations within the village with an average of 49.15 μg/m3 for the village where as the quartz concentration at the control site, 5 km away from the Multanpura village is 3.51 μg/m3 [Table 1]. Prevalence of non-occupational silicosis and non-occupational silico-tuberculosis in the vicinity (exposed sites) was reported to be 12.6 and 6.3%, respectively.[29]
Agate industry, India
Agate industry has been developed primarily as a cottage or household industry mainly located in and around Khambhat, Gujarat, India. Grinding and polishing of agate puts it in semiprecious category of ornamental stones. A variety of articles like necklaces, earrings, cufflinks, key chains, ashtrays, etc., are made from agate. The process of making necklaces and other decorative articles includes baking of the stones, chipping of stones, grinding, and polishing. Amongst various processes, agate grinding activity, where the agate beads are ground against the rotating emery wheel, generates lots of silica dust in the work environment. During the preliminary visits, it was observed that this dust not only pervades the work environment, but also the community environment. Consequently, the family members of the house where agate grinding activities are carried out and the people residing in the vicinity are also exposed to the airborne silica dust, although they are not engaged in this occupation.
An epidemiological study in agate industry carried out by Sadhu et al.,[11] showed that the prevalence of silicosis was 40.7% in agate workers. Environmental hygiene survey[30] also showed that dust concentrations in the work environment were much higher than the permissible exposure limits. Bhagia et al.,[26] also reported high dust concentrations in agate grinding operations. These observations motivated National Institute of Occupational Health (NIOH) to measure non-occupational exposure to silica dust in the vicinity of agate industry.
Bhagia et al.,[25,26] reported ambient air pollution study with the objectives of assessing quartz concentrations in the vicinity of agate industry. Four sites in the vicinity of agate industry, namely, Shakarpur, Hajju fajju no mohallo, Vadva-metpur and Bhoi-bari were selected as exposed sites. In addition to exposed sites, one locality in the city called Nareshwar, which was away from these units was also selected as a control site in the city. The other two control sites, Rohini and Pandad villages, where epidemiological study was carried out for control subjects were 10–15 km away from Khambhat.
People living in the vicinity of agate industry are exposed to an average 24 h crystalline silica (quartz) concentration of 15.28 μg/m3, whereas in control localities, away from agate industry, they are exposed to an average crystalline silica concentration of 3.03 μg/m3 [Table 1]. No cases of non-occupational silicosis were reported from control sites.[26] Prevalence of non-occupational silicosis and non-occupational silico-tuberculosis was reported to be 5.8 and 2.4%, respectively.[26]
AMBIENT AIR QUALITY STANDARDS FOR SILICA
National ambient air quality standards (NAAQS) for suspended particulate matter (PM-10) are stated in terms of 24-h average concentrations with a primary standard of 150 μg/m3 and a secondary standard of 50 μg/m3.[6,31] Central Pollution Control Board (CPCB, India, 1994)[32] standard based on 24-h PM-10 dust concentration is 100 μg/m3 for residential localities. Although there is no ambient air quality standard for crystalline silica, Environmental Protection Agency (EPA)[6,33] suggested interim annual air quality standard (IAAQS).[6,33] EPA concluded that “for healthy individuals not compromised by other respiratory ailments and for ambient environments expected to contain less than 10% crystalline silica fraction in PM-10, the maintenance of 50 μg/m3 annual NAAQS for PM-10 should be adequate to protect against the silicotic effects from ambient crystalline silica exposures”. This standard was based upon average ambient concentrations of silica in United States and risk was calculated by converting ambient exposures to equivalent occupational exposures.[6] No epidemiological studies were carried out in the community to derive the standards. Considering a maximum of 10% silica in dust, an interim standard of 5 μg/m3 for ambient silica can be assumed. The most important and common observation in the vicinity of agate and slate pencil industries [Table 1] is that the quartz concentrations in exposed localities are more than 5 μg/m3 and in the control localities quartz concentrations are less than 5 μg/m3.
INDIRECT ESTIMATION OF CUMMULATIVE RISK PERCENTAGE
The comparison of interim standard of 5 μg/m3 for quartz[6] (EPA) with our observations suggest that ambient exposure to quartz in the vicinity of agate and slate-pencil industries poses potential risk of silicosis. For derivation of ambient air quality standard for crystalline silica EPA[6] used a method, which converts ambient exposures to the equivalent occupational exposures. Cumulative risk (%) can then be computed from graphs of cumulative risk percentage vs cumulative silica exposures. People living in the vicinity of agate industry are exposed to an average 24-h crystalline silica (quartz) concentration of 15.28 μg/m3, whereas in control localities they are exposed to an average crystalline silica concentration of 3.03 μg/m3 [Table 1]. Relation between continuous and occupational exposures[6] is defined by Continuous exposure = TWA occupational exposures × (5 days/7 days) × (10 m3 air breathed at work/20 m3 total air breathed in a day).
The occupational equivalents of exposure of 15.28 and 3.03 μg/m3 in exposed and controlled localities using above equation are 0.042 and 0.0084 mg/m3, respectively for agate industry. A 70-year exposure to these occupational equivalents would result in cumulative silica exposures of 2.94 mg/m3 × years and 0.59 mg/m3 × years for exposed and control localities, respectively. Cumulative risk (%) for these values was computed by log-logistic cumulative risk model of Hnizdo and Sluis-Cremer,[8] which is represented by following equation:
F (CD) =1 − [1 + CD1/δ × exp (−μ/δ)]−1
Where, CD = cumulative dose, μ = 1.298, and δ = 0.2111[6]
The cumulative risk (%) for exposed and control localities computed from above equation was found to be 26.11 and 0.02%, respectively for agate industry. Similarly, risk % for slate pencil industry was found to be 99 and 0.04% for exposed and control sites, respectively. The cumulative risk for an ambient exposure to 5 μg/m3 (an interim air quality standard for silica, based on findings of EPA) was 0.33%.
DISCUSSION
Computation of cumulative risk is only an approximation because cumulative risk (%) depends on many factors such as silica particle size distribution in PM-10 dust, surface properties, and sources of quartz. EPA[6] derived the standard for ambient silica exposures by converting ambient exposures to occupational exposures. The curve for cumulative risk (%) versus cumulative silica exposure was used by EPA,[6] which was based upon respirable dust (≤5 μm). The concentration of silica in ambient dust is generally higher in large size fractions in the range of 2.5-15 μm and in dust fractions less than 2.5 μm.[1,6] Others like Buckman and Brandy,[34] and Ruble and Goldsmith[27] also reported that particulates greater than 10 μm contain more silica than particulates having diameters less than 10 μm. This may be so because quartz is harder than most minerals and does not disintegrate to fine particles easily as reported by Ayer.[35] This may be the reason why cases of silicosis are not reported from metropolitan cities of USA. But in the vicinity of silica-based industry; quartz comes from crushing, cutting, and grinding operations. The total airborne dust collected from work environment of agate industry was analyzed for particle size. It was found that 90% of the particles are having diameters less than 5 μm.[25,26] These particles get dispersed in the vicinity of agate industry. This is in contrast to the natural dust in which percentage of fine quartz particles is less. To certain extent, it justifies the conversion of ambient exposures to occupational exposures by EPA[6] in estimating risk in the vicinity of silica-based industry because cumulative occupational exposures are based upon respirable dust (≤5 μm). Secondly, airborne quartz in the vicinity of agate and slate pencil industry is freshly fractured. It has been reported that freshly fractured silica is much more cytotoxic than aged quartz.[6,36,37] Considering all these arguments, a question arises whether there should be separate silica standard for community environment (non-occupational exposure to silica dust from nonindustrial sources) and the environment in the vicinity of industry emitting silica particles (non-occupational exposure to silica dust from industrial sources).
Another question is whether the standard should be based on PM-10 dust or it should be based on respirable dust (less than 4 or 5 μm) or PM-2.5 because silicosis is the restrictive type of lung disease. Hearl[38] suggested the use of industrial hygiene techniques for measurement of crystalline silica in ambient environment. Bhagia[7] used PM-10 high volume samplers (1,100 liter per minute (LPM)) and vertical elutriators with median cutoff at 10 μm and a maximum cutoff at 15 μm (7.4 LPM) for measurement of silica in the vicinity of slate and agate industries. Davis et al.,[1] used dichotomous samplers with a maximum cutoff at 15 μm. The manual dichotomous sampler (16.7 LPM) is used for routine compliance monitoring in USA for PM-10 and PM-2.5. To answer all the questions discussed above, lot of field studies are required with simultaneous monitoring of PM-10, PM-2.5, and respirable dust (less than 4 or 5 μm) in the vicinity of silica-based industry as well as in the community environment. Our observations [Table 1] show that quartz concentrations (PM-10) in the vicinity of agate and slate pencil industries are more than 5 μg/m3, while in control localities away from these industries are less than 5 μg/m3. For the time being, an interim ambient air quality standard of 5 μg/m3 for silica with PM-10 measurement with a cumulative risk of 0.33% appears reasonable.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Davis BL, Johnson LR, Stevens RK, Courtney WJ, Safriet DW. The quartz content and elemental composition of aerosols from selected sites of the EPA inhalable particulate network. Atmos Environ. 1984;18:771–82. [Google Scholar]
- 2.NIOSH. National Institute of Occupational Safety and Health, Manual of Analytical Methods; Method 7602, Silica Crystalline by IR. 4th. Atlanta: Centers for Disease Control and Prevention; 1994. [Google Scholar]
- 3.IARC. International agency for research on Cancer Monographs on the Evaluation of Carcinogenic Rrisks to Humans: Silica, Some Silicates, Coal Dust and Para-Ararmid Fibrils. vol. 68. Lyon, France: WHO, International Agency for Research on Cancer; 1997. [Google Scholar]
- 4.Norboo T, Angchuk PT, Yahya M, Kamat SR, Pooley FD, Corrin B, et al. Silicosis in a Himalayan village population: Role of environmental dust. Thorax. 1991;46:341–3. doi: 10.1136/thx.46.5.341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Saiyed HN, Sharma YK, Sadhu HG, Norboo T, Patel PD, Patel TS, et al. Non-occupational pneumoconiosis at high altitude villages in central Ladakh. Br J Ind Med. 1991;48:825–9. doi: 10.1136/oem.48.12.825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.U. S. Environmental Protection Agency. Ambient levels and noncancer health effects of inhaled crystalline and Amorphous silica: Health issue assessment. Triangle Park: US EPA; 1996. EPA/600/R-95/115: Chapter 1. [Google Scholar]
- 7.Bhagia LJ. Non-occupational exposure to silica dust in vicinity of slate pencil industry, India. Environ Monit Assess. 2009;151:477–82. doi: 10.1007/s10661-008-0290-x. [DOI] [PubMed] [Google Scholar]
- 8.Hnizdo E, Sluis-Cremer GK. Risk of silicosis in a cohort of South African gold miners. Am J Ind Med. 1993;24:447–57. doi: 10.1002/ajim.4700240409. [DOI] [PubMed] [Google Scholar]
- 9.Saiyed HN, Parikh DJ, Ghodasara NB, Sharma YK, Patel GC, Chatterjee SK, et al. Silicosis in slate-pencil workers: I. An environmental and medical study. Am J Ind Med. 1985;8:127–33. doi: 10.1002/ajim.4700080207. [DOI] [PubMed] [Google Scholar]
- 10.Jiang CQ, Xiao LW, Lam TH, Xie NW, Zhu CQ. Accelerated silicosis in workers exposed to agate dust in Guangzhou, China. Am J Ind Med. 2001;40:87–91. doi: 10.1002/ajim.1074. [DOI] [PubMed] [Google Scholar]
- 11.Sadhu HG, Parikh DJ, Sharma YK, Saiyed HN, Rao PV, Kulkarni PK, et al. A follow up study of health status of small-scale agate industry workers. Indian J Ind Med. 1995;41:101–5. [Google Scholar]
- 12.Sepke G. Silicosis from street dust. Z Gesamte Hyg. 1961;7:833–7. [Google Scholar]
- 13.Farina G, Gambini G. A rare case of silicosis from inhalation of desert sand. Med Lav. 1968;59:281–6. [PubMed] [Google Scholar]
- 14.Ranavaya MI, Reger RB, Battigelli MC. Non-occupational pneumoconiosis at high altitude villages in central Ladakh. Br J Ind Med. 1992;49:452–3. doi: 10.1136/oem.49.6.452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Franco G, Massola A. Correspondence. Occup Environ Med. 1992;49:452–3. [Google Scholar]
- 16.Gaetani M, Casnedi R, Fois E, Garzanti E, Jadoul F, Nicora A, et al. Stratigraphy on the tethys himalaya in Zanskar, Ladakh. Riv It Paleont Strat. 1986;91:443–78. [Google Scholar]
- 17.Patial RK. Mountain desert silicosis. J Assoc Physicians India. 1999;47:503–4. [PubMed] [Google Scholar]
- 18.Schenker MB. Respiratory health hazards in agriculture. Am J Respir Crit Care Med. 1998;158(5 Pt 2):S1–76. doi: 10.1164/ajrccm.158.supplement_1.rccm1585s1. [DOI] [PubMed] [Google Scholar]
- 19.Schenker M. Exposures and health effects from inorganic agricultural dusts. Environ Health Perspect. 2000;108(Suppl 4):661–4. doi: 10.1289/ehp.00108s4661. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Castranova V, Dalal NS, Vallyathan V. Role of surface free radicals in the pathogenicity of silica. In: Castranova V, Vallyathan V, Wallace WE, editors. Silica and Silica-Induced Lung Disease. Boca Raton: CRC Press; 1996. pp. 91–105. [Google Scholar]
- 21.Fennerty A, Hunter AM, Smith AP, Pooley FD. Silicosis in a Pakistani farmer. Br Med J (Clin Res Ed) 1983;287:648–9. doi: 10.1136/bmj.287.6393.648-a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Green FH, Yoshida K, Fick G, Paul J, Hugh A, Green WF. Characterization of airborne mineral dusts associated with farming activities in rural Alberta, Canada. Int Arch Occup Environ Health. 1990;62:423–30. doi: 10.1007/BF00379058. [DOI] [PubMed] [Google Scholar]
- 23.Dynnik VI, Khizhniakova LN, Baraneko AA, Makotchenko VM, Okseniuk IM. Silicosis in tractor drivers working on sandy soils on tree farms. Gig Tr Prof Zabol. 1981;12:26–8. [PubMed] [Google Scholar]
- 24.Goldsmith DF. Quail Hollow Special Investigation. Monterey Bay Air Pollution Control District. Davis, CA: University of California, Division of Occupational and Environmental Medicine; 1991. May 30, [Google Scholar]
- 25.Bhagia LJ, Parikh DJ, Saiyed HN. Ambient silica monitoring in vicinity of agate industry, Khambhat, India. Indian J Occup Hyg Safety. 2007;1:6–10. [Google Scholar]
- 26.Bhagia LJ, Sadhu HG, Parikh DJ, Karnik AB, Saiyed HN. Prevention, Control and Treatment of Silicosis and Silico-Tuberculosis in Agate Industry Report submitted by National Institute of Occupational Health, Ahmedabad to Indian Council of Medical Research and the Ministry of Health and Family welfare, Government of India. 2004 [Google Scholar]
- 27.Ruble R, Goldsmith DF. Ambient PM10 emissions: Contributions and impact on silica emissions. J Expo Anal Environ Epidemiol. 1997;7:327–44. [PubMed] [Google Scholar]
- 28.Ghodasara NB, Rathod RA, Sathwara NG, Saiyed HN, Parikh DJ, Kashyap SK. Environmental dust hazards and its control in small scale slate pencil industry. Indian J Environ Protect. 1992;12:50–3. [Google Scholar]
- 29.Tiwari RR, Bhagia LJ, Sharma YK. Health risk assessment and development of intervention programme in cottage industries with high risk of silicosis: A study among slate pencil workers in Mandsaur. Report submitted by National Institute of Occupational Health, Ahmedabad to Indian Council of Medical Research and the Ministry of Health and Family Welfare, Government of India [Google Scholar]
- 30.Ghodasara NB, Rathod RA, Pandya GL, Saiyed HN, Parikh DJ, Kashyap SK. Environmental dust exposure study in agate grinding units. Indian J Environ Protect. 1997;17:124–7. [Google Scholar]
- 31.Code of Fedral Regulations. National primary and secondary air quality standards of particulate matter, CFR 40. 1991 [Google Scholar]
- 32.CPCB: Central Pollution Control Board, India. National Ambient Air Quality Standards, No. 252. 1994 May 20; [Google Scholar]
- 33.Gift JS, Faust RA. Noncancer inhalation toxicology of crystalline silica: Exposure-response assessment. J Expo Anal Environ Epidemiol. 1997;7:345–58. [PubMed] [Google Scholar]
- 34.Buckman H, Brandy N. The Nature and Properties of Soil. 7th. New York: Macmillan; 1969. [Google Scholar]
- 35.Ayer HE. The proposed ACGIH mass limits for quartz: Review and evaluation. Am Ind Hyg Assoc J. 1969;30:117–25. doi: 10.1080/00028896909343096. [DOI] [PubMed] [Google Scholar]
- 36.Vallyathan V. Generation of oxygen radicals by minerals and its correlation to cytotoxicity. Environ Health Perspect. 1994;102(Suppl 10):111–5. doi: 10.1289/ehp.94102s10111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Vallyathan V, Shi XL, Dalal NS, Irr W, Castrinova V. Generation of free radicals from freshly fractured silica dust. Potential role in acute silica-induced lung injury. Am Rev Respir Dis. 1988;138:1213–9. doi: 10.1164/ajrccm/138.5.1213. [DOI] [PubMed] [Google Scholar]
- 38.Hearl FJ. Industrial hygiene sampling and applications to ambient silica monitoring. J Expo Anal Environ Epidemiol. 1997;7:279–89. [PubMed] [Google Scholar]