

Abstract
Background:
The aim of the present study was to assess which modifiable, non-modifiable, and socioeconomic factors are good predictors for cardiovascular risk in overweight and obese Iranian women.
Materials and Methods:
This clinical cross-sectional study was conducted on 811 overweight and obese women of age 20–60 years in Islamic Republic of Iran. In this study, the dependent variables were fasting blood sugar (FBS) and lipid profile, and the independent variables were educational level, waist to hip ratio (WHR), body mass index (BMI), waist circumference (WC), age, fasting glycemia, and diabetes.
Results:
Univariate analysis showed that the significant factors associated with FBS were age, BMI, education, and WHR, but the effect of age was more than that of others. For total cholesterol (TC), only glycemia had a significant effect [P = 0.004, odds ratio (OR) 1.9 vs. others independent variables’ ORs]. Having diabetes, BMI ≥30 kg/m2, and education ≤12 years were the significant factors associated with triglyceride (TG), but the effect of diabetes was more than that of others (OR: 2.7, 2.2, and 1.9 for diabetes, BMI, and education, respectively). The effect of age was more than that of other independent factors on low density lipoprotein-cholesterol (LDL-C). There was not any significant association between independent variables and high density lipoprotein-cholesterol (HDL-C) in multiple logistic regression models.
Conclusion:
Based on the obtained results, in clinic, for overweight and obese women, age, glycemia, and having diabetes can be considered as predictors for FBS, and LDL-C, TC, and TG, respectively.
Keywords: Cardiovascular risk factors, Iran, modifiable, non-modifiable, socioeconomic, women
INTRODUCTION
One of the health concerns in developing countries as well as developed countries is the increasing challenges about overweight and obesity which are related to some cardiovascular risk factors. The results of some studies have shown that modifiable, non-modifiable, and some socioeconomic factors such as age, education, obesity, glycemia, and diabetes may affect the lipid profile and fasting blood sugar (FBS), although other researches did not report the same evidence.
Some studies have indicated an inverse relation of level of education with FBS and lipid profile,[1,2] but other studies could not find such a correlation.[3]
The results of some studies have shown that central adiposity has a greater effect on total cholesterol (TC) and low density lipoprotein-cholesterol (LDL-C) among women than body mass index (BMI).[4] On the other hand, Orsatti et al. reported that only waist to hip ratio (WHR) is significantly associated with dysglycemia, hypertriglyceridemia, and decreased high density lipoprotein-cholesterol (HDL-C).[5] Other reports emphasize on the association of waist circumference (WC) or BMI and WHR with serum lipid levels as a main parameter.[6,7] It must be emphasized that this kind of study in the view of being a good predictor between modifiable, non-modifiable, and socioeconomic factors for predicting the cardiovascular disease risk factors at clinic in overweight and obese women is scarce too.[8–10]
The result of Erem et al.'s study has shown that the prevalence of high TC, LDL-C, triglyceride (TG), and TC/HDL-C ratio increased with age.[2]
There is also some data about the correlation of glycemia and diabetes with lipid profile. Vijayakumar has shown that diabetes mellitus (DM) was significantly associated with hypercholesterolemia.[11] The study of Sadeghi et al. has shown that serum lipids were higher in people with DM and impaired glucose tolerance test (IGTT), especially in females.[12]
Keeping in consideration the data scarcity and controversy, we attempted to evaluate which modifiable, non-modifiable, and socioeconomic factors have more effect on lipid profiles and FBS in overweight and obese Iranian women. As women are at greater risk of obesity than men in the population,[13,14] we conducted our project on overweight and obese women. It must be emphasized that this kind of study in the view of being a good predictor between modifiable, non-modifiable, and socioeconomic factors for predicting the cardiovascular disease risk factors at clinic in overweight and obese women is scarce too.
MATERIALS AND METHODS
Study subjects and geographic area
This clinical cross-sectional study was conducted in women who were referred to two nutrition clinics at Zahedan, Iran. This city is the center of Sistan and Baluchestan province and located in the southeast of Iran. The subjects were 811 women of age between 20 and 60 years. The center gets patients referred from different parts of the province. Data collected for each subject included age, weight, height, waist and hip circumferences, level of education, glycemia, diabetes, and lipid profiles. The subjects gave verbal consent for participation in this study.
Anthropometric measurements
BMI was considered as general obesity index, and WC and WHR were considered as central obesity indices. These measurements were made in accordance with World Health Organization (WHO) standards.[15]
Inclusion and exclusion criteria
Based on WHO standard for BMI (underweight: BMI < 18.5 kg/m2; normal: BMI 18.5–24.9 kg/m2; overweight: BMI 25.0–29.9 kg/m2; obese: BMI ≥ 30 kg/m2),[16] women with BMI between 25 and 29.9 kg/m2 classified as overweight and between ≥30 and 39.9 kg/m2 classified as obese were included in the study. Men, subjects of age below 20 years or more than 60 years, those with BMI less than 25 and ≥40 kg/m2, and pregnant women were excluded from study.
Evaluation of lipid profiles, FBS, and educational level
Lipid profile (TC, TG, HDL-C) and FBS were determined by the usual laboratory tests after 12-h overnight fasting. LDL-C was calculated according to the Friedewald equation.[17] Data analysis also included two levels of education: 1–12 years of schooling and more than 12 years of schooling.
In this study, the following criteria were used as cutoffs (threshold) for the variables used: ≥30 kg/m2, ≥88 cm, ≥0.85, ≥200 mg/dl, ≥200 mg/dl, ≥130 mg/dl, <35 mg/dl, 100 mg/dl, and 126 mg/dl for BMI, WC, WHR, TC, TG, LDL-C, HDL-C, fasting glycemia, and diabetes, respectively.[16]
Statistical analysis
All statistical analyses were performed using SPSS/PC statistical program (version 16 for Windows). The results are presented as mean ± standard deviation. Student's t-test was used for comparison of differences between two groups as univariate analysis. To control the potential confounders, multiple logistic regression was used to find the association between binary dependent variables (FBS, TC, TG, LDL-C, and HDL-C) and independent variables (educational level, age, BMI, WC, WHR, fasting glycemia, and diabetes). Normality of data was checked using Shapiro–Wilk test. Odds Ratios (ORs) and the 95% Confidence Intervals (CIs) were also estimated, and P values <0.05 were considered significant.
RESULTS
The characteristics of subjects showed that the mean and standard deviation of the independent variables, i.e. education, WHR, BMI, WC, and age, were 11.2 ± 4.1 years, 0.99 ± 2.3, 33.9 ± 5.6 kg/m2, 101.6 ± 14.5 cm, and 33.3 ± 8.9 years, respectively. The mean and standard deviation of the dependent variables, i.e. FBS, TC, TG, LDL-C, HDL-C, TC/HDL-C, and LDL/HDL-C were 98.9 ± 47.3 mg/dl, 195.6 ± 42.7 mg/dl, 149 ± 79.7 mg/dl, 119.5 ± 36.8 mg/dl, 48.5 ± 28.6 mg/dl, 4.3 ± 2.1, and 2.6 ± 1.2, respectively.
FBS, TC, and TG were significantly higher in subjects aged ≥40 years compared to subjects <40 years old (118.7 ± 91.1 mg/dl vs. 94.1 ± 25.1 mg/dl, P < 0.000; 204.8 ± 43 mg/dl vs. 193.3 ± 42.2 mg/dl, P < 0.002; and 174.5 ± 85 mg/dl vs. 142.7 ± 76.9 mg/dl, P < 0.000 for FBS, TC, and TG, respectively). For HDL-C and LDL-C, such significant differences were not observed [Table 1].
Table 1.
Mean and standard deviation of FBS and lipid profile on the basis of age

Women with higher educational level had significantly lower FBS, TC, and TG. There were no significant differences for HDL-C and LDL-C between the two educational levels.
Mean and standard deviation of FBS and lipid profile on the basis of fasting glycemia and diabetes are presented in Tables 2 and 3, respectively.
Table 2.
Mean and standard deviation of FBS and lipid profile on the basis of fasting glycemia
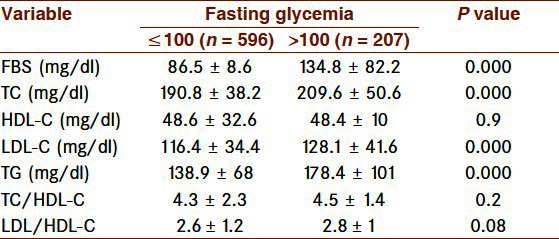
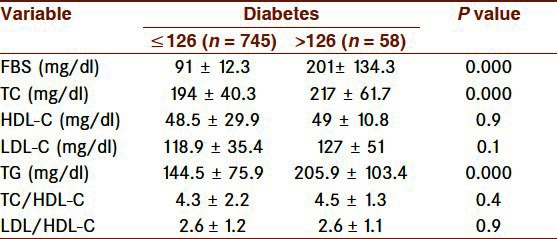
Table 3.
Mean and standard deviation of FBS and lipid profile on the basis of diabetes
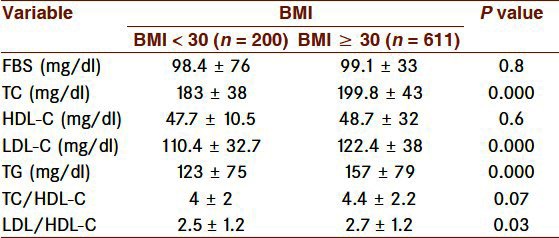
TC, LDL-C, and TG were significantly higher in the women with higher BMI than those with low BMI (199.8 ± 43 mg/dl vs. 183 ± 38 mg/dl, P < 0.000; 122.4 ± 38 mg/dl vs. 110.4 ± 32.7 mg/dl, P < 0.000; and 157 ± 79 mg/dl vs. 123 ± 75 mg/dl, P < 0.000 for TC, LDL-C, and TG, respectively). No such significant differences were obtained for FBS and HDL-C [Table 4]. The same results were also obtained for waist circumference index.
Table 4.
Mean and standard deviation of FBS and lipid profile on the basis of BMI
The women with high WHR had significantly high FBS, TC, TG, and LDL-C than those with normal WHR.
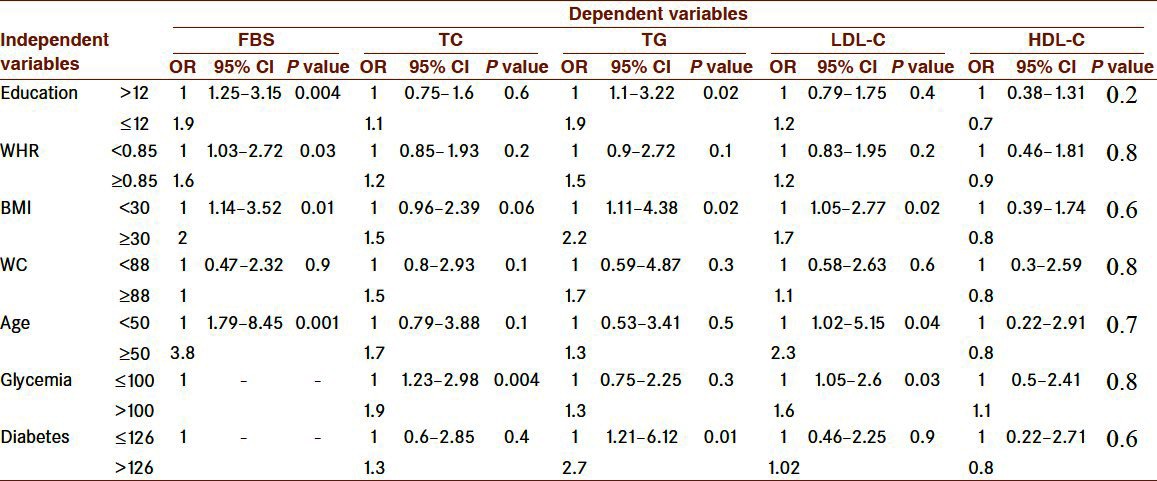
Logistic regression model between dependent and independent variables is shown in Table 5. Significant factors associated with FBS were age, BMI, education, and WHR, but the effect of age was more than that of others. For TC, only glycemia as an independent factor had a significant effect (P = 0.004, OR 1.9 vs. others independent variables’ ORs). Having diabetes, BMI ≥30 kg/m2, and education ≤12 years were significant factors associated with TG, but the effect of diabetes was more than that of others (OR: 2.7, 2.2, and 1.9 for diabetes, BMI, and education, respectively). Although age, BMI, and glycemia as independent factors had significant association with LDL-C, the effect of age was more than that of others (OR: 2.3, 1.7, and 1.6 for age, BMI, and glycemia, respectively). There was not any significant association between independent variables and HDL-C in multiple logistic regression models.
Table 5.
Logistic regression model between dependent and independent variables
DISCUSSION
The primary objective of the present study was to examine which modifiable, non-modifiable, and socioeconomic factors have more effect on lipid profiles and FBS in overweight and obese Iranian women. Our findings suggest that age, glycemia, and having diabetes have more effect than the other independent variables (education, BMI, WC, WHR) on FBS, and LDL-C, TC, and TG, respectively. Logistic regression model did not show any significant association between independent variables and HDL-C.
FBS, TC, and TG were significantly higher in subjects aged ≥40 years compared to subjects <40 years old, which is consistent with the reports from Iran[18] and other counties.[2] Iranian women are in good shape and have normal weight before they get married. This situation changes after marriage. Iranian food patterns (using greasy foods a lot), lack of physical activity between Iranian people especially among women,[19] higher number of parity in Sistan and Baluchestan women than in women from other parts of Iran,[20] and some physiological factors like decreasing estrogen after menopause age[21] can support these results observed after 40 years of age.
In the present study, women with higher education level were observed to have significantly lower FBS, TC, and TG. This inverse relationship is supported by other studies,[1,2] although there are some data contrary to this result.[3] The result of another study has shown that physical activity may increase by employment and working out, and on the other hand, having a better educational level may cause to get reducing diet or take other ways to weight loss comparable to women with low level of education.[22] Because there are many governmental and private universities in Sistan and Baluchestan province now than in the last two decades, the women have more access to university for improving and developing their educational level.
As reported in other studies,[11,12] TC, TG, and FBS were significantly higher in increased FBS and diabetic groups compared to normal ones [Tables 2 and 3]. Sistan and Baluchestan people, like in other parts of Iran,[23] used to take foods of high energy density. Carbohydrate diet, especially some kinds of local breads (Taftoon and Lavash), constitute the main source of energy of Sistan and Balouchestan subjects. The above-mentioned local breads are energy dense and nearly all the people who live in this part of Iran used to take it with all daily meals. On the other hand, Sistan and Baluchestan subjects used to drink tea a lot (more than six glasses per day) with high amount of cubic sugar (at least 5–6 cubic sugar with each class of tea).
In the present study, except for HDL-C, nearly all the lipid profile variables and FBS were significantly higher in high BMI, high WC, and high WHR groups compared to other groups. This order of magnitude is in line with the results of other studies also.[24,25] It must be mentioned that most men and women, especially women, like to be obese indeed in this part of Iran. On the other hand, because of religious and cultural factors, most of the Sistan and Baluchestan women do not go to gym for physical activity, eat large meals for lunch and dinner (especially dinner), and use lot a of fatty food as meals.
In conclusion, in view of the obtained results, in clinic, for overweight and obese women, age, glycemia, and having diabetes can be considered as predictors of FBS, and LDL-C, TC, and TG, respectively. Further studies are needed to clarify this.
LIMITATION
People of different races are living in this province, and so there may be various kinds of genetic polymorphism. We could not evaluate this, which is one of the limitations of the study.
ACKNOWLEDGMENT
Our thanks go to all who participated actively in this project.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Maddah M. Association of gender and education with blood lipids and fasting glucose levels in a sample of Iranian obese adults. Int J Cardiol. 2007;120:281–3. doi: 10.1016/j.ijcard.2006.07.201. [DOI] [PubMed] [Google Scholar]
- 2.Erem C, Hacihasanoglu A, Deger O, Kocak M, Topbas M. Prevalence of dyslipidemia and associated risk factors among Turkish adults: Trabzon lipid study. Endocrine. 2008;34:36–51. doi: 10.1007/s12020-008-9100-z. [DOI] [PubMed] [Google Scholar]
- 3.Narksawat K, Podhipak A, Punyaratabundhu P, Podang J. Atheromatous risk factors among Thai labor forces by socioeconomic status. J Med Assoc Thai. 2003;86:655–65. [PubMed] [Google Scholar]
- 4.Njelekela MA, Negishi H, Nara Y, Sato T, Tomohiro M, Kuga S, et al. Obesity and lipid profiles in middle aged men and women in Tanzania. East Afr Med J. 2002;79:58–64. doi: 10.4314/eamj.v79i2.8901. [DOI] [PubMed] [Google Scholar]
- 5.Orsatti FL, Nahas EA, Nahas-Neto J, Maesta N, Orsatti CL, Vespoli Hde L, et al. Association between anthropometric indicators of body fat and metabolic risk markers in post-menopausal women. Gynecol Endocrinol. 2010;26:16–22. doi: 10.3109/09513590903184076. [DOI] [PubMed] [Google Scholar]
- 6.Moreira-Andrés MN, del Cañizo-Gómez FJ, Losa MA, Ferrando P, Gómez de la Cámara A, Hawkins FG. Comparison of anthropometric parameters as predictors of serum lipids in premenopausal women. J Endocrinol Invest. 2004;27:340–7. doi: 10.1007/BF03351059. [DOI] [PubMed] [Google Scholar]
- 7.Oliveira MA, Fagundes RL, Moreira EA, Trindade EB, Carvalho TD. Relation between anthropometric indicators and risk factors for cardiovascular disease. Arq Bras Cardiol. 2010;94:478–85. doi: 10.1590/s0066-782x2010005000012. [DOI] [PubMed] [Google Scholar]
- 8.Chehrei A, Sadrnia S, Keshteli AH, Daneshmand MA, Rezaei J. Correlation of dyslipidemia with waist to height ratio, waist circumference, and body mass index in Iranian adults. Asia Pac J Clin Nutr. 2007;16:248–53. [PubMed] [Google Scholar]
- 9.Ko GT, Chan JC, Woo J, Lau E, Yeung VT, Chow CC, et al. Simple anthropometric indexes and cardiovascular risk factors in Chinese. Int J Obes Relat Metab Disord. 1997;21:995–1001. doi: 10.1038/sj.ijo.0800508. [DOI] [PubMed] [Google Scholar]
- 10.Dalton M, Cameron AJ, Zimmet PZ, Shaw JE, Jolley D, Dunstan DW, et al. AusDiab Steering Committee. Waist circumference, waist-hip ratio and body mass index and their correlation with cardiovascular disease risk factors in Australian adults. J Intern Med. 2003;254:555–63. doi: 10.1111/j.1365-2796.2003.01229.x. [DOI] [PubMed] [Google Scholar]
- 11.Vijayakumar G, Arun R, Kutty VR. High prevalence of type 2 diabetes mellitus and other metabolic disorders in rural Central Kerala. J Assoc Physicians India. 2009;57:563–7. [PubMed] [Google Scholar]
- 12.Sadeghi M, Roohafza H, Shirani S, Poormoghadas M, Kelishadi R, Baghaii A, et al. Diabetes and associated cardiovascular risk factors in Iran: the Isfahan Healthy Heart Programme. Ann Acad Med Singapore. 2007;36:175–80. [PubMed] [Google Scholar]
- 13.Musaiger AO, Al-Mannai MA. Weight, height, body mass index and prevalence of obesity among the adult population in Bahrain. Ann Hum Biol. 2001;28:346–50. doi: 10.1080/030144601300119151. [DOI] [PubMed] [Google Scholar]
- 14.Erem C, Yildiz R, Kavgaci H, Karahan C, Deger O, Can G, et al. Prevalence of diabetes, obesity and hypertension in a Turkish population (Trabzon city) Diabetes Res Clin Pract. 2001;54:203–8. doi: 10.1016/s0168-8227(01)00320-5. [DOI] [PubMed] [Google Scholar]
- 15.Azizi F, Allahverdian S, Mirmiran P, Rahmani M, Mohammadi F. Dietary factors and body mass index in a group of Iranian adolescents: Tehran lipid and glucose study-2. Int J Vitam Nutr Res. 2001;71:123–7. doi: 10.1024/0300-9831.71.2.123. [DOI] [PubMed] [Google Scholar]
- 16.Lysen LK, Israel DA. Nutrition in weight management. In: Mahan LK, Escott Stump, Raymond JL, editors. Krause's Food and the Nutrition Care Process. 13th ed. USA: W. B Saunders Co; 2012. pp. 462–488. Appendix 30, p. 1082-98. [Google Scholar]
- 17.Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem. 1972;18:499–502. [PubMed] [Google Scholar]
- 18.Boshtam M, Rafiei M, Sarraf-Zadegan N. Obesity and its association with other cardiovascular risk factors in Isfahan population: Isfahan CVD risk factor survey. Atherosclerosis. 1997;1:7–11. [Google Scholar]
- 19.Esmaillzadeh A, Azadbakht L. Food intake patterns may explain the high prevalence of cardiovascular risk factors among Iranian women. J Nutr. 2008;138:1469–75. doi: 10.1093/jn/138.8.1469. [DOI] [PubMed] [Google Scholar]
- 20.Jamshidbygi A. Iranian Behvarz Journal. no. 54, spring 82. I.R.Iran: published by Ministry of Health; Iran vital zyje and its outcomes in 1380; p. 15. [Google Scholar]
- 21.Davidson MH, Maki KC, Karp SK, Ingram KA. Management of hypercholesterolaemia in postmenopausal women. Drugs Aging. 2002;19:169–78. doi: 10.2165/00002512-200219030-00002. [DOI] [PubMed] [Google Scholar]
- 22.Serdula MK, Collins ME, Williamson DF, Anda RF, Pamuk E, Byers TE. Weight control practices of U.S. adolescents and adults. Ann Intern Med. 1993;119:667–71. doi: 10.7326/0003-4819-119-7_part_2-199310011-00008. [DOI] [PubMed] [Google Scholar]
- 23.Esmaillzadeh A, Azadbakht L. Dietary energy density and the metabolic syndrome among Iranian women. Eur J Clin Nutr. 2011;65:598–605. doi: 10.1038/ejcn.2010.284. [DOI] [PubMed] [Google Scholar]
- 24.Patil VC, Parale GP, Kulkarni PM, Patil HV. Relation of anthropometric variables to coronary artery disease risk factors. Indian J Endocrinol Metab. 2011;15:31–7. doi: 10.4103/2230-8210.77582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Neri D, Espinoza A, Bravo A, Rebollo MJ, Moraga F, Mericq V, et al. Visceral adiposity and its association with serum lipids in female obese teenagers. Rev Med Chil. 2007;135:294–300. doi: 10.4067/s0034-98872007000300003. [DOI] [PubMed] [Google Scholar]