

Abstract
Hypertension is an important worldwide public -health challenge with high mortality and disability. Due to the limitations and concerns with current available hypertension treatments, many hypertensive patients, especially in Asia, have turned to Chinese medicine (CM). Although hypertension is not a CM term, physicians who practice CM in China attempt to treat the disease using CM principles. A variety of approaches for treating hypertension have been taken in CM. For seeking the best evidence of CM in making decisions for hypertensive patients, a number of clinical studies have been conducted in China, which has paved the evidence-based way. After literature searching and analyzing, it appeared that CM was effective for hypertension in clinical use, such as Chinese herbal medicine, acupuncture, moxibustion, cupping, qigong, and Tai Chi. However, due to the poor quality of primary studies, clinical evidence is still weak. The potential benefits and safety of CM for hypertension still need to be confirmed in the future with well-designed RCTs of more persuasive primary endpoints and high-quality SRs. Evidence-based Chinese medicine for hypertension still has a long way to go.
1. Introduction
In global health politics, cardiovascular disease is the elephant in the room; it is a massive problem that few want to acknowledge and even fewer want to tackle [1]. Cardiovascular disease (CVD) is as the leading cause of death worldwide, accounting for an estimated 30% and 10% of all deaths and disability, respectively [2, 3]. It is reported that, approximately 62% of strokes and 49% of myocardial infarctions are caused by high blood pressure (BP) [4]. Hypertension is an important worldwide public-health challenge because of its high frequency and concomitant risks of cardiovascular and kidney disease [5]. It affects about 972 million adults worldwide [5] and is attributable each year for 7.6 million excess deaths and loss of 92 million disability-adjusted life years (DALYs) [2]. The purpose of antihypertensive treatment is to prevent the occurrence of CVD, by means of strict control of BP [6]. However, hypertension in most adults remains untreated or uncontrolled. BP control in the population is far from optimal, and SBP/DBP values <140/90 mmHg are achieved in no more than 25% of patients with treated hypertension worldwide [1]. Effective treatment of hypertension is limited by availability, cost, and adverse effects of antihypertensive medications [6]. Thus, due to the limitations and concerns with current available hypertension treatments, a certain proportion of the population, especially in Asia, has turned to complementary and alternative medicine (CAM) [7–11], including Chinese medicine (CM) [12–15], in searching for a treatment modality with potential efficacy and few advice effects. CAM is becoming increasingly popular and frequently used among patients with CVD, but these therapies lack demonstrated efficacy and safety for treating cardiovascular disease including hypertension [16]. Further research is essential in all areas of CAM to confirm its usefulness as an adjunct therapy [17, 18].
Chinese medicine, a system of ancient medical practice that differs in substance, methodology, and philosophy to modern medicine, plays an important role in health maintenance for the peoples of Asia and is becoming more frequently used in countries in the West [19]. It has been used to treat symptoms related to hypertension for more than 2500 years [20, 21]. Today, CM is commonly used to treat hypertension in China and the West [22–25]. And until now, the efficacy of CM for treating hypertension is suggested by a large number of published case series and uncontrolled trials [26–30]. Six randomized controlled trials [31–36] reported significant reductions in BP relative to randomly assigned control groups treated for 4 to 12 weeks, whereas the other six trials [37–42] reported negative results of CM relative to control subjects. For seeking the best evidence of CM in making decisions for hypertensive patients, a number of clinical studies have been conducted in China to gain credibility with the researchers' unremitting efforts. Thus, it is helpful to review the current research status of clinical study of evidence-based Chinese medicine for hypertension.
The purpose of the paper is to review multiple approaches of Chinese medicine therapies for the treatment of hypertension. The literature available through both English and Chinese search engines that discusses the potential uses of Chinese medicine therapies to treat hypertension is reviewed. The English language literature is searched through the Cochrane Central Register of Controlled Trials (CENTRAL) in the Cochrane Library (September, 2012), MEDLINE (1959–2012), PUBMED (1959–2012), and EMBASE (1980–2012) databases. The Chinese language literature was searched through Chinese National Knowledge Infrastructure (CNKI) (1980–2012), Chinese Scientific Journal Database (VIP) (1989–2012), Chinese Biomedical Literature Database (CBM) (1978–2012), and WANFANG (1998–2012) databases. The following search terms were used individually or combined: “traditional Chinese medicine,” “Chinese medicine,” “Chinese herbal medicine,” “herb,” “blood pressure,” “hypertension,” “essential hypertension.” Chinese terms that were used in search were equivalent to those used to search from English language databases. Finally, 15 systematic reviews (SRs) and meta-analysis [43–57] were collected and reviewed for this study, with 5 articles in English [47, 53–56] and 10 articles in Chinese [43–46, 48–52, 57]. To our knowledge, this is the first systematic English review of the evidence-based Chinese herbs for the treatment of hypertension.
2. The Understanding of Hypertension from the Perspective of Chinese Medicine
Different from Western medicine (WM), Chinese medicine (CM) has formed a unique way to diagnose and treat diseases [58]. Great efforts have been made by China's ancient ancestors through meticulous observation of nature, the cosmos, and the human body. And a series of traditional medical practices were originated in China including Chinese herbal medicine (CHM), acupuncture, moxibustion, cupping, qigong, Tai Chi (shadow boxing exercise), diet, and exercise therapy.
As we know, blood pressure is the diagnostic gold standard in conventional medicine. Thus, there is no concept and diagnosis of hypertension in ancient China. Although hypertension is not a CM term, physicians who practice CM in China attempt to treat the disease using CM principles. According to the typical signs and symptoms of the disease, it falls into the category of “vertigo or headache” in CM [21]. CM has long been used to treat hypertension-related symptoms in clinical practice for centuries. CM approaches hypertension as it does for other diseases under the guidance of holistic concept and treatment based on syndrome differentiation and formula syndrome differentiation [59, 60]. CM has been widely used to certain syndromes and formula syndromes in hypertension, such as fire syndrome, Banxia Baizhu Tianma Tang (decoction of Pinellia ternata, Atractylodes, and Gastrodia elata) syndrome [61]. Physicians who prescribe Chinese herbs and formulas recently realized that patient with hypertension exhibit the same pathological changes as those that are characteristic of fire syndrome and Banxia Baizhu Tianma Tang (Decoction of Pinellia ternata, Atractylodes and Gastrodia elata) syndrome. Moreover, increasing evidence indicates that, Chinese herbs and formulas that improve fire syndrome and Banxia Baizhu Tianma Tang (Decoction of Pinellia ternata, Atractylodes, and Gastrodia elata) syndrome are useful in treating hypertensive patients in China [21].
In our previous studies, hypertension could be divided into the following three major types on the basis of the stage and symptoms of the disease in CM. The first one is fire syndrome which could be found in various stages of hypertension. It can also be further divided into four types such as liver fire, heart fire, stomach fire, and intestinal fire. The second one is phlegm-fluid retention syndrome which often appears in the later stage of the disease. In light of the disease location, it could be divided into three types such as fluid retention in up jiao syndrome, fluid retention in middle jiao syndrome, and fluid retention in down jiao syndrome. The last one is deficiency syndrome. The most common deficiency syndromes are spleen deficiency syndrome and kidney deficiency syndrome. The recommended treatment program of hypertension by Chinese herbal formulas is shown in Table 1.
Table 1.
Recommended treatment program of hypertension by Chinese herbal formulas.
| Syndrome | Clinical signs | Treatment principles | Classical formula |
|---|---|---|---|
| Fire syndrome | |||
| Liver fire syndrome | Vertigo, headache, facial flushing with perspiration, conjunctival congestion, bitter taste in the mouth, thirst, irritability and restlessness, wiry-rapid-powerful pulse or powerful cunkou pulse alone, or wiry and long pulse even well beyond the cunkou pulse | Calming liver and suppressing liveryang hyperactivity | Tianma Gouteng decoction, Zhengan Xifeng decoction, Jianling decoction, and Longdan Xiegan decoction |
| Heart fire syndrome | Facial flushing with perspiration, bitter taste in the mouth, thirst, insomnia, red tip of the tongue, and rapid pulse | Clearing heart fire | Zhi-zi-chi decoction, Sanhuang Xiexin decoction, and Huanglian Jiedu decoction |
| Stomach fire syndrome and intestine fire syndrome | Dry mouth, thirst with desire for cold drinks, easy to starve, foul breath, abdominal distension and pain, smelly stool, constipation, red tongue, yellow dry fur, right guan pulse powerful alone, or strength and deep-hidden-powerful pulse | Clearing stomach-intestine fire, promoting digestion, relaxing bowels, and relieving constipation | Da Chai Hu decoction, Baohe pill, Baihu decoction, Houpu Dahuang decoction, Gegen Qinlian decoction, and Zeng Ye decoction |
|
| |||
| Phlegm-fluid retention syndrome | |||
| Phlegm and dampness syndrome | Obesity, dizziness, sticky mouth, thirst without a desire to drink, chest distress, nausea, vomiting, anorexia, abdominal distension, loose stools, sleepiness, greasy tongue coating, and slippery pulse | Dispelling phlegm and eliminating dampness | Erchen decoction, Pingwei powder, Wendan decoction, Banxia Baizhu Tianma decoction, and Xiao Xianxiong decoction |
| Fluid retention syndrome | Dizziness aggravated by change in body position, thirst without a desire to drink or not being thirsty, chest distress, palpitation, gastric distension, abdominal distension, poor appetite, lumbar heaviness, weakness and heaviness in the lower extremities, edema, daytime sleepiness, abnormal leucorrhea, dysuria, greasy fur, swollen tongue, and deep pulse | Dissipating excessive fluid | Banxia baizhu tianma decoction, Wuling powder, Zhuling decoction, Zexie decoction, and Fuling Guizhi Baizhu Gancao decoction |
|
| |||
| Deficiency syndrome | |||
| Spleen deficiency syndrome | Fatigue, shortness of breath, stomach pain, poor appetite, abdominal distension, and loose stools | Reinforcing spleen | Fuling Guizhi Baizhu Gancao decoction, Si jun Zi decoction, and Liu Jun Zi decoction |
| Kidney deficiency syndrome | Tiredness in the loins and legs, tinnitus and dizziness, sexual dysfunction, dysuria, weakness and fatigue, and weak chi pulse | Reinforcing kidney | Liuwei Dihuang pill and Shenqi pill |
Each CHM under the classical formula is composed of multiple herbs.
A variety of approaches for treating hypertension have been taken in CM. Among them, Chinese herbal therapy is the most commonly used. Furthermore, acupuncture, moxibustion, cupping, qigong, Tai Chi (Shadow boxing exercise), and CM external therapy (including bath foot, acupoint application, and thorn collaterals bloodletting) could also be used in the treatment of the disease.
3. Paving the Way for Evidence-Based Chinese Medicine for Hypertension
Evidence-based medicine (EBM), a new paradigm for medical practice, quickly developed in the 1990s. According to the book of “Evidence-based Medicine: How to Practice and Teach EBM” written by Dr. Sackett, one of the pioneers in EBM, EBM makes the explicit, judicious, and conscientious use of the best evidence in making decisions for preventing diseases, promoting the recovery and improving life quality [62]. It has brought great impacts on the efficacy and safety of previous widely accepted strategies of therapeutic, rehabilitative, and preventive regimens by the evidences from a series of systematic reviews and meta-analysis. That is to say clinical experience is unreliable and all medical interventions should be based on rigorous research evidences [63]. Eugene Braunwald, a famous cardiologist, also advocated that current cardiology practice should be evidence based and global in scope [64].
There is close relationship between CM and EBM [65]. Due to the shortage of objective and quantitative criteria in evaluating therapeutic effect and safety in CM, it is urgent to formulate a scientific way. The emergence of EBM had just provided an appropriate method to solve this critical issue. As the applications of CM in the treatment of hypertension are increasing, more and more concern on the efficacy and safety are aroused [22]. Whether CM is equal or superior to WM, how CM plays the role in enhancing efficacy and reducing toxicity, and how to optimize the therapeutic regimen by combination of CM and WM, all these problems are not clear currently. All of these issues warrant further investigation and need more evidences. Here, the paper reviews the background of CM for the treatment of hypertension.
According to historical records in CM classics, the earliest evidence of Chinese herbal medicine used in China is of two graves from the Han Era (206 B.C. to 220 A.D.) [66]. There are a large number of clinical trials about classical famous prescriptions for the treatment of “vertigo or headache” since ancient time. Although patients with “vertigo or headache” may not necessarily be fully consistent with the diagnosis of hypertension, previous widely used formulae still have a good clinical effect in the treatment of hypertension today. Physicians in ancient China realized that there is a certain connection between a special pattern and a corresponding herb or formula in the clinical practice. And they recorded the treatment process. It is considered as the “clinical trial” in ancient time. After then, the “clinical trial” was tested and repeated by the successors for hundreds or even thousands of years. Thus, it is a unique clinical trial. In the trial, the special pattern is also known as “formula syndrome” or “herb syndrome” [60], which is the indication of Chinese herbs and formulas [59]. The corresponding formula is called classical formulae. These classical formulae in the treatment of hypertension included Tianma Gouteng Yin (decoction of Gastrodia and Uncaria), Banxia Baizhu Tianma Tang (decoction of Pinellia ternata, Atractylodes and Gastrodia elata), Longdan Xiegan Tang (decoction of radix gentianae for purging liver fire), Da Chai Hu Tang (Major Bupleurum Decoction), Zexie Tang (Decoction of American water Plantain), and Liu Wei Dihuang Wan (Pill of Rehmannia) [21].
In order to obtain supportive evidence of CM herbs and approaches that are thought to exert hypotensive effect, we retrieved the data primarily via the Internet (Cochrane Library, PubMed, EMBASE, CNKI, VIP, CBM, and WANFANG) up to September 30, 2012. All the case reports, case series, case control studies, ideas, editorials opinions, animal studies, in vitro studies, randomized controlled trials, systematic reviews, and meta-analysis based on CM for essential hypertension were included. There were no restrictions on population characteristics, language, and publication type. Duplicated publications reporting that the same groups of participants were excluded. We could see from Figure 1 that there are a large number of researches in the field of CM for hypertension in the past 50 years, especially in the past 30 years.
Figure 1.
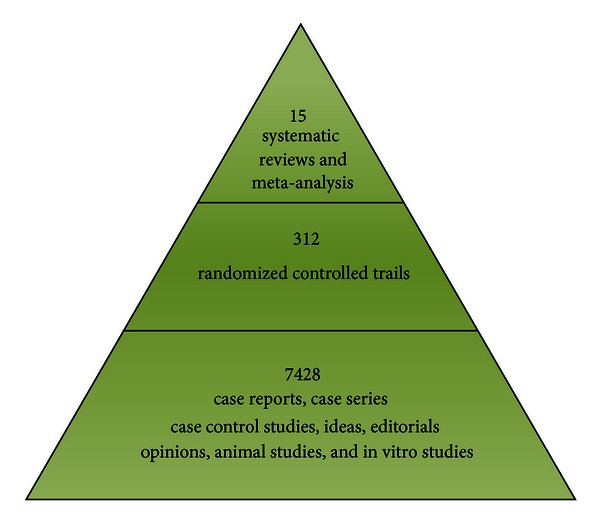
Number of studies on CM for hypertension published in Cochrane Library, PubMed, EMBASE, CNKI, VIP, CBM, and WANFANG.
As shown in the first stage, 7428 studies reported the effectiveness of CM for hypertension ranging from case control studies, case reports, case series, ideas, editorials, opinions, animal studies, and in vitro studies to controlled observational studies. Among the herbal therapies, it includes three categories of formulae. The first one is individually prescribed decoctions, which have been used in most outpatients and inpatients. The second one is currently effective practice formula or experienced prescriptions from famous CM doctors. The third one is the modified classical formulae. The last one is the classical formulae or well-known Chinese medicine formula. In recent decades, the proprietary Chinese medicines (PCMs) for treatment of hypertension are mainly originated from the last three categories. The PCMs have been tested in a large number of clinical trials.
With increasing awareness and practice of EBM, 312 randomized controlled trials (RCTs) have been conducted to evaluate the effectiveness of CM for hypertension as shown in the second stage.
Regarding clinical effect and its evaluation in clinical researches on CM for hypertension, systematic reviews (SRs) and meta-analysis are important approaches to get the best available evidence. In the third stage of Figure 1, there are 15 SRs and meta-analysis [43–57] collected after literature searches.
4. Exploring the Differences in Response to Treatment from SR
As shown in Table 2, there are 15 SRs and meta-analysis of CM for hypertension published in Chinese or English. Here, these published findings are analyzed to explore the range and role of CM for the treatment of hypertension.
Table 2.
The characteristics of systematic reviews and meta-analysis of CM for hypertension.
| Intervention | Title | Authors | Year published |
Trials | Participants included |
Authors' comments |
|---|---|---|---|---|---|---|
| Meta-analysis of effectiveness of antihypertension of 442 traditional Chinese herbal decoctions | Ding and Zhou [43] | 2012 | 7 | 808 | Limited evidence suggested that total effective rate and efficiency of CM are lower than those of single WM as for BP controlling. But owing to lack of data from high-quality RCT, the efficacy need to be further studied. | |
| Quantitative analysis of clinical controlled trials of traditional Chinese medicine and systematic evaluation of randomized controlled trials involving traditional Chinese medicine for essential hypertension | Hu [44] | 2009 | 24 | 1660 | CM combined with WM showed better results than WM for treating hypertension. However, due to the generally low quality of the trials, large sample, multicenter double blind RCTs with strict design are warranted. | |
| Meta-analysis of traditional Chinese medicine for essential hypertension | Ren et al. [45] | 2006 | 11 | 1010 | CM may be beneficial to reduce BP in patients with hypertension. | |
| Chinese Herbal medicine | Systematic review and meta-analysis of Tianma Gouteng Yin combined with enalapril for essential hypertension | Dong et al. [46] | 2011 | 6 | 543 | Tianma Gouteng Yin combined with enalapril showed additional better effects than enalapril for hypertension. No serious adverse event is reported. Due to the low methodological quality and potential bias of trials, large-sample, multicenter, randomized, double-blind, controlled trials are warranted. |
| Tianma Gouteng Yin Formula for treating primary hypertensionE | Zhang et al. [47] | 2012 | 0 | 0 | The review could not find any randomized controlled clinical trials that compared Tianma Gouteng Yin Formula (TGYF) to placebo or no treatment. The authors cannot draw a conclusion that TGYF may be beneficial for hypertension. Well-designed randomized controlled studies need to be conducted and published. | |
| Systematic review of clinical evidence about calm the liver and subdue yang therapy on the hypertension disease with the syndrome of upper hyperactivity of liver yang | Xu and Li [48] | 2012 | 8 | 944 | The calm the liver and subdue yang therapy for treating hypertension disease with syndrome of upper hyperactivity of liver yang has curative effect and high safety. However, owing to lack of data from high-quality RCT and potential publication bias, the positive findings should be interpreted conservatively. | |
| Systematic review of replenishing kidney qi method for essential hypertension with kidney qi deficiency syndrome | Shi and Zhang [49] | 2012 | 5 | 457 | The replenishing kidney qi therapy for treating hypertension with kidney qi deficiency syndrome has curative effect and high safety. High-quality and large-scale RCTs are needed to further prove the results of the study because of the low quality of the included studies. | |
| Systematic review on treatment of essential hypertension from spleen and kidney deficiency | Liu and Li [50] | 2011 | 15 | 1661 | Treatment of essential hypertension from the spleen and kidney deficiency was effective, and the level of safety is reliable. However, the quality of most trials was low. | |
| Effects of Chinese medicine on elderly isolated systolic hypertension: a meta-analysis | Li and Yang [51] | 2012 | 17 | 1323 | Chinese medicine is effective on treating isolated systolic hypertension of the old, as well as reducing symptoms and pulse pressure. | |
|
| ||||||
| Acupuncture | The effect of acupuncture therapy on essential hypertension: a systematic review of long-term effect | Zhao et al. [52] | 2011 | 18 | 1460 | Although it shows a tendency that acupuncture can improve the conditions of essential hypertension, a reliable conclusion cannot be drawn from the present data because of the defects in methodological quality and insufficient numbers of trials. It is necessary to perform more multicentral RCTs of high quality in the future. |
|
| ||||||
| Moxibustion | Moxibustion for hypertension: a systematic reviewE | Kim et al. [53] | 2010 | 4 | 240 | There is insufficient evidence to suggest that moxibustion is an effective treatment for hypertension. Rigorously designed trials are warranted to answer the many remaining questions. |
|
| ||||||
| Cupping | Cupping for hypertension: a systematic reviewE | Lee et al. [54] | 2010 | 2 | 76 | The evidence is not significantly convincing to suggest that cupping is effective for treating hypertension. Further research is required to investigate whether it generates any specific effects for that condition. |
|
| ||||||
| Qigong | Qigong for hypertension: a systematic review of randomized clinical trialsE | Lee et al. [55] | 2007 | 12 | 1332 | There is some encouraging evidence of qigong for lowering SBP, but the conclusiveness of these findings is limited. Rigorously designed trials are warranted to confirm these results. |
| Clinical effect of Qigong practice on essential hypertension: a meta-analysis of randomized controlled trialsE | Guo et al. [56] | 2008 | 9 | 908 | Self-practiced qigong for less than 1 year is better in decreasing BP in patients with essential hypertension than in no-treatment controls, but is not superior to that in active controls. More methodologically strict studies are needed to prove real clinical benefits of qigong and to explore its potential mechanism. | |
|
| ||||||
| Tai Chi | Systematic review of Tai Chi for essential hypertension | Li and Xu [57] | 2011 | 5 | 318 | Tai Chi is effective on treating essential hypertension. However, different exercise time of Tai Chi has an impact on hypertensive patients. More RCTs of high quality are warranted to prove benefits of Tai Chi on hypertensive patients with different stages. |
CM: Chinese medicine; WM: Western medicine; RCT: randomized controlled trial; BP: blood pressure; SBP: systolic blood pressure; and E: in English.
4.1. Chinese Herbal Medicine
There are 9 SR of Chinese herbal medicines published whether on individually prescribed decoctions or classical formulae for hypertension. The results are shown in Table 1 [43–51]. Comprehensive evaluations of the clinical efficacy of the Chinese herbal medicine were conducted in 3 SRs [43–45]. Chinese herbal medicine, which could clear fire, suppress liver yang hyperactivity, remove blood stasis, fluid and phlegm, nourish kidney, and reinforce spleen qi, were all included in the analysis. The result showed that Chinese herbal medicine the use of alone may be beneficial to reduce BP in patients with hypertension, and no significant difference was found between CM and WM [44, 45]. Combination therapies, just CM combined with WM, showed better results than those of WM for treating hypertension [45]. However, another SR reported negative results that total effective rate and efficiency of CM are lower than that of single WM as for BP controlling [43]. Owing to the lack of data from high-quality RCT, the efficacy needs to be further studied [43–45].
Tianma Gouteng Yin Formula (TGYF), a famous prescription noted in Za Bing Zheng Zhi Xin Yi (New Meanings in Syndrome and Therapy of Miscellaneous Diseases), contains eleven commonly used herbs (Gastrodia Elata, Uncaria, Abalone Shell, Eucommia Ulmoides Oliv, Achyranthes Root, Loranthus Parasiticus, Gardenia, Scutellaria Baicalensis Georgi, Leonurus Japonicus, Poria Cocos, and caulis polygoni multiflori). It could suppress liver yang hyperactivity, clear heat, activate blood, and nourish the kidney; it has been widely used to treat hypertension-related signs and symptoms in clinical practice for centuries in China. 2 SRs [46, 47] assess the efficacy and safety of TGYF for treating primary hypertension. One SR [46] showed that TGYF combined with enalapril showed additional better effects than enalapril for hypertension. No serious adverse event is reported. However, the other SR could not find any randomized controlled clinical trials that compared TGYF to placebo or no treatment [47]. Authors advised that well-designed randomized controlled studies need to be conducted and published.
Liver yang hyperactivity syndrome, kidney deficiency syndrome, and spleen deficiency syndrome are very common in CM. Aiming to improve these different syndromes, treatment principles of calming the liver and replenishing kidney and spleen were used, respectively. 3 SRs [48–50] assess the efficacy and safety of treatment based on Chinese medicine principles for hypertension. All SR showed curative effect and high safety of CM.
When referring to elderly isolated systolic hypertension, it indicated that CM is effective on treating isolated systolic hypertension of the old, as well as reducing symptoms and pulse pressure [51]. Authors also gave conclusions that the evidence for the favorable results in the trials is limited, and these findings should be carefully interpreted due to the low methodological quality.
4.2. Acupuncture
Acupuncture is considered an ancient practice of TCM that began thousands of years ago. It has been reported to have potential effectiveness for treating cardiovascular diseases including hypertension, with few reported adverse effects [67, 68]. Several features of acupuncture make it an attractive therapeutic alternative with increasing popularity [36]. Although the results of the trials showed a tendency that acupuncture can improve the conditions of essential hypertension, a reliable conclusion cannot be drawn from the present data because of the defects in methodological quality and insufficient numbers of trials [52]. Thus, evidence of efficacy in lowering blood pressure from controlled trials has been scant. It is necessary to perform more multicentral RCTs of high quality in the future.
4.3. Moxibustion
Moxibustion, a traditional medical intervention of CM, involves the application of ignited mugwort (Artemisia vulgaris) directly or indirectly at acupuncture points or other specific parts of the body to treat or prevent diseases [69]. The mechanism of moxibustion maybe related to the combination of heat (burning pain and heat stress), tar (extract), aroma (fume), and psychological stress [70]. According to the theory of CM, a possible explanation for how moxibustion works is that heat could increases qi circulation and relieves qi stagnation by stimulating the acupuncture points to regulate the function of meridians and visceral organs [71]. A SR on the effects of moxibustion on hypertension revealed no evidence that moxibustion is beneficial to people with hypertension [53]. Differences between specific and nonspecific effects should be examined in a future study, and rigorously designed trials are warranted to answer the many remaining questions.
4.4. Cupping
Cupping therapy, as a part of CM, is widely used in treating pain and many other complaints for millennia [72]. A glass cup is utilized to create suction over a painful area or an acupuncture point after incisions are made to the skin. By doing so, the skin is pulled into the cup without drawing blood. Therefore, negative pressure acts on the skin and irritates subcutaneous muscles. It is often used to lower BP and relieve hypertension-related symptoms such as headaches and anxiety [73]. A SR on the effect of cupping on hypertension revealed no significantly convincing evidence to suggest that cupping is effective for treating hypertension. Further research is required to investigate whether it generates any specific effects for that condition [54].
4.5. Qigong
Qigong, as an ancient Chinese healing art, is widely used in Asia and has been officially recognized as a standard medical technique in Chinese hospitals. It involves exercises for posture, coordination of different breathing patterns, movement, and meditation [74]. According to the theory of CM, it could increase the healthy flow of qi throughout the body to heal itself. It is claimed that qigong has potential beneficial effects on various disorders, including cardiovascular disease [75]. Several RCTs have claimed that qigong has therapeutic effects on blood pressure in patients with hypertension [76–78]. 2 SRs on the effects of qigong on hypertension revealed some encouraging evidence of qigong for lowering BP. However, the conclusiveness of these findings is limited. Rigorously designed trials are warranted to confirm these results [55, 56].
4.6. Tai Chi
Tai Chi (also known as Tai Chi Quan or Shadow Boxing), originated in ancient China, is a Chinese conditioning exercise well known for its graceful movement. It has been practiced for centuries in the East for health promotion and longevity. In recent years, there has been a growing interest and prevalence in Tai Chi exercise in western societies. During the practice, it combines deep diaphragmatic breathing with continuous body motions to achieve a harmonious balance between body and mind. Previous researches have indicated that Tai Chi exercise may improve health-related fitness (including cardiorespiratory function, muscular strength, balance, and flexibility), quality of life, and psychological well-being. Recent studies also suggest that it may have beneficial effects for patients with cardiovascular conditions and some cardiovascular risk factors [79, 80], including hypertension [81]. There are few trials on the effectiveness of Tai Chi in the management of hypertension. A SR [57] including 5 randomized clinical trials with 318 hypertensive patients reported some positive findings for Tai Chi on treating essential hypertension. It is also pointed out that different exercise time of Tai Chi has an impact on hypertension. However, more RCTs of high quality are warranted to prove benefits of Tai Chi on hypertensive patients with different stages.
5. Providing Evidence of Safety
It is widely accepted that herbal medicine is undoubtedly safe for various diseases in China. However, with the increasing reports of liver toxicity and other adverse events associated with Chinese herbal medicines [82–84], the safety of CM needs to be monitored rigorously and reported appropriately in the future clinical trials [85–87]. According to our review, safety evaluation of CM is not the highlight. Inadequate reporting on adverse events is found either in the included SRs or in the original RCTs. Most of the adverse effects of CM were mentioned as “low adverse effect” or “none obvious.” Only six of the fifteen SRs reported the adverse effect of CM briefly, providing limited information [43, 46, 48–50, 56]. Among them, four SRs about Chinese herbal medicine [43, 46, 48, 50] reported nine specific symptoms in treatment group including headache, dizziness, dry mouth, dry cough, abdominal distension, and constipation. However, all these adverse events could be tolerated by participants in the trials. The other two SRs reported no serious adverse event in replenishing kidney qi group [49] and qigong group [56]. The rest nine SRs did not mention whether they had monitored adverse effects at all [44, 45, 47, 51–55, 57]. It is generally believed that acupuncture, moxibustion, cupping, qigong, and Tai Chi have reliable safety. Unfortunately, included SRs about these approaches provided insufficient evidence. Therefore, conclusions about the safety of CM cannot be made from this paper and needs to be further proven, due to the limited, inadequate recording, and reporting of adverse events.
6. Discussion
Considerable progress has been made by domestic and foreign clinical experts and researchers for the treatment of hypertension [88–90]. Oral antihypertensive drugs are a milestone in the therapy of essential hypertension. However, the current awareness, control, and mortality rates of hypertension are still far from optimal [91, 92]. Only 25% of patients could achieve the goal, and recurrent cardiovascular events still occur in those who take antihypertensive drugs. What's more, numerous adverse reactions, including headache, dizziness, orthostatic hypotension, and decreased sexual function, limit the clinical practice of antihypertensive drugs [93]. Thus, traditional medicine (TM) has got increasing popularity with people all over the world [94–97]. CM has made great contributions to the health and well-being of the people for its unique advantages in preventing and curing diseases, rehabilitation, and health care [98–103]. Over the past 30 years, the study of CM for treating hypertension is the most active area of researches worldwide [104–108]. Significant progress has been made from theory and experiments to clinic fields based on the inheritance and innovation of thoughts of CM for hypertension [109–113]. A recent study investigated the multiprotective mechanisms of Chinese herbal formulas for treating hypertension from the perspective of modern science, including smoothly controlling BP, reducing blood pressure variability (BPV), protecting target organs, regulating renin-angiotensin-aldosterone system (RAAS), reversing risk factors, improving endothelial function, blocking calcium channels, improving life quality and clinical symptoms, and reversing uncontrollable factors of BP [114]. Therefore, much attention has been paid to the holistic, multitarget, and multidimensional pharmacological studies of CM currently.
The systematic reviews indicated the potential benefit of CM for hypertension in terms of some outcome measures, but none of them drew a definite conclusion due to the poor quality of primary studies. Poor methodology and reporting quality of SRs about CM have caused widespread concern [115, 116]. According to preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement, it was found that most of the included reviews have poor quality [117]. If the reviews are poorly designed and reported, misleading conclusions about current clinical practice would be given. So, the reporting of SR should be in accordance with PRISMA in future researches. The included literature must be scrutinized and selected strictly in order to avoid the potential bias. Process of extracting data such as study design, allocation sequence, allocation concealment, blinding, intention to treat analysis, and drop outs should be conducted rigorously. Also, how to evaluate the validity of the primary studies is an important aspect. It is well known that the primary goal of the treatment for essential hypertension is to reduce mortality and prevent progression to heart disease and other complications of hypertension. The secondary endpoints are mainly blood pressure, blood liquid, and traditional Chinese medicine syndromes [118]. Our overview showed that there is a lack of definite data on the primary endpoints, whereas the secondary endpoints were most commonly adopted in clinical trials. Therefore, the persuasion of conclusions about CM for hypertension would be reduced greatly. Although it appeared that CM was effective for hypertension in clinical use, such as Chinese herbal medicine, acupuncture, moxibustion, cupping, qigong, and Tai Chi, most SRs were inconclusive that CM had a definite effect owing to the poor evidence. As weak recommendations result from low quality evidence, high quality evidence of CM for hypertension is warranted in further RCTs to guide clinical practice either for hypertensive patients or physicians.
In conclusion, evidence-based Chinese medicine for hypertension still has a long way to go [119, 120]. The potential benefits and safety of CM for hypertension still need to be confirmed in the future with well-designed RCTs of more persuasive primary endpoints and high-quality SRs. Although the development of evidence-based CM for hypertension will be full of challenge, we have full confidence.
Conflict of Interests
All authors declare that they have no conflict of interests.
Acknowledgments
This work was supported in part by the National Basic Research Program of China (973 Program, 2003CB517103) and the National Natural Science Foundation Project of China (90209011).
References
- 1.MacMahon S, Alderman MH, Lindholm LH, Liu LS, Sanchez RA, Seedat YK. Blood-pressure-related disease is a global health priority. The Lancet. 2008;371(9623):1480–1482. doi: 10.1016/S0140-6736(08)60632-7. [DOI] [PubMed] [Google Scholar]
- 2.Lawes CM, Vander Hoorn S, Rodgers A. Global burden of blood-pressure-related disease, 2001. The Lancet. 2008;371(9623):1513–1518. doi: 10.1016/S0140-6736(08)60655-8. [DOI] [PubMed] [Google Scholar]
- 3.World Health Organization. World Health Statistics 2006. Geneva, Switzerland: World Health Organization; 2006. [Google Scholar]
- 4.Farsang C, Naditch-Brule L, Avogaro A, et al. Where are we with the management of hypertension? From science to clinical practice. The Journal of Clinical Hypertension. 2009;11(2):66–73. doi: 10.1111/j.1751-7176.2008.00066.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J. Global burden of hypertension: analysis of worldwide data. The Lancet. 2005;365(9455):217–223. doi: 10.1016/S0140-6736(05)17741-1. [DOI] [PubMed] [Google Scholar]
- 6.Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension. 2003;42(6):1206–1252. doi: 10.1161/01.HYP.0000107251.49515.c2. [DOI] [PubMed] [Google Scholar]
- 7.Xu H, Chen KJ. Complementary and alternative medicine: is it possible to be mainstream? Chinese Journal of Integrative Medicine. 2012;18(6):403–404. doi: 10.1007/s11655-012-1126-7. [DOI] [PubMed] [Google Scholar]
- 8.Chen KJ, Hui KK, Lee MS, Xu H. The potential benefit of complementary/alternative medicine in cardiovascular diseases. Evidence-Based Complementary and Alternative Medicine. 2012;2012:1 pages. doi: 10.1155/2012/125029.125029 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Wood MJ, Stewart RL, Merry H, Johnstone DE, Cox JL. Use of complementary and alternative medical therapies in patients with cardiovascular disease. American Heart Journal. 2003;145(5):806–812. doi: 10.1016/S0002-8703(03)00084-X. [DOI] [PubMed] [Google Scholar]
- 10.Wang J, Xiong XJ, Feng B, Xu H. Cardiovascular effects of salvianolic acid B. Evidence-Based Complementary and Alternative Medicine. 2013;2013 doi: 10.1155/2013/247948.247948 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Yeh GY, Davis RB, Phillips RS. Use of complementary therapies in patients with cardiovascular disease. American Journal of Cardiology. 2006;98(5):673–680. doi: 10.1016/j.amjcard.2006.03.051. [DOI] [PubMed] [Google Scholar]
- 12.Chen KJ. Clinical service of Chinese medicine. Chinese Journal of Integrative Medicine. 2008;14(3):163–164. doi: 10.1007/s11655-008-0163-8. [DOI] [PubMed] [Google Scholar]
- 13.Xu H, Chen KJ. Integrative medicine: the experience from China. The Journal of Alternative and Complementary Medicine. 2008;14(1):3–7. doi: 10.1089/acm.2006.6329. [DOI] [PubMed] [Google Scholar]
- 14.Chen KJ, Xu H. The integration of traditional Chinese medicine and Western medicine. European Review. 2003;11(2):225–235. [Google Scholar]
- 15.Wang J, Xiong XJ. Current situation and perspectives of clinical study in integrative medicine in China. Evidence-Based Complementary and Alternative Medicine. 2012;2012:11 pages. doi: 10.1155/2012/268542.268542 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Astin JA. Why patients use alternative medicine: results of a national study. Journal of the American Medical Association. 1998;279(19):1548–1553. doi: 10.1001/jama.279.19.1548. [DOI] [PubMed] [Google Scholar]
- 17.Arthur HM, Patterson C, Stone JA. The role of complementary and alternative therapies in cardiac rehabilitation: a systematic evaluation. European Journal of Cardiovascular Prevention and Rehabilitation. 2006;13(1):3–9. doi: 10.1097/00149831-200602000-00002. [DOI] [PubMed] [Google Scholar]
- 18.Lin MC, Nahin R, Gershwin ME, Longhurst JC, Wu KK. State of complementary and alternative medicine in cardiovascular, lung, and blood research: executive summary of a workshop. Circulation. 2001;103(16):2038–2041. doi: 10.1161/01.cir.103.16.2038. [DOI] [PubMed] [Google Scholar]
- 19.Cheung F. TCM: made in China. Nature. 2011;480(7378):S82–S83. doi: 10.1038/480S82a. [DOI] [PubMed] [Google Scholar]
- 20.Chen KJ, Li LZ. Study of traditional Chinese medicine—which is after all the right way? Chinese Journal of Integrative Medicine. 2005;11(4):241–242. doi: 10.1007/BF02835782. [DOI] [PubMed] [Google Scholar]
- 21.Wang J, Xiong XJ. Control strategy on hypertension in Chinese medicine. Evidence-Based Complementary and Alternative Medicine. 2012;2012:6 pages. doi: 10.1155/2012/284847.284847 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ernst E. Complementary/alternative medicine for hypertension: a mini-review. Wiener Medizinische Wochenschrift. 2005;123:386–391. doi: 10.1007/s10354-005-0205-1. [DOI] [PubMed] [Google Scholar]
- 23.Nahas R. Complementary and alternative medicine approaches to blood pressure reduction: an evidence-based review. Canadian Family Physician. 2008;54(11):1529–1533. [PMC free article] [PubMed] [Google Scholar]
- 24.Bell RA, Suerken CK, Grzywacz JG, Lang W, Quandt SA, Arcury TA. CAM use among older adults age 65 or older with hypertension in the United States: general use and disease treatment. The Journal of Alternative and Complementary Medicine. 2006;12(9):903–909. doi: 10.1089/acm.2006.12.903. [DOI] [PubMed] [Google Scholar]
- 25.Kaplan NM. Acupuncture for hypertension: can 2500 years come to an end? Hypertension. 2006;48(5):p. 815. doi: 10.1161/01.HYP.0000241069.80574.76. [DOI] [PubMed] [Google Scholar]
- 26.Gong YM, Guo RX, Zhang LS. Application of jiang ya paste onto yongquan acupoint for treatment of primary hypertension. Journal of Traditional Chinese Medicine. 1995;15(2):112–113. [PubMed] [Google Scholar]
- 27.Wei GK, He JM, Chen ZG. Treatment of 104 cases suffering from cervico-spinal hypertension with rotation-reduction method—observation of the long-term effect. Journal of Traditional Chinese Medicine. 1989;9(4):266–268. [PubMed] [Google Scholar]
- 28.Huang HQ, Liang SZ. Acupuncture at otoacupoint heart for treatment of vascular hypertension. Journal of Traditional Chinese Medicine. 1992;12(2):133–136. [PubMed] [Google Scholar]
- 29.Chiu YJ, Chi A, Reid IA. Cardiovascular and endocrine effects of acupuncture in hypertensive patients. Clinical and Experimental Hypertension. 1997;19(7):1047–1063. doi: 10.3109/10641969709083204. [DOI] [PubMed] [Google Scholar]
- 30.Dong J. Acupuncture treatment of hypertension: a report of 70 cases. International Journal of Clinical Acupuncture. 1996;7:173–175. [Google Scholar]
- 31.Li H, Liu LT, Zhao WM, et al. Effect of traditional and integrative regimens on quality of life and early renal impairment in elderly patients with isolated systolic hypertension. Chinese Journal of Integrative Medicine. 2010;16(3):216–221. doi: 10.1007/s11655-010-0216-y. [DOI] [PubMed] [Google Scholar]
- 32.Zhong GW, Chen MJ, Luo YH, et al. Effect of Chinese herbal medicine for calming Gan and suppressing hyperactive yang on arterial elasticity function and circadian rhythm of blood pressure in patients with essential hypertension. Chinese Journal of Integrative Medicine. 2011;17(6):414–420. doi: 10.1007/s11655-011-0761-6. [DOI] [PubMed] [Google Scholar]
- 33.Park J, Hong S, Park T, et al. P02. 136. A randomized controlled trial for the use of qigong in the treatment of pre and mild essential hypertension. BMC Complementary and Alternative Medicine. 2012;12(supplement 1):p. P192. [Google Scholar]
- 34.Lee MS, Lim HJ, Lee MS. Impact of qigong exercise on self-efficacy and other cognitive perceptual variables in patients with essential hypertension. The Journal of Alternative and Complementary Medicine. 2004;10(4):675–680. doi: 10.1089/acm.2004.10.675. [DOI] [PubMed] [Google Scholar]
- 35.Walker AF, Marakis G, Morris AP, Robinson PA. Promising hypotensive effect of hawthorn extract: a randomized double-blind pilot study of mild, essential hypertension. Phytotherapy Research. 2002;16(1):48–54. doi: 10.1002/ptr.947. [DOI] [PubMed] [Google Scholar]
- 36.Flachskampf FA, Gallasch J, Gefeller O, et al. Randomized trial of acupuncture to lower blood pressure. Circulation. 2007;115(24):3121–3129. doi: 10.1161/CIRCULATIONAHA.106.661140. [DOI] [PubMed] [Google Scholar]
- 37.Stavro PM, Woo M, Heim TF, Leiter LA, Vuksan V. North American Ginseng exerts a neutral effect on blood pressure in individuals with hypertension. Hypertension. 2005;46(2):406–411. doi: 10.1161/01.HYP.0000173424.77483.1e. [DOI] [PubMed] [Google Scholar]
- 38.Stavro PM, Woo M, Leiter LA, Heim TF, Sievenpiper JL, Vuksan V. Long-term intake of North American Ginseng has no effect on 24-hour blood pressure and renal function. Hypertension. 2006;47(4):791–796. doi: 10.1161/01.HYP.0000205150.43169.2c. [DOI] [PubMed] [Google Scholar]
- 39.Macklin EA, Wayne PM, Kalish LA, et al. Stop hypertension with the acupuncture research program (SHARP): results of a randomized, controlled clinical trial. Hypertension. 2006;48(5):838–845. doi: 10.1161/01.HYP.0000241090.28070.4c. [DOI] [PubMed] [Google Scholar]
- 40.Li JJ, Lu ZL, Kou WR, et al. Beneficial impact of Xuezhikang on cardiovascular events and mortality in elderly hypertensive patients with previous myocardial infarction from the China Coronary Secondary Prevention Study (CCSPS) Journal of Clinical Pharmacology. 2009;49(8):947–956. doi: 10.1177/0091270009337509. [DOI] [PubMed] [Google Scholar]
- 41.Li JJ, Lu ZL, Kou WR, et al. Long-term effects of Xuezhikang on blood pressure in hypertensive patients with previous myocardial infarction: data from the Chinese Coronary Secondary Prevention Study (CCSPS) Clinical and Experimental Hypertension. 2010;32(8):491–498. doi: 10.3109/10641961003686427. [DOI] [PubMed] [Google Scholar]
- 42.Li JJ, Lu ZL, Kou WR, et al. Impact of Xuezhikang on coronary events in hypertensive patients with previous myocardial infarction from the China Coronary Secondary Prevention Study (CCSPS) Annals of Medicine. 2010;42(3):231–240. doi: 10.3109/07853891003652534. [DOI] [PubMed] [Google Scholar]
- 43.Ding HS, Zhou XF. Meta-analysis of effectiveness of anti-hypertension of 442 traditional Chinese herbal decoctions. Shi Yong Yi Yuan Lin Chuang Za Zhi. 2012;9(4):192–194. [Google Scholar]
- 44.Hu YX. Quantitative analysis of clinical controlled trials of traditional Chinese medicine and systematic evaluation of randomized controlled trials involving traditional Chinese medicine for essential hypertension [M.S. thesis] Guangzhou, China: Guangzhou University of Chinese Medicine; 2009. [Google Scholar]
- 45.Ren Y, Ou AH, Lin XZ, Lao YR. Meta-analysis of traditional Chinese medicine for essential hypertension. Shanxi Zhong Yi. 2006;27(7):794–796. [Google Scholar]
- 46.Dong DX, Yao SL, Yu N, Yang B. Systematic review and meta-analysis of Tianma Gouteng Yin combined with enalapril for essential hypertension. Zhongguo Zhong Yi Ji Zheng. 2011;20(5):762–764. [Google Scholar]
- 47.Zhang HW, Tong J, Zhou G, Jia H, Jiang JY. Tianma Gouteng Yin Formula for treating primary hypertension. Cochrane Database of Systematic Reviews. 2012;(6) doi: 10.1002/14651858.CD008166.pub2.CD008166 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Xu WJ, Li YL. Systematic review of clinical evidence about calm the liver and subdue yang therapy on the hypertension disease with syndrome of upper hyperactivity of liver yang. Zhonghua Zhong Yi Yao Za Zhi. 2012;27(3):736–739. [Google Scholar]
- 49.Shi M, Zhang YH. Systematic review of replenishing kidney qi method for essential hypertension with kidney qi deficiency syndrome. Shandong Zhong Yi Za Zhi. 2012;31(4):236–238. [Google Scholar]
- 50.Liu L, Li YL. Systematic review on treatment of essential hypertension from spleen and kidney deificency. Zhonghua Zhong Yi Yao Za Zhi. 2011;26(8):1700–1703. [Google Scholar]
- 51.Li DN, Yang CH. Effects of Chinese medicine on elderly isolated systolic hypertension: a meta-analysis. Liaoning Zhong Yi Za Zhi. 2012;39(5):812–815. [Google Scholar]
- 52.Zhao R, Fu LX, Xiong J, Li S, Wang ZL. The effect of acupuncture therapy on essential hypertension: a systematic review of long-term effect. Zhen Jiu Lin Chuang Za Zhi. 2011;27(3):46–51. [Google Scholar]
- 53.Kim JI, Choi JY, Lee H, Lee MS, Ernst E. Moxibustion for hypertension: a systematic review. BMC Cardiovascular Disorders. 2010;10, article 33 doi: 10.1186/1471-2261-10-33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Lee MS, Choi TY, Shin BC, Kim JI, Nam SS. Cupping for hypertension: a systematic review. Clinical and Experimental Hypertension. 2010;32(7):423–425. doi: 10.3109/10641961003667955. [DOI] [PubMed] [Google Scholar]
- 55.Lee MS, Pittler M, Guo RL, Ernst E. Qigong for hypertension: a systematic review of randomized clinical trials. Journal of Hypertension. 2007;25(8):1525–1532. doi: 10.1097/HJH.0b013e328092ee18. [DOI] [PubMed] [Google Scholar]
- 56.Guo XF, Zhou B, Nishimura T, Teramukai S, Fukushima M. Clinical effect of Qigong practice on essential hypertension: a meta-analysis of randomized controlled trials. The Journal of Alternative and Complementary Medicine. 2008;14(1):27–37. doi: 10.1089/acm.2007.7213. [DOI] [PubMed] [Google Scholar]
- 57.Li HG, Xu ZW. Systematic review of Tai Chi for essential hypertension. Wen Ti Yong Pin Yu Ke Ji. 2011;22(7):35–37. [Google Scholar]
- 58.Cheng JT. Review: drug therapy in Chinese traditional medicine. The Journal of Clinical Pharmacology. 2000;40(5):445–450. doi: 10.1177/00912700022009198. [DOI] [PubMed] [Google Scholar]
- 59.Wang J, Wang PQ, Xiong XJ. Current situation and re-understanding of syndrome and formula syndrome in Chinese medicine. Internal Medicine. 2012;2(3)1000113 [Google Scholar]
- 60.Xiong XJ, Chu FY, Li HX, He QY. Clinical application of the TCM classic formulae for treating chronic bronchitis. Journal of Traditional Chinese Medicine. 2011;31(1):69–72. doi: 10.1016/s0254-6272(11)60016-2. [DOI] [PubMed] [Google Scholar]
- 61.Xu H, Chen KJ. Progress, difficulty and countermeasure in treating hypertensive disease with integrated Chinese and Western medicine. Shi Jie Zhong Yi Yao. 2007;2(1):3–5. [Google Scholar]
- 62.Sackett DL, Straus SE, Richardson WS, Rosenberg W, Hanynes RB. Evidence Based Medicine: How To Practice and Teach EBM. 2nd edition. London, UK: Churchill Livingstone; 2000. [Google Scholar]
- 63.Xu H, Chen KJ. Making evidence-based decisions in the clinical practice of integrative medicine. Chinese Journal of Integrative Medicine. 2010;16(6):483–485. doi: 10.1007/s11655-010-0560-7. [DOI] [PubMed] [Google Scholar]
- 64.Braunwald E. The rise of cardiovascular medicine. European Heart Journal. 2012;33(7):838–845. doi: 10.1093/eurheartj/ehr452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Wang JY. Significance of evidence-based medicine in the assessment of Chinese medicine clinical efficacy. Chinese Journal of Integrative Medicine. 2010;16(5):392–393. doi: 10.1007/s11655-010-0533-x. [DOI] [PubMed] [Google Scholar]
- 66.Isaacs L. Alternative forms of medicine are becoming more popular, http://www.smudailymustang.com/?p=27201.
- 67.Xu X. Acupuncture in an outpatient clinic in China: a comparison with the use of acupuncture in North America. Southern Medical Journal. 2001;94(8):813–816. [PubMed] [Google Scholar]
- 68.Napadow V, Kaptchuk TJ. Patient characteristics for outpatient acupuncture in Beijing, China. The Journal of Alternative and Complementary Medicine. 2004;10(3):565–572. doi: 10.1089/1075553041323849. [DOI] [PubMed] [Google Scholar]
- 69.Kim SY, Chae Y, Lee SM, Lee H, Park HJ. The effectiveness of moxibustion: an overview during 10 years. Evidence-Based Complementary and Alternative Medicine. 2011;2011:19 pages. doi: 10.1093/ecam/nep163.306515 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Yamashita H, Ichiman Y, Tanno Y. Changes in peripheral lymphocyte subpopulations after direct moxibustion. The American Journal of Chinese Medicine. 2001;29(2):227–235. doi: 10.1142/S0192415X01000265. [DOI] [PubMed] [Google Scholar]
- 71.Lee MS, Kang JW, Ernst E. Does moxibustion work? An overview of systematic reviews. BMC Research Notes. 2010;3, article 284 doi: 10.1186/1756-0500-3-284. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Lauche R, Cramer H, Hohmann C, et al. The effect of traditional cupping on pain and mechanical thresholds in patients with chronic nonspecific neck pain: a randomized controlled pilot study. Evidence-Based Complementary and Alternative Medicine. 2012;2012:10 pages. doi: 10.1155/2012/429718.429718 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Kim JI, Lee MS, Lee DH, Boddy K, Ernst E. Cupping for treating pain: a systematic review. Evidence-Based Complementary and Alternative Medicine. 2011;2011:7 pages. doi: 10.1093/ecam/nep035.467014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Lee MS, Hong SS, Lim HJ, Kim HJ, Woo WH, Moon SR. Retrospective survey on therapeutic efficacy of Qigong in Korea. The American Journal of Chinese Medicine. 2003;31(5):809–815. doi: 10.1142/S0192415X03001442. [DOI] [PubMed] [Google Scholar]
- 75.Sancier KM, Holman D. Multifaceted health benefits of medical qigong. The Journal of Alternative and Complementary Medicine. 2004;10(1):163–165. doi: 10.1089/107555304322849084. [DOI] [PubMed] [Google Scholar]
- 76.Lee MS, Lee MS, Choi ES, Chung HT. Effects of Qigong on blood pressure, blood pressure determinants and ventilatory function in middle-aged patients with essential hypertension. The American Journal of Chinese Medicine. 2003;31(3):489–497. doi: 10.1142/S0192415X03001120. [DOI] [PubMed] [Google Scholar]
- 77.Lee MS, Lim HJ, Lee MS. Impact of qigong exercise on self-efficacy and other cognitive perceptual variables in patients with essential hypertension. The Journal of Alternative and Complementary Medicine. 2004;10(4):675–680. doi: 10.1089/acm.2004.10.675. [DOI] [PubMed] [Google Scholar]
- 78.Lee MS, Lee MS, Kim HJ, Choi ES. Effects of qigong on blood pressure, high-density lipoprotein cholesterol and other lipid levels in essential hypertension patients. International Journal of Neuroscience. 2004;114(7):777–786. doi: 10.1080/00207450490441028. [DOI] [PubMed] [Google Scholar]
- 79.Yeh GY, Wang C, Wayne PM, Phillips R. Tai Chi exercise for patients with cardiovascular conditions and risk factors: a systematic review. Journal of Cardiopulmonary Rehabilitation and Prevention. 2009;29(3):152–160. doi: 10.1097/HCR.0b013e3181a33379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Lee MS, Pittler MH, Taylor-Piliae RE, Ernst E. Tai Chi for cardiovascular disease and its risk factors: a systematic review. Journal of Hypertension. 2007;25(9):1974–1975. doi: 10.1097/HJH.0b013e32828cc8cd. [DOI] [PubMed] [Google Scholar]
- 81.Tsai JC, Wang WH, Chan P, et al. The beneficial effects of Tai Chi Chuan on blood pressure and lipid profile and anxiety status in a randomized controlled trial. The Journal of Alternative and Complementary Medicine. 2003;9(5):747–754. doi: 10.1089/107555303322524599. [DOI] [PubMed] [Google Scholar]
- 82.Xiong XJ, Wang J. Discussion of related problems in herbal prescription science based on objective indications of herbs. Journal of Chinese Integrative Medicine. 2010;8(1):20–24. doi: 10.3736/jcim20100104. [DOI] [PubMed] [Google Scholar]
- 83.Xu H, Chen KJ. Herb-drug interaction: an emerging issue of integrative medicine. Chinese Journal of Integrative Medicine. 2010;16(3):195–196. doi: 10.1007/s11655-010-0195-z. [DOI] [PubMed] [Google Scholar]
- 84.Xiong XJ, Wang J, He QY. Application status and safety countermeasures of traditional Chinese medicine injections. Journal of Chinese Integrative Medicine. 2010;8(4):307–311. doi: 10.3736/jcim20100402. [DOI] [PubMed] [Google Scholar]
- 85.Xu H, Chen KJ. Integrating traditional medicine with biomedicine towards a patient-centered healthcare system. Chinese Journal of Integrative Medicine. 2011;17(2):83–84. doi: 10.1007/s11655-011-0641-2. [DOI] [PubMed] [Google Scholar]
- 86.Xiong XJ, Wang J, He QY. Thinking about reducing adverse reactions based on idea of formula corresponding to syndromes. Zhongguo Zhong Yao Za Zhi. 2010;35(4):536–538. doi: 10.4268/cjcmm20100429. [DOI] [PubMed] [Google Scholar]
- 87.Shen ZY, Chen X. Analysis on 99 cases of adverse reactions of Chinese patent drugs. African Journal of Microbiology Research. 2012;6(8):1742–1746. [Google Scholar]
- 88.Wu YF, Huxley R, Li LM, et al. Prevalence, awareness, treatment, and control of hypertension in China data from the China National Nutrition and Health Survey 2002. Circulation. 2008;118(25):2679–2686. doi: 10.1161/CIRCULATIONAHA.108.788166. [DOI] [PubMed] [Google Scholar]
- 89.Sliwa K, Stewart S, Gersh BJ. Hypertension: a global perspective. Circulation. 2011;123(24):2892–2896. doi: 10.1161/CIRCULATIONAHA.110.992362. [DOI] [PubMed] [Google Scholar]
- 90.Mancia G, De Backer G, Dominiczak A, et al. Guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC) Journal of Hypertension. 2007;25(6):1105–1187. doi: 10.1097/HJH.0b013e3281fc975a. [DOI] [PubMed] [Google Scholar]
- 91.Alderman MH, Ogihara T. Global challenge for overcoming high blood pressure: fukuoka statement, 19 October 2006. Journal of Hypertension. 2007;25(3):p. 727. doi: 10.1097/HJH.0b013e3280961a1f. [DOI] [PubMed] [Google Scholar]
- 92.Ezzati M, Lopez AD, Rodgers A, Vander Hoorn S, Murray CJL. Selected major risk factors and global and regional burden of disease. The Lancet. 2002;360(9343):1347–1360. doi: 10.1016/S0140-6736(02)11403-6. [DOI] [PubMed] [Google Scholar]
- 93.Yach D, Hawkes C, Gould CL, Hofman KJ. The global burden of chronic diseases: overcoming impediments to prevention and control. Journal of the American Medical Association. 2004;291(21):2616–2622. doi: 10.1001/jama.291.21.2616. [DOI] [PubMed] [Google Scholar]
- 94.Liu MY, Chen KJ. Convergence: the tradition and the modern. Chinese Journal of Integrative Medicine. 2012;18(3):164–165. doi: 10.1007/s11655-012-1014-1. [DOI] [PubMed] [Google Scholar]
- 95.Xiong XJ. Study on the history of formulas corresponding to syndromes. Journal of Chinese Integrative Medicine. 2010;8(6):581–588. doi: 10.3736/jcim20100612. [DOI] [PubMed] [Google Scholar]
- 96.Lu AP, Chen KJ. Integrative medicine in clinical practice: from pattern differentiation in traditional Chinese medicine to disease treatment. Chinese Journal of Integrative Medicine. 2009;15(2):p. 152. doi: 10.1007/s11655-009-0152-6. [DOI] [PubMed] [Google Scholar]
- 97.Lu AP, Bian ZX, Chen KJ. Bridging the traditional Chinese medicine pattern classification and biomedical disease diagnosis with systems biology. Chinese Journal of Integrative Medicine. 2012;18(12):883–890. doi: 10.1007/s11655-012-1290-6. [DOI] [PubMed] [Google Scholar]
- 98.Wang J, Feng B, Yang XC, et al. Tianma gouteng yin as adjunctive treatment for essential hypertension: a systematic review of randomized controlled trials. Evidence-Based Complementary and Alternative Medicine. 2013;2013:18 pages. doi: 10.1155/2013/706125.706125 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Xiong XJ, Yang XC, Liu W, et al. Banxia baizhu tianma decoction for essential hypertension: a systematic review of randomized controlled trials. Evidence-Based Complementary and Alternative Medicine. 2012;2012:10 pages. doi: 10.1155/2012/271462.271462 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Chen KJ, Xie YH, Liu Y. Profiles of traditional Chinese medicine schools. Chinese Journal of Integrative Medicine. 2012;18(7):534–538. doi: 10.1007/s11655-012-1147-2. [DOI] [PubMed] [Google Scholar]
- 101.Xiong XJ, Wang J. Experience of diagnosis and treatment of exogenous high-grade fever. Journal of Chinese Integrative Medicine. 2011;9(6):681–687. doi: 10.3736/jcim20110616. [DOI] [PubMed] [Google Scholar]
- 102.Sun XG, Wu WK, Lu ZP. Chinese integrative medicine: translation toward person-centered and balanced medicine. Chinese Journal of Integrative Medicine. 2012;18(1):3–6. doi: 10.1007/s11655-012-0961-x. [DOI] [PubMed] [Google Scholar]
- 103.Dobos G, Tao I. The model of Western integrative medicine: the role of Chinese medicine. Chinese Journal of Integrative Medicine. 2011;17(1):11–20. doi: 10.1007/s11655-011-0601-x. [DOI] [PubMed] [Google Scholar]
- 104.Xiong XJ, Yang XC, Feng B, et al. Zhen gan xi feng decoction, a traditional Chinese herbal formula, for the treatment of essential hypertension: a systematic review of randomized controlled trials. Evidence-Based Complementary and Alternative Medicine. 2013;2013:9 pages. doi: 10.1155/2013/982380.982380 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Wang J, Yang XC, Feng B, et al. Is Yangxue Qingnao Granule combined with antihypertensive drugs, a new integrative medicine therapy, more effective than antihypertensive therapy alone in treating essential hypertension? Evidence-Based Complementary and Alternative Medicine. 2013;2013:8 pages. doi: 10.1155/2013/540613.540613 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Wang J, Yao KW, Yang XC, et al. Chinese patent medicine liu wei di huang wan combined with antihypertensive drugs, a new integrative medicine therapy, for the treatment of essential hypertension: a systematic review of randomized controlled trials. Evidence-Based Complementary and Alternative Medicine. 2012;2012:7 pages. doi: 10.1155/2012/714805.714805 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Wu AM, Zhang DM, Gao YH, et al. The correlation between high-sensitivity C-reactive protein, matrix metallopeptidase 9, and traditional Chinese medicine syndrome in patients with hypertension. Evidence-Based Complementary and Alternative Medicine. 2013;2013:8 pages. doi: 10.1155/2013/780937.780937 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Chen SL, Liu XY, Xu WM, Mei WY, Chen XL. Clinical study of Western medicine combined with Chinese medicine based on syndrome differentiation in the patients with polarized hypertension. Chinese Journal of Integrative Medicine. 2012;18(10):746–751. doi: 10.1007/s11655-012-1231-7. [DOI] [PubMed] [Google Scholar]
- 109.Janicki JS, Levick SP. The convergence of ancient Chinese medicine with modern therapeutics to prevent cardiac fibrosis. American Journal of Hypertension. 2012;25(2):p. 139. doi: 10.1038/ajh.2011.226. [DOI] [PubMed] [Google Scholar]
- 110.Liu W, Chen J, Xu T, Tian W, Li Y, Li WR. Qiliqiangxin improves cardiac function in spontaneously hypertensive rats through the inhibition of cardiac chymase. American Journal of Hypertension. 2012;25(2):250–260. doi: 10.1038/ajh.2011.219. [DOI] [PubMed] [Google Scholar]
- 111.Lei Y. Train of thought and strategy over strengthening the research of treating hypertension by integrative Chinese and Western medicine. Chinese Journal of Integrative Medicine. 2004;10(1):4–6. [Google Scholar]
- 112.Shi ZX. Train of thought about treatment of high blood pressure with integrative traditional and Western medicine. Chinese Journal of Integrative Medicine. 2004;10(1):2–4. [Google Scholar]
- 113.Zhao YH, Xu YH, Guan Y, Xiang P. Effects of Yinian Jiangya Decoction containing serum on cytokines secretion of vascular endothelium of spontaneously hypertensive rats. Chinese Journal of Integrative Medicine. 2010;16(4):344–347. doi: 10.1007/s11655-010-0524-y. [DOI] [PubMed] [Google Scholar]
- 114.Xiong XJ, Yang XC, Liu YM, Zhang Y, Wang PQ, Wang J. Chinese herbal formulas for treating hypertension in traditional Chinese medicine: perspective of modern science. Hypertension Research. 2013 doi: 10.1038/hr.2013.18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Junhua Z, Hongcai S, Xiumei G, et al. Methodology and reporting quality of systematic review/meta-analysis of traditional Chinese medicine. The Journal of Alternative and Complementary Medicine. 2007;13(8):797–805. doi: 10.1089/acm.2007.7195. [DOI] [PubMed] [Google Scholar]
- 116.Manheimer E, Wieland S, Kimbrough E, Cheng K, Berman BM. Evidence from the Cochrane Collaboration for traditional chinese medicine therapies. The Journal of Alternative and Complementary Medicine. 2009;15(9):1001–1014. doi: 10.1089/acm.2008.0414. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLOS Medicine. 2009;6(7) doi: 10.1371/journal.pmed.1000097.e1000097 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Wang J, Xiong XJ. Outcome measures of Chinese herbal medicine for hypertension: an overview of systematic reviews. Evidence-Based Complementary and Alternative Medicine. 2012;2012:7 pages. doi: 10.1155/2012/697237.697237 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119.Witt CM, Huang WJ, Lao LX, Berman BM. Which research is needed to support clinical decision-making on integrative medicine?—can comparative effectiveness research close the gap? Chinese Journal of Integrative Medicine. 2012;18(10):723–729. doi: 10.1007/s11655-012-1255-z. [DOI] [PubMed] [Google Scholar]
- 120.Tang JL. Some reflections on the evaluation of clinical effectiveness of Chinese medicine in China. Chinese Journal of Integrative Medicine. 2010;16(5):390–391. doi: 10.1007/s11655-010-0531-z. [DOI] [PubMed] [Google Scholar]