

Abstract
Objectives
The short-term effects of low-frequency repetitive transcranial magnetic stimulation (rTMS) in the patients with catastrophic and intractable tinnitus were investigated.
Methods
Fifteen participants were recruited among patients with catastrophic intractable tinnitus to receive 1 Hz rTMS treatment. Tinnitus severity was assessed before rTMS and directly after sham or real rTMS using the tinnitus handicap inventory (THI) and visual analog scale (VAS).
Results
There was no statistical difference in the THI score before and after sham stimulation. However, after 5 replications of real rTMS there was statistically significant reduction in THI score. Eight patients showed a decrease of more than 10 in THI score. Patients who showed a vast change in THI score after rTMS also showed a large decrease in their VAS score (r=0.879, P<0.001). Duration of tinnitus and change of THI score showed statistically significant moderate negative correlation (r=-0.637, P=0.011). But in case of VAS, there was no significant difference between VAS and duration of tinnitus.
Conclusion
Among total 15 patients with catastrophic intractable chronic tinnitus, eight patients showed some improvement in symptoms after 1 Hz rTMS. rTMS can be considered management modality for intractable tinnitus even with distress as severe as catastrophic stage.
Keywords: Tinnitus, Transcranial magnetic stimulation
INTRODUCTION
Tinnitus is a symptom characterized by recognizing sounds or noises in ears or brain without any external sound stimulation [1,2]. While it often develops in patients with hearing loss, it may occur also in patients with normal hearing [3]. Prevalence is reported at 10%-25%, with about 8% of sufferers having tinnitus too severe to maintain daily life [4]. It is thought that tinnitus is caused by changes in neuronal network including auditory and non-auditory systems [5].
Changes in neural activity related to tinnitus are not restricted in the auditory path and occur also in areas not related to the auditory system, such as frontal cortex, hippocampus, and amygdala [6]. It has been known that while auditory perception of tinnitus originates mainly in changes of central auditory system, tinnitus related distress is associated with changes of non-acoustic area [7].
Studies reporting neuronal activity of central auditory pathway by the electrical and functional imaging support these possible mechanisms [8]. Repetitive transcranial magnetic stimulation (rTMS) has been attempted conventionally as treatment of hallucination or writer's cramp and recently came into use as therapy for tinnitus [9]. Repetitive use of rTMS allows continuous changes of cortical excitability and can bring changes to neural excitability depending on stimulation parameter [10]. Although various parameters show different treatment results, they are effective in about 50% of patients [11]. To our knowledge there is no rTMS study on patients with catastrophic intractable chronic tinnitus who have severe distress and are not reactive to other treatments. Accordingly, this study is intended to identify if patients with catastrophic intractable chronic tinnitus can be improved by rTMS therapy, assessing short term therapeutic effects initially.
MATERIALS AND METHODS
Among patients who visited an out-patient clinic with chief complaint of tinnitus from October, 2010 to March, 2011, patients meeting the inclusion criteria were selected. The inclusion criteria include: 1) patients who had received medication such as alprazolam and/or tinnitus retraining therapy and/or had experienced use of sound generator or hearing aid for more than 6 months before, but showed no improvement in spite of these treatments; 2) tinnitus of more than 6 months' duration; 3) patients in catastrophic stage with a score of more than 78 points on tinnitus handicap inventory (THI) questionnaire for assessing distress in the pre-rTMS study; 4) patients who had no neurological diseases including previously diagnosed epilepsy, stroke, or intracranial abnormality; 5) patients who had no history of cardiac pacemaker, aneurysm clipping, or coil embolization; 6) patients who were over 18 years old; and 7) patients willing to undergo rTMS treatment.
Basic personal data such as age, sex, affected side and treatment modality used in conventional treatment, and treatment period were documented. Other symptoms including insomnia, dizziness, and ear fullness were identified.
All patients underwent two sessions of rTMS treatment. Sham rTMS was performed for 5 days from Monday to Friday in the first week, washout period lasted for 2 days, and then real rTMS was performed from Monday to Friday in the next week.
For sham rTMS, the coil was located between T3 and C3/T5 using 10-20 international electroencephalography (EEG) system, not contacting the scalp, tilted 90° vertically so that noise was similar, but the effect of magnetic field was delivered minimally to the cortex.
All patients were notified that treatment methods included sham rTMS, however, they did not know when the sham rTMS was used. By conducting coil angulation for sham rTMS, the patients were kept from recognizing these changes. In addition, they were used ear plugs for hearing protection.
THI questionnaire and visual analogue scale (VAS) for annoyance (able to assess up to 10 points) was used before and directly after sham rTMS and real rTMS both for evaluation of distress. All subjects gave written informed consent and this study was approved by the Ethics Committee of Kyung Hee University Hospital at Gangdong.
For delivery of rTMS, Magstim 200 (The Magstim Co., Whitland, UK) with figure-eight coil was used. The stimulation intensity was at 100% of the motor threshold, which was defined as the lowest intensity sufficient to produce left thenar muscle activation (magnetic evoked potentials>50 mV) with a single pulse delivered to the motor cortex in at least 5 of 10 trials. Location of coil was set to stimulate between T3 and C3/T5 using 10-20 international EEG system and the stimulation parameter was set up as 1 Hz and 1,200 times/day.
Statistical analysis was performed with nonparametric correlation analysis and Wilcoxon signed rank test using SPSS ver. 18.0 (SPSS Inc., Chicago, IL, USA) and was defined as significant at P-value less than 0.05.
RESULTS
A total of 15 patients satisfied the inclusion criteria. They included 8 males and 7 females by sex. Mean age was 53 years (range, 44 to 67 years) and duration was about 4 years (rage, 1.8 to 8 years). Eleven of fifteen patients complained of bilateral tinnitus. Insomnia was the most frequent associated symptom (Table 1).
Table 1.
Demographic data of patients
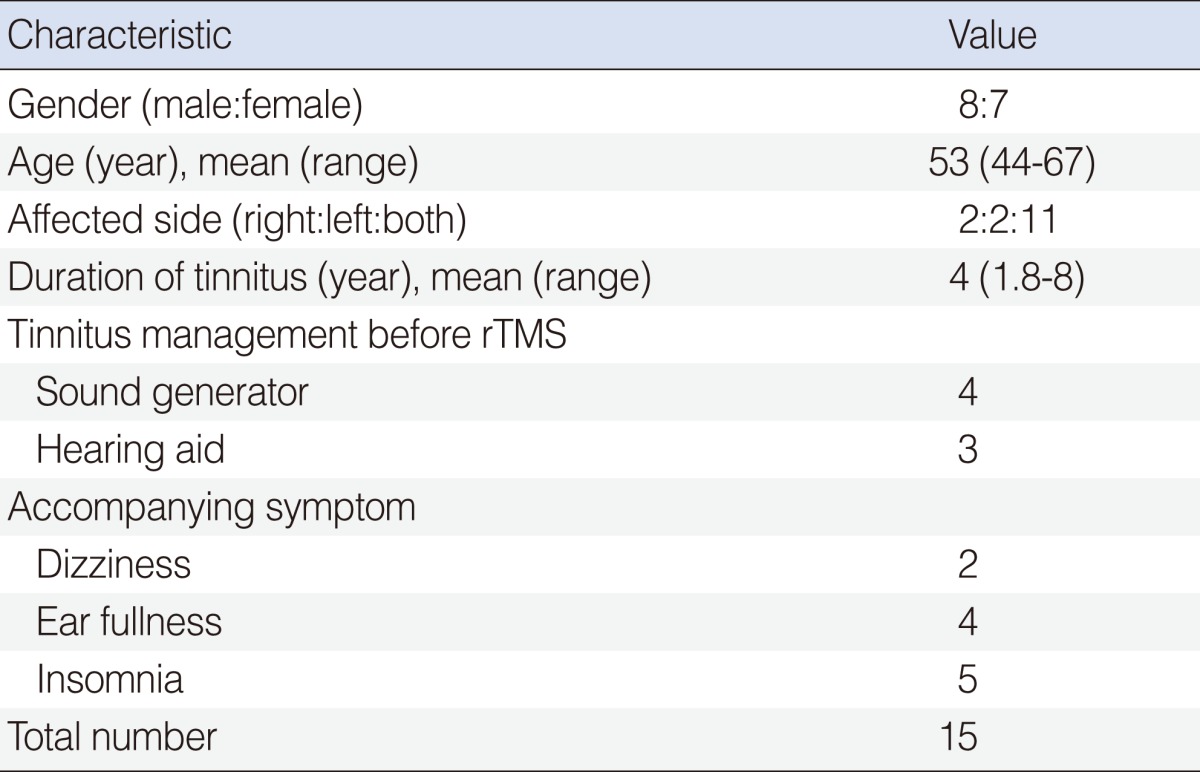
rTMS, repetitive transcranial magnetic stimulation.
Mean initial THI score (before sham rTMS) was 92.8, and after 5 replications of sham rTMS, mean THI score was 91.3, not a statistically significant change. The mean THI score after 5 replications of real rTMS was 81.6. This was a statistically significant reduction in THI score (Table 2).
Table 2.
Change of tinnitus after sham and real rTMS
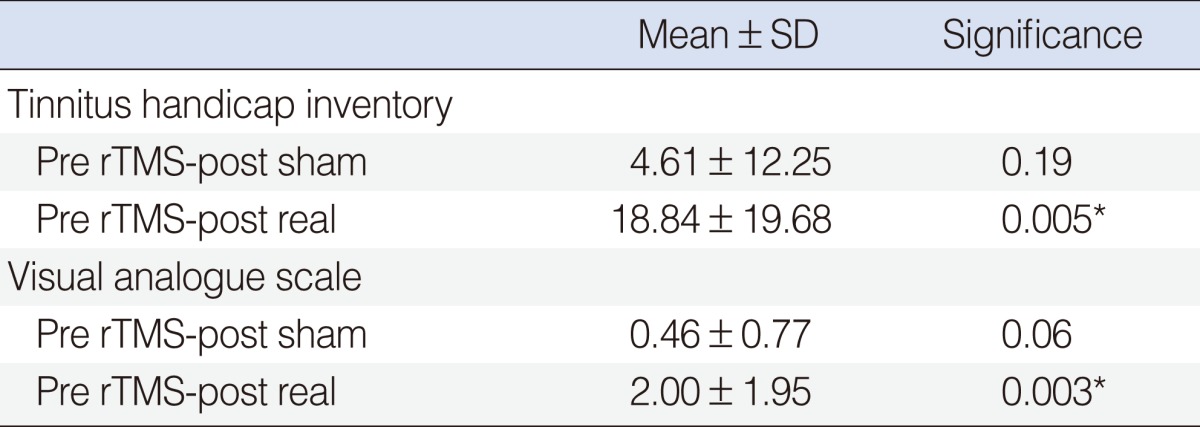
rTMS, repetitive transcranial magnetic stimulation.
*P<0.05
The mean VAS score was 8.6 before rTMS and 8.3 after 5 replications of sham rTMS, whereas 5 replications of real rTMS resulted in a mean score of 6.0. One patient had large reduction in VAS score after sham rTMS. In eight patients, it was found that real rTMS brought a reduction more than 3 points in VAS score. The average VAS score showed a significant reduction only after real rTMS (P=0.003) (Table 2).
There was a high positive correlation between change in THI score and VAS score after rTMS (r=0.879, P<0.001). There was good correlation between duration of tinnitus and change of VAS and THI score (Table 3). Although the duration of tinnitus and change of THI score were significantly moderately correlated (r=-0.637, P=0.011), the duration and change of VAS while showing a similar correlation (r=-0.478, P=0.071) did not reach statistical significance.
Table 3.
Tinnitus characteristics of patients
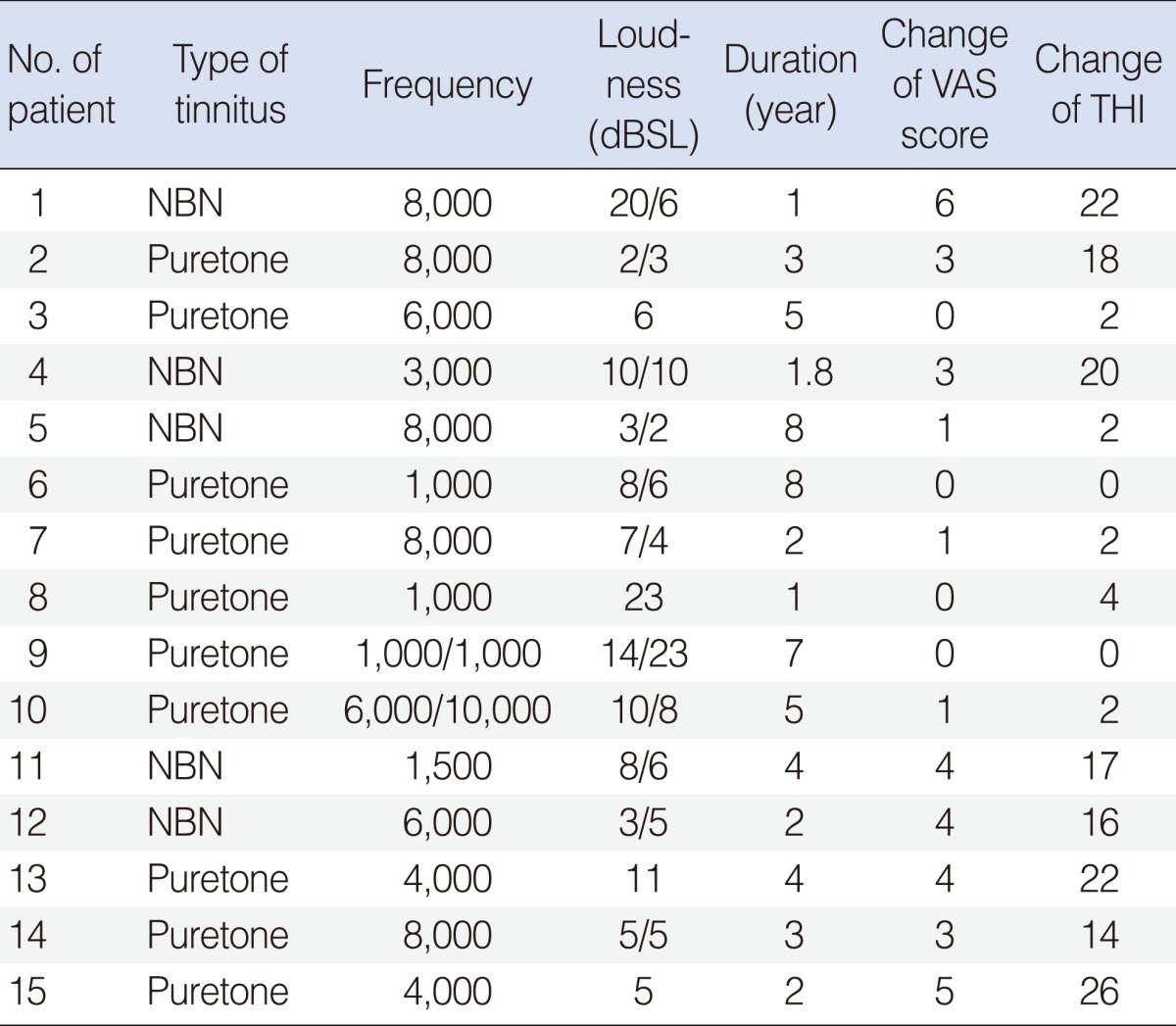
VAS, visual analogue scale; THI, tinnitus handicap inventory; NBN, narrow-band noise.
DISCUSSION
Tinnitus is considered an intractable disease [12]. Among therapeutic methods often attempted to patients with tinnitus, tinnitus retraining therapy (TRT) and cognitive behavioral therapy are well known, considered useful therapeutic methods to reduce negative effects of tinnitus in daily life by habituation [13,14].
Pathophysiologically, tinnitus is correlated with increased neural activity in non-classical pathway transcribed to secondary cortex and associated cortex, as well as in classical pathway transcribed to the primary auditory cortex, with eventual maladaptive plastic reorganization in several levels [15,16].
Low-frequency rTMS is a method to treat tinnitus by inhibiting neurological exciting of the cerebral cortex through electromagnetic stimulation different from TRT and cognitive behavior and is a more fundamental treatment when considering known pathophysiological aspects of tinnitus [8].
This study was conducted among patients with catastrophic and chronic tinnitus, who had been known to not respond to most conventional therapies excluding rTMS. The overall results showed reduction of tinnitus in most patients.
As far as we know, there are few studies on the analysis of therapeutic effect by tinnitus severity. That is why this study is novel. One study, analyzing fourteen patients with THI scores ranged from 40-70 reported no significant improvement in real rTMS versus placebo [17]. Another study, though it had a limitatition that it did not showed the range of baseline THI, showed significant improvement in twenty mild chronic patients with a mean THI of 29.8 after rTMS [18]. In addition to THI, the tinnitus questionnaire is frequently used in other studies to assess distress of tinnitus [19].
It is known that the rTMS can induce continuous changes in cortical excitability. Various effects has been reported, and factors affecting therapeutic results include morbid period of tinnitus, severity of deafness, cortical excitability, and metabolic activity of the stimulated area [7,10,11,20-22].
To select the stimulation location used in this study, 10-20 international EEG system was used, and to stimulate the same location, fixed cab was used to mark the stimulation area and stimulate between T3 and C3/T5. In the studies which used traditional positron emission tomography (PET), some studies stimulated the left auditory cortex since spontaneous neuronal activity on the left side increased regardless of direction of the tinnitus [19,22] while other studies reported that the opposite side should be stimulated since the opposite side of tinnitus perceiving side on functional magnetic resonance imaging (fMRI) taken after the stimulation was activated preferably [23,24].
Techniques for conducting rTMS are obviously still being researched, and additionally it is difficult to establish the direction of rTMS when the tinnitus is from both sides or cannot be determined exactly. Among the (severely affected) patients included in this study, the number patients complaining of both side tinnitus was 73.3% (11/15). The stimulation was given uniformly on left side auditory cortex. Results showed that many patients had reduction of tinnitus and THI score. However, small sample size restricted the statistical power to identify difference in effects for the stimulation direction, so further studies will be needed.
The audiological features of tinnitus of the study patients were as follows. It was found that most were in a form of pure tone corresponding to high frequency. The magnitude of tinnitus was ranged in 2-23 dBSL and its duration was 1-8 years depending on the patients (Table 3).
It is well known that longer duration of tinnitus is associated with worse prognosis [21,24]. There was no statistically significant difference between audiologic results and duration of the tinnitus. However, it appeared that shorter duration of tinnitus resulted in a larger change of THI, supporting prior study results. Similar findings for the VAS score did not reach statistical significance. Considering that the number of patients included in this study was relatively small and the subjective manner of VAS assessment, these doubtful points can be resolved through further research with larger numbers of patients.
This study is limited in that only short term effects immediately after rTMS were identified. In a study that had one year follow-up, it was assumed that high frequency rTMS had more consistent effects, and it was reported that 1 Hz rTMS showed relatively lower effect that was maintained for long term [23]. However, there was no study of patients with catastrophic intractable tinnitus showing severe distress as far as we know, and it seems that a large scale study to identify long term effects of this treatment is needed.
Another limitation of this study is the short wash-out period. Previous studies reported that long-term wash-out period is required to reduce carry-out effects [25], and at least two weeks of washout period are frequently used [26]. We cannot rule out an effect of the short washout period. However, we assumed that the effect of the first week treatment would not cause a cumulative effect, since sham rTMS preceded real rTMS. Nevertheless, a sufficient long-term washout period is important for study validity.
Among total 15 patients with catastrophic intractable chronic tinnitus, 8 patients showed some improvement in symptoms after 1 Hz rTMS. rTMS can be considered a management modality for intractrable tinnitus even with severe distress.
Footnotes
No potential conflict of interests relevant to this article was reported.
References
- 1.Jastreboff PJ. Phantom auditory perception (tinnitus): mechanisms of generation and perception. Neurosci Res. 1990 Aug;8(4):221–254. doi: 10.1016/0168-0102(90)90031-9. [DOI] [PubMed] [Google Scholar]
- 2.Andersson G, Lyttkens L. A meta-analytic review of psychological treatments for tinnitus. Br J Audiol. 1999 Aug;33(4):201–210. doi: 10.3109/03005369909090101. [DOI] [PubMed] [Google Scholar]
- 3.Zoger S, Svedlund J, Holgers KM. Relationship between tinnitus severity and psychiatric disorders. Psychosomatics. 2006 Jul-Aug;47(4):282–288. doi: 10.1176/appi.psy.47.4.282. [DOI] [PubMed] [Google Scholar]
- 4.Arnold W, Bartenstein P, Oestreicher E, Römer W, Schwaiger M. Focal metabolic activation in the predominant left auditory cortex in patients suffering from tinnitus: a PET study with [18F]deoxyglucose. ORL J Otorhinolaryngol Relat Spec. 1996 Jul-Aug;58(4):195–199. doi: 10.1159/000276835. [DOI] [PubMed] [Google Scholar]
- 5.Schlee W, Hartmann T, Langguth B, Weisz N. Abnormal resting-state cortical coupling in chronic tinnitus. BMC Neurosci. 2009 Feb;10:11. doi: 10.1186/1471-2202-10-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Lanting CP, de Kleine E, van Dijk P. Neural activity underlying tinnitus generation: results from PET and fMRI. Hear Res. 2009 Sep;255(1-2):1–13. doi: 10.1016/j.heares.2009.06.009. [DOI] [PubMed] [Google Scholar]
- 7.Langguth B, Kleinjung T, Landgrebe M, de Ridder D, Hajak G. rTMS for the treatment of tinnitus: the role of neuronavigation for coil positioning. Neurophysiol Clin. 2010 Mar;40(1):45–58. doi: 10.1016/j.neucli.2009.03.001. [DOI] [PubMed] [Google Scholar]
- 8.Bohning DE. Introduction and overview of TMS physics. In: George MS, Belmaker R, editors. Transcranial magnetic stimulation in neuropsychiatry. Washington, DC: American Psychiatric Press; 2000. pp. 13–44. [Google Scholar]
- 9.Hoffman RE, Cavus I. Slow transcranial magnetic stimulation, long-term depotentiation, and brain hyperexcitability disorders. Am J Psychiatry. 2002 Jul;159(7):1093–1102. doi: 10.1176/appi.ajp.159.7.1093. [DOI] [PubMed] [Google Scholar]
- 10.Frank G, Kleinjung T, Landgrebe M, Vielsmeier V, Steffenhagen C, Burger J, et al. Left temporal low-frequency rTMS for the treatment of tinnitus: clinical predictors of treatment outcome-a retrospective study. Eur J Neurol. 2010 Jul;17(7):951–956. doi: 10.1111/j.1468-1331.2010.02956.x. [DOI] [PubMed] [Google Scholar]
- 11.Langguth B, de Ridder D, Dornhoffer JL, Eichhammer P, Folmer RL, Frank E, et al. Controversy: does repetitive transcranial magnetic stimulation/transcranial direct current stimulation show efficacy in treating tinnitus patients. Brain Stimul. 2008 Jul;1(3):192–205. doi: 10.1016/j.brs.2008.06.003. [DOI] [PubMed] [Google Scholar]
- 12.Dobie RA. A review of randomized clinical trials in tinnitus. Laryngoscope. 1999 Aug;109(8):1202–1211. doi: 10.1097/00005537-199908000-00004. [DOI] [PubMed] [Google Scholar]
- 13.Jastreboff PJ, Jastreboff MM. Tinnitus retraining therapy: a different view on tinnitus. ORL J Otorhinolaryngol Relat Spec. 2006;68(1):23–30. doi: 10.1159/000090487. [DOI] [PubMed] [Google Scholar]
- 14.Londero A, Peignard P, Malinvaud D, Nicolas-Puel C, Avan P, Bonfils P. Contribution of cognitive and behavioral therapy for patients with tinnitus: implication in anxiety and depression. Ann Otolaryngol Chir Cervicofac. 2004 Dec;121(6):334–345. doi: 10.1016/s0003-438x(04)95531-4. [DOI] [PubMed] [Google Scholar]
- 15.Moller AR. Pathophysiology of tinnitus. Otolaryngol Clin North Am. 2003 Apr;36(2):249–266. doi: 10.1016/s0030-6665(02)00170-6. [DOI] [PubMed] [Google Scholar]
- 16.Eggermont JJ. Pathophysiology of tinnitus. Prog Brain Res. 2007;166:19–35. doi: 10.1016/S0079-6123(07)66002-6. [DOI] [PubMed] [Google Scholar]
- 17.Piccirillo JF, Garcia KS, Nicklaus J, Pierce K, Burton H, Vlassenko AG, et al. Low-frequency repetitive transcranial magnetic stimulation to the temporoparietal junction for tinnitus. Arch Otolaryngol Head Neck Surg. 2011 Mar;137(3):221–228. doi: 10.1001/archoto.2011.3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Marcondes RA, Sanchez TG, Kii MA, Ono CR, Buchpiguel CA, Langguth B, et al. Repetitive transcranial magnetic stimulation improve tinnitus in normal hearing patients: a double-blind controlled, clinical and neuroimaging outcome study. Eur J Neurol. 2010 Jan;17(1):38–44. doi: 10.1111/j.1468-1331.2009.02730.x. [DOI] [PubMed] [Google Scholar]
- 19.Kleinjung T, Eichhammer P, Langguth B, Jacob P, Marienhagen J, Hajak G, et al. Long-term effects of repetitive transcranial magnetic stimulation (rTMS) in patients with chronic tinnitus. Otolaryngol Head Neck Surg. 2005 Apr;132(4):566–569. doi: 10.1016/j.otohns.2004.09.134. [DOI] [PubMed] [Google Scholar]
- 20.De Ridder D, Verstraeten E, Van der Kelen K, De Mulder G, Sunaert S, Verlooy J, et al. Transcranial magnetic stimulation for tinnitus: influence of tinnitus duration on stimulation parameter choice and maximal tinnitus suppression. Otol Neurotol. 2005 Jul;26(4):616–619. doi: 10.1097/01.mao.0000178146.91139.3c. [DOI] [PubMed] [Google Scholar]
- 21.Khedr EM, Rothwell JC, El-Atar A. One-year follow up of patients with chronic tinnitus treated with left temporoparietal rTMS. Eur J Neurol. 2009 Mar;16(3):404–408. doi: 10.1111/j.1468-1331.2008.02522.x. [DOI] [PubMed] [Google Scholar]
- 22.Langguth B, Eichhammer P, Kreutzer A, Maenner P, Marienhagen J, Kleinjung T, et al. The impact of auditory cortex activity on characterizing and treating patients with chronic tinnitus: first results from a PET study. Acta Otolaryngol Suppl. 2006 Dec;(556):84–88. doi: 10.1080/03655230600895317. [DOI] [PubMed] [Google Scholar]
- 23.Smits M, Kovacs S, de Ridder D, Peeters RR, van Hecke P, Sunaert S. Lateralization of functional magnetic resonance imaging (fMRI) activation in the auditory pathway of patients with lateralized tinnitus. Neuroradiology. 2007 Aug;49(8):669–679. doi: 10.1007/s00234-007-0231-3. [DOI] [PubMed] [Google Scholar]
- 24.Kleinjung T, Steffens T, Sand P, Murthum T, Hajak G, Strutz J, et al. Which tinnitus patients benefit from transcranial magnetic stimulation? Otolaryngol Head Neck Surg. 2007 Oct;137(4):589–595. doi: 10.1016/j.otohns.2006.12.007. [DOI] [PubMed] [Google Scholar]
- 25.Londero A, Langguth B, De Ridder D, Bonfils P, Lefaucheur JP. Repetitive transcranial magnetic stimulation (rTMS): a new therapeutic approach in subjective tinnitus? Neurophysiol Clin. 2006 May-Jun;36(3):145–155. doi: 10.1016/j.neucli.2006.08.001. [DOI] [PubMed] [Google Scholar]
- 26.Rossi S, De Capua A, Ulivelli M, Bartalini S, Falzarano V, Filippone G, et al. Effects of repetitive transcranial magnetic stimulation on chronic tinnitus: a randomised, crossover, double blind, placebo controlled study. J Neurol Neurosurg Psychiatry. 2007 Aug;78(8):857–863. doi: 10.1136/jnnp.2006.105007. [DOI] [PMC free article] [PubMed] [Google Scholar]