

Abstract
Sialolipoma is a rare tumor found within both major and minor salivary glands. Here we discuss sialolipoma of the parotid gland and briefly review the English literature. Including our case, a total of 35 sialolipomas have been reported, 18 within major salivary glands and 17 within minor salivary glands. Major gland sialolipomas most often are presented in the parotid gland (77%) and those from minor glands were most often seen in the palate (41%). All lesions were well circumscribed and contained mature adipose tissue intimately admixed with benign salivary gland components. Ductal dilatation was found in 100% of minor salivary gland sialolipomas but in only 28% of major salivary gland tumors. Nerve entrapment has also rarely been noted in major salivary glands (14%) whereas myxoid degeneration has been identified in rare minor salivary glands tumors (13%). Treatment is surgical excision and is curative with no reports of recurrence.
Keywords: Lipoma, major salivary gland, minor salivary gland, parotid gland, sialolipoma
INTRODUCTION
Benign fatty tumors of parotid gland (lipomas) are very unusual, accounting for less than 0.5% of all parotid tumors. Despite infrequent numbers, numerous histological variants of salivary gland lipoma have been described. Sialolipoma, a new distinct variant, is characterized by proliferation of mature adipocytes with secondary entrapment of normal salivary gland elements.[1] A review of English scientific literature (PubMed) indicates 34 reported cases of sialolipoma, including 13 cases (38%) arising in the parotid gland,[2–5] followed by 7 cases (21%) in the palate. Here we report the 14th case of parotid gland sialolipoma.
CASE REPORT
A 69-year-old White male presented to the otolaryngology clinic with a right parotid mass of approximately 5-year duration, without history of xerostomia, salivary pain, odynophagia, dysphagia, weight loss, mouth pain, facial weakness, hemoptysis, infection, or conditions associated with immunodeficiency. Significant medical history included Type II diabetes, prostatic cancer, hypercholesterolemia, hypertension, and back pain. On examination, a 2×2 cm soft mass was palpated over the right parotid bed, which was nontender and mobile. Computed tomography (CT) scan showed a 1.9×2.3 cm encapsulated hypodense, hypoenhancing mass in the anterosuperior aspect of the right parotid gland [Figure 1]. The density of the mass was consistent with fat with intralesional heterogeneity. Fine needle aspiration was performed twice, but was nondiagnostic. The patient was treated surgically with a right superficial parotidectomy with facial nerve preservation.
Figure 1.
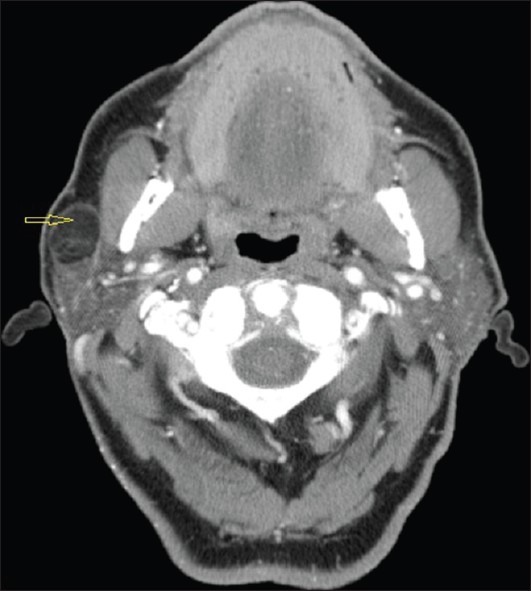
Axial CT neck showing a 19 × 23 mm well encapsulated mass in right anterior parotid bed. It has fat-like enhancement
On gross pathologic examination, a 2.7×2.2×1.5 cm well-circumscribed pale, firm soft tissue mass abutting the anterior margin of the specimen was noted. On microscopy a well-delineated lesion was observed, composed predominantly (75-90%) of mature adipose tissue with interspersed aggregates of oncocytic cells in small acini and clusters. A diagnosis of sialolipoma was rendered [Figures 2–4].
Figure 2.
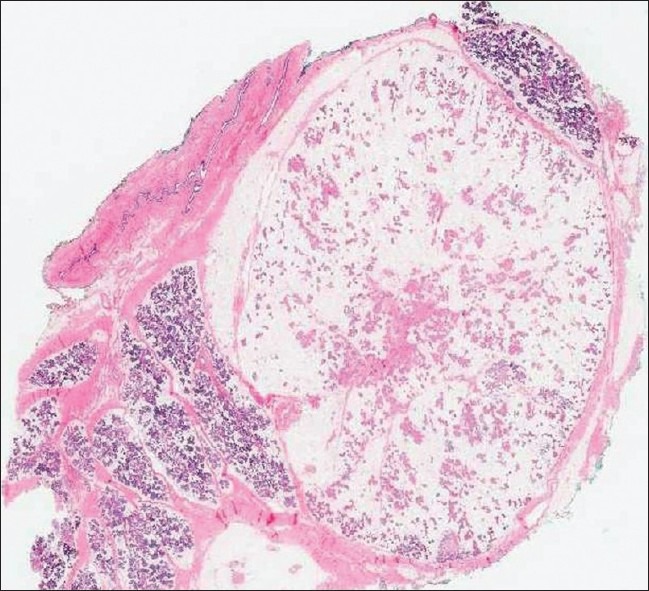
Image showing well demarcated mass with fat and admixed epithelial elements. (H and E, ×40)
Figure 4.
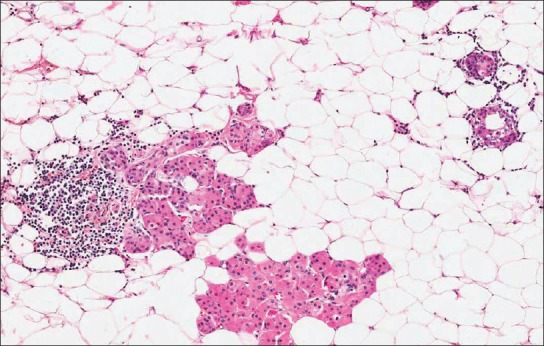
Image showing lesion with lymphocytic infiltrate and oncocytic metaplasia in a background of mature fat cells. (H and E, ×100)
Figure 3.
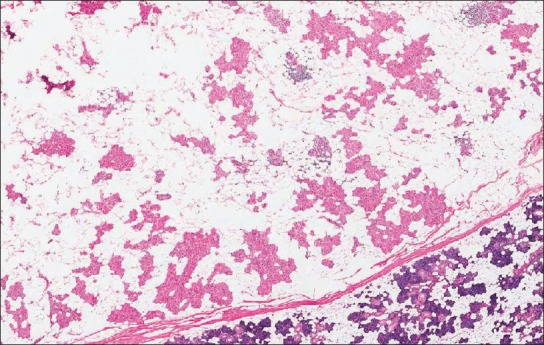
Image showing salivary gland elements with oncocytic change intermingled with mature adipose tissue, separated by fibrous capsule from normal parotid gland parenchyma. (H and E, ×200)
DISCUSSION
Sialolipoma is a relatively new histological variant of lipoma typified by benign salivary gland parenchyma intimately admixed with mature adipose tissue.[1] Our patient's clinical presentation of painless, slow growing, mobile mass with the microscopic findings of an encapsulated lesion with 75-90% of mature adipose tissue entrapping benign acinar and ductal cells and small lymphoid aggregates was consistent with the rendered diagnosis of sialolipoma.[1] Oncocytic metaplasia and mild to moderate lymphocytic infiltrate have previously been mentioned.[1,5,6] Glandular atrophy, periductal fibrosis, ductal dilatation and peripheral nerve involvement are additional features that have been reported in prior cases,[6] but were not present in our patient.
In a tabulated analysis of 35 cases (including our own), we compared the features of sialolipoma within major and minor salivary glands [Table 1].[1–6] The typical clinical presentation was that of a painless slow-growing mass, most commonly in parotid gland or palate. While the age distribution for major salivary gland sialolipomas was diverse (including four pediatric cases), minor salivary gland tumors were reported in adults only. Major salivary gland lesions were larger compared with minor salivary gland lesions, likely related to more room for the lesion to grow within the larger salivary gland prior to being noticed.
Table 1.
Comparison of sialolipomas originating in major and minor salivary glands
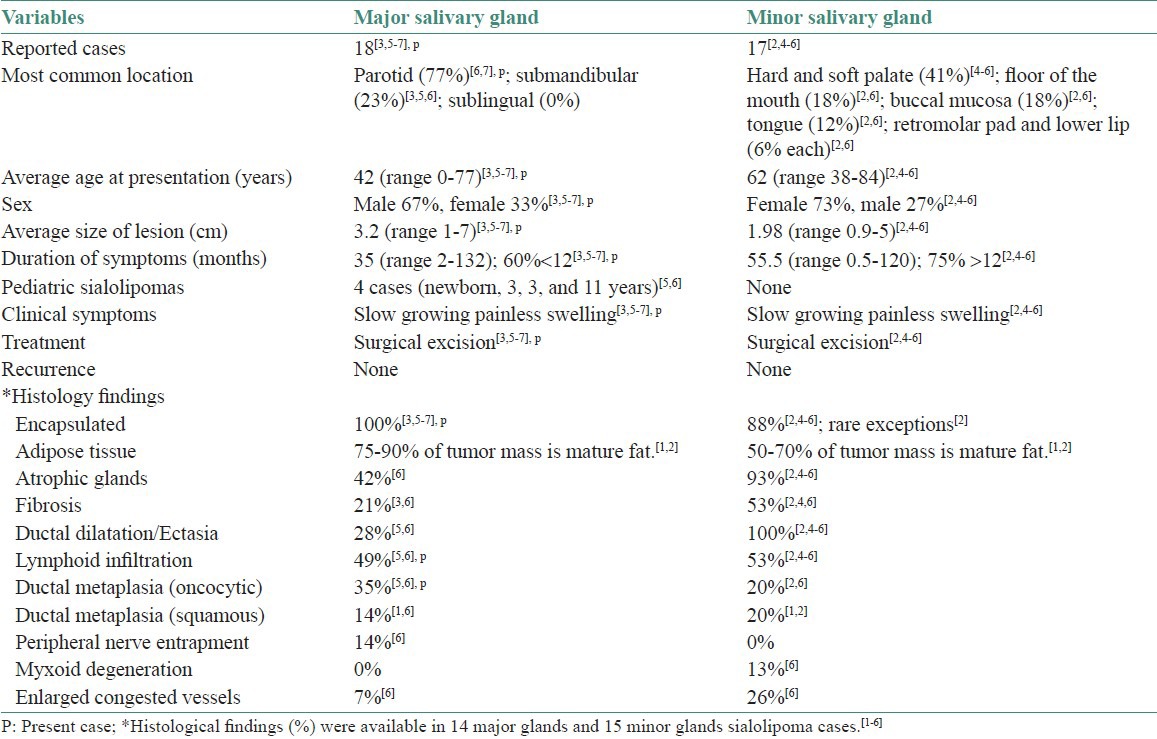
Histopathological features were also compared between major and minor salivary gland sialolipomas. Most lesions in either group were well circumscribed and contained mature fat intimately admixed with benign salivary gland components. Nerve entrapment was noted only in major salivary glands whereas myxoid degeneration was observed only in minor salivary gland tumors.
Akrish et al.[5] hypothesized that pathogenesis of sialolipoma may be associated with some form of salivary gland dysfunction, leading to altered salivary gland configuration. This concept is favored microscopically by replacement of the normal salivary gland tissue with mature adipose tissue admixed with atrophic salivary glandular elements, and/or chronic ductal epithelial changes (oncocytic metaplasia, fibrosis and lymphocytic infiltrate). Presence of similar histological findings in other conditions related to salivary gland dysfunction, for example, sialadenosis, senile, and reactive salivary gland changes further supports the above argument.[5]
The differential diagnosis of sialolipoma includes lipomatous lesions such as lipomatosis, lipoadenoma, and pleomorphic adenoma with an extensive fat constituent. CT or magnetic resonance imaging can be helpful in narrowing the differential diagnosis and are superior to ultrasonography in defining exact location and texture of the lesion. Fine needle aspiration, which is the first line procedure in diagnosing major salivary gland lesions is of little help, as its accuracy is less than 50% in lipomatous tumors.[3,6,7] Treatment of choice is surgical excision for both major and minor salivary glands sialolipomas. There are no reports of recurrence.[2]
Salivary gland neoplasms have a vast differential diagnosis. Physicians should be mindful of the possibility of sialolipoma, especially when CT scanning shows a well circumscribed fat-like tissue within the parotid gland.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Nagao T, Sugano I, Ishida Y, Asoh A, Munakata S, Yamazaki K, et al. Sialolipoma: A report of seven cases of a new variant of salivary gland lipoma. Histopathology. 2001;38:30–6. doi: 10.1046/j.1365-2559.2001.01054.x. [DOI] [PubMed] [Google Scholar]
- 2.Nonaka CF, Pereira KM, de Andrade Santos PP, de Almeida Freitas R, da Costa Miguel MC. Sialolipoma of minor salivary glands. Ann Diagn Pathol. 2011;15:6–11. doi: 10.1016/j.anndiagpath.2009.12.009. [DOI] [PubMed] [Google Scholar]
- 3.Sato K, Gotoh C, Uchida H, Kawashima H, Yoshida M, Kitano Y, et al. Sialolipoma of the submandibular gland in a child. J Pediatr Surg. 2011;46:408–10. doi: 10.1016/j.jpedsurg.2010.09.097. [DOI] [PubMed] [Google Scholar]
- 4.de Moraes M, de Matos FR, de Carvalho CP, de Medeiros AM, de Souza LB. Sialolipoma in minor salivary gland: Case report and review of the literature. Head Neck Pathol. 2010;4:249–52. doi: 10.1007/s12105-010-0187-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Akrish S, Leiser Y, Shamira D, Peled M. Sialolipoma of the salivary gland: Two new cases, literature review, and histogenetic hypothesis. J Oral Maxillofac Surg. 2011;69:1380–4. doi: 10.1016/j.joms.2010.05.010. [DOI] [PubMed] [Google Scholar]
- 6.Okada H, Yokoyama M, Hara M, Akimoto Y, Kaneda T, Yamamoto H. Sialolipoma of the palate: A rare case and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108:571–6. doi: 10.1016/j.tripleo.2009.05.045. [DOI] [PubMed] [Google Scholar]
- 7.Doğan S, Can IH, Unlü I, Süngü N, Gönültaş MA, Samim EE. Sialolipoma of the parotid gland. J Craniofac Surg. 2009;20:847–8. doi: 10.1097/SCS.0b013e3181a2ef7d. [DOI] [PubMed] [Google Scholar]