

Abstract
Introduction:
Coronary artery disease (CAD) is the leading cause of death and disability all over the world. A sedentary lifestyle and dyslipidemia are known to be the major risk factors, which play an important role in the progression of coronary artery disease. Regarding gender differences, the risk of developing coronary heart disease is recognized as being different between non-obese males and non-obese females. Hence, the aim of this study is to assess the benefits of a comprehensive cardiac rehabilitation program (CRP) on the functional capacity and lipid profiles, such as, total cholesterol, triglycerides, low density lipoprotein cholesterol, and high density lipoprotein cholesterol in non-obese males and non-obese females with coronary artery disease, and comparing these groups.
Materials and Methods:
We evaluated 585 non-obese males and females with coronary artery disease. All the participants completed the cardiac rehabilitation program for two months, which included 24 exercise training sessions, medical evaluation, and consultation. For investigation of the effects of the cardiac rehabilitation program on the functional capacity and lipid profiles, exercise tests were carried out by each patient, and also, their blood samples were taken on entrance and at the end of this period.
Results:
The findings, following 24 sessions in the cardiac rehabilitation program, showed that the functional capacity (P = 0.00) and all lipid profiles had significantly improved in both the groups, except that the high density lipoprotein cholesterol did not show a significant difference in non-obese females. In addition, comparing the two groups did not show any significant differences in lipid profiles, but the changes in functional capacity were significant (P = 0.00) between the two groups, following the cardiac rehabilitation program.
Conclusion:
The CRP, which was performed by the patients under supervision of a physician and an exercise physiologist, plays a key role in improving the functional capacity (FC) and all lipid profiles in non-obese males and females with coronary artery disease, without any attention to gender differences.
Keywords: Cardiac rehabilitation program, coronary artery disease, gender, risk factor
INTRODUCTION
Coronary artery disease (CAD) is the leading cause of death and disability in males and females in industrialized societies and developing countries.[1,2,3,4]
The major risk factors that play an important role in developing cardiovascular disease (CVD) are a sedentary lifestyle and hyperlipidemia, hypertension, smoking, obesity, and others. Several studies suggest that an increased level of total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), and a low level of high density lipoprotein cholesterol (HDL-C) are associated with a worse prognosis of coronary artery disease.[5,6]
Concerning gender differences, the risk of CVD progression is recognized to be different between males and females. According to a pervious study, CAD presents in males approximately 10 years earlier than in females;[7] and the incidence of coronary events is 60% higher in males than in females.[8] However, some studies reveal that females have similar improvements in functional capacity (FC) and risk factors compared to males, after the cardiac rehabilitation program.[6,9]
It was suggested that CRP, which is based on supervised exercise training, medical evaluation, risk factor modification, education, and consultation is particularly well suited to improve the functional capacity, and helps to prevent and treat many established cardiovascular risk factors.[2,10] A pervious study showed that CRP combined with resistance and aerobic training improved the exercise capacity by its beneficial effects on the skeletal muscle strength in patients with myocardial infarction.[11] Also, Afzalaghaiee suggested that CRP had useful effects on the lipid profiles in male and female patients with CAD.[12]
There are many investigations in this regard, but they have not paid any attention to the body mass index (BMI) in patients with CAD. So, the aim of this study is to assess the benefits of a comprehensive cardiac rehabilitation program on the functional capacity and lipid profiles in non-obese males and females with coronary artery disease, and in addition, to know if there is any difference between these groups?
MATERIALS AND METHODS
In an observational study between 2000 and 2011, we evaluated 585 non-obese patients with CAD, who referred to the Phase II Cardiac Rehabilitation Unit of the Isfahan Cardiovascular Research Institute. CAD was defined as a history of one of the following: Myocardial infarction (MI), coronary artery bypass grafting (CABG), percutaneous coronary intervention (PCI), or chronic stable angina. We elected these samples on the basis of their BMI. In fact, at first, the height and weight of each patient was measured by a nurse, and then the BMI was calculated by weight / height2 (kg / m2), and patients who had a BMI < 30 were enrolled in our investigation. Also, a blood sample was taken after 12 – 14 hours of fasting, for measuring serum lipids, including triglycerides (TG), total cholesterol (TC), and high-density lipoprotein cholesterol (HDL-C), using enzymatic methods, and low density lipoprotein cholesterol (LDL-C) was calculated according to the Friedewald formula.[13] All the patients used their angina treatment and the dose of these medications was not altered during the program. In addition, an exercise test with the protocol of Naughton was performed on each patient, under the supervision of a cardiologist. The exercise test provided an opportunity to evaluate the body reaction and FC. All the tests were assessed at the beginning of the study. Then the participants began CRP for two months, which consisted of 24 sessions, three times a week. CRP included exercise training sessions, nutritional and psychological consultation, and risk factor modification. Exercise training consisted of combined aerobic and resistance training and it was performed in the Cardiac Rehabilitation Center, under the supervision of a physician and an exercise physiologist, by using a treadmill, stationary cycles, stationary steppers, stair climbing, rowing, jogging, and some resistance devices. Each session lasted up to 90 minutes, with a 20-minute warm-up followed by 60 minutes of aerobic and resistance training, and finally 10 minutes of cool-down. The intensity of training was established according to the clinical condition and calculated between 60 and 85% of the maximum heart rate. Also, all the participants had dietary instructions given by a visiting dietitian in this duration. After passing two months and completing the rehabilitation program, all the tests were carried out by each patient for a second time. The patients were classified into two groups, which were known as the non-obese male and non-obese female groups. The research was conducted under the Medical Ethics Standards and approved by the Ethics Committee of the Isfahan Cardiovascular Research Institute. Independent sample t-tests were used to identify baseline differences and to compare the changes between the two groups. For investigation of changes between the baseline and completion of CRP, we used the paired t-tests. The results were expressed as mean and standard deviation (SD) and the level of significance was set at P < 0.05.
RESULT
In this study 585 male and female patients with CAD were evaluated, as their BMI was lower than 30kg/m2. The clinical and demographic characteristics of patients were mentioned in [Table 1]. Independent sample t-tests were used to identify the baseline differences among non-obese male and non-obese female patients [Table 2]. At baseline, the non-obese males had a higher functional capacity (P = 0.001), but TC and HDL-C were lower in males compared to females. Also, for examination of the changes between the baseline and completion of CRP, we used the paired sample t-tests [Table 3]. These tests revealed a significant improvement in all evaluated factors such as FC and lipid profiles in both the groups, except HDL-C, which did not have any significant change in non-obese females.
Table 1.
Clinical and demographic characteristics of patients
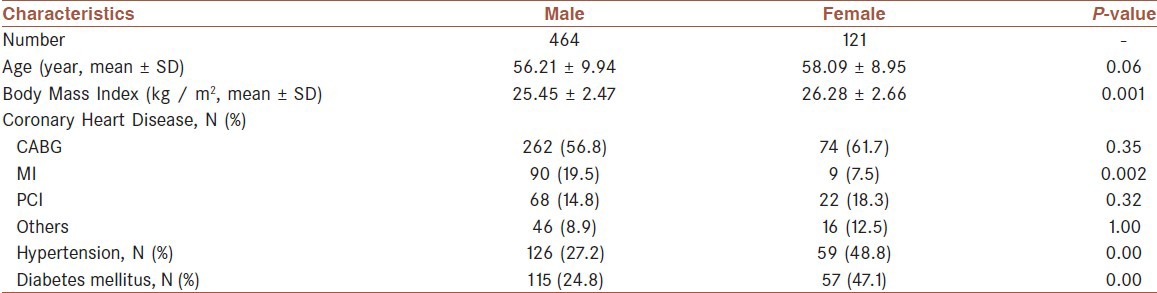
Table 2.
Comparison between non-obese males and non-obese females at baseline

Table 3.
Comparison of the changes within groups and between groups following the cardiac rehabilitation program

Finally, for comparing the changes between the two groups, independent sample t-tests were used and the data showed a significant difference only in FC between the two groups [Table 3].
DISCUSSION
Our finding revealed that eight-weeks of comprehensive cardiac rehabilitation had beneficial effects on FC enhancement and improvement of all lipid profiles in both non-obese male and non-obese female patients with CAD. Only in HDL-C we did not see any significant changes in non-obese females.
Many studies confirm our finding.[1,5,14,15] Plaza showed that patients who participated in the secondary prevention program experienced improvements in FC and lipid profiles.[16]
Also, the study of Sarrafzadegan suggested that comprehensive CRP has a beneficial effect on TC, TG, LDL, and HDL in Iranian cardiovascular patients even without using anti-lipid drugs.[2]
Yang's investigation showed that exercise interventions were useful for aerobic capacity, functional ability, and all lipid profiles, except HDL-C in patients, after stroke, with prior coronary artery disease.[17] Another article proved that CRP had an important impact on improving the functional capacity and decreasing the serum lipid profiles in coronary patients.[18]
Another study proposed that CRP played an important role in improving exercise tolerance and HDL-C levels in younger and older females with CVD.[19] Regarding no significant improvement being seen in HDL-C in non-obese females, we can state that a greater duration of exercise training and more attention to dietary restriction may have an effect on these patients and improve their HDL-C levels, significantly.
Concerning the FC, Jankowska implied that resistance training increased muscle strength and exercise capacity in patients with coronary heart failure.[20]
Additionally, an attributed study demonstrated a significant improvement in maximal, submaximal, and endurance exercise capacity following 12 weeks of exercise training in patients with heart failure.[21]
Also, another study that assessed FC by a six-minute walking test showed that CRP significantly improved the FC in patients after cardiac surgery.[10]
In addition, we compared the response of non-obese males and females to CPR and exercise training, and the results showed that except in FC, two groups did not have any significant differences. This meant that although there were significant differences between the two groups at baseline, after CRP, both of them benefited alike from the advantages of this period, but the males showed more improvement in FC compared to the females. In relation to this difference, we could imply that baseline differences in FC and BMI levels, as also the risk of hypertension and diabetes mellitus, which were higher in females than in males, could be causes for the differences in the FC, endurance, and fitness levels between non-obese males and females following CRP.
An attributed study, which assessed gender differences after CRP, showed that both genders benefited similarly from this program and they showed improvement in FC and lipid profiles.[22]
Similar to our finding, Schuster suggested that males were significantly better able to tolerate physical activity and had greater efficacy in enduring exercise and activities of daily living than females, following CRP.[23] On the contrary, Brochu revealed that neither male nor female patients obtained significant improvement in TC, LDL-C, or TG after the three-month exercise training alone.[24]
Another investigation showed that CRP and exercise training prevented and controlled the established cardiovascular risk factors, such as, high triglycerides, cholesterol concentrations, and low high-density lipoprotein cholesterol (HDL-C) concentrations, in patients with CAD.[3] In fact by CRP and exercise training, the cholesterol that sediments in muscles and vascular walls dissolves in the blood. Following this the liver removes this dissolved cholesterol from the blood and catabolizes it. Thus, this process leads to a decrease in the blood cholesterol levels.
Finally, we can state that regular physical training produces central and peripheral adaptations in the cardiac and skeletal muscles and vasculature that enhance FC and skeletal muscle strength. In fact, cardiac adaptations result in increased cardiac dimensions, stroke volume, and cardiac output that cause them to deliver more blood flow to the skeletal muscle, and the tissues receive adequate oxygen and these processes lead to an increase in aerobic capacity in the exercised muscle. On the other hand, vascular adaptations by increasing the density of skeletal muscle capillaries and improving endothelial-dependent vasodilatation in both epicardial and coronary arteries help in these progressions.[25,26]
CONCLUSION
According to our study we can notify that CRP, which is performed by patients under supervision of a physician and an exercise physiologist, plays a key role in improving FC and all lipid profiles in non-obese males and females with CAD, and the two groups did not have any significant difference in lipid profiles.
ACKNOWLEDGMENT
The authors thank all the physicians, nurses, and staff in the Cardiac Rehabilitation Center and Isfahan Cardiovascular Research Institute.
Footnotes
Source of Support: Isfahan Cardiovascular Research Institute
Conflict of Interest: None declared.
REFERENCES
- 1.Seki E, Watanabe Y, Shimada K, Sunayama S, Onishi T, Kawakami K, et al. Effects of a phase III cardiac rehabilitation program on physical status and lipid profiles in elderly patients with coronary artery disease. Circ J. 2008;72:1230–4. doi: 10.1253/circj.72.1230. [DOI] [PubMed] [Google Scholar]
- 2.Sarrafzadegan N, Rabieib K, Kabir A, Asgary S, Tavassoli A, Khosravi AR, et al. Changes in lipid profile of patients referred to a cardiac rehabilitation program. Eur J Cardiovasc Prev Rehabil. 2008;15:467–72. doi: 10.1097/HJR.0b013e328300271f. [DOI] [PubMed] [Google Scholar]
- 3.Ades PA. Cardiac rehabilitation and secondary prevention of coronary heart disease. N Engl J Med. 2001;345:892–902. doi: 10.1056/NEJMra001529. [DOI] [PubMed] [Google Scholar]
- 4.Barth J, Volz A, Schmid JP, Kohls S, Kanel R, Znoj H, et al. Gender differences in cardiac rehabilitation outcomes: Do women benefit equally in psychological health? J Womens Health. 2009;18:2033–9. doi: 10.1089/jwh.2008.1058. [DOI] [PubMed] [Google Scholar]
- 5.Warner JG, Brubaker PH, Zhu Y, Morgan TM, Ribisl PM, Miller HS, et al. Long-term (5-year) changes in HDL cholesterol in cardiac rehabilitation patients (do sex differences exist.)? Circulation. 1995;92:773–7. doi: 10.1161/01.cir.92.4.773. [DOI] [PubMed] [Google Scholar]
- 6.Mosca L, Manson J, Sutherland SE, Langer RD, Manolio T, Barrett-Connor E. Cardiovascular disease in women: A statement for healthcare professionals from the American Heart Association. Circulation. 1997;96:2468–82. doi: 10.1161/01.cir.96.7.2468. [DOI] [PubMed] [Google Scholar]
- 7.Wake R, Yoshiyama M. Gender differences in ischemic heart disease. Recent Pat Cardiovasc Drug Discov. 2009;4:234–40. doi: 10.2174/157489009789152249. [DOI] [PubMed] [Google Scholar]
- 8.Izawa KP, Oka K, Watanabe S, Yokoyama H, Hiraki K, Morio Y, et al. Gender related differences in clinical characteristic and physiological and psychological outcomes of Japanese patients at entry into phase II cardiac rehabilitation. J Rehabil Med. 2008;40:225–30. doi: 10.2340/16501977-0156. [DOI] [PubMed] [Google Scholar]
- 9.Cannistra LB, Balady GJ, O’Malley CJ, Weiner DA, Ryan TJ. Comparison of the clinical profile and outcome of women and men in cardiac rehabilitation. Am J Cardiol. 1992;69:1274–9. doi: 10.1016/0002-9149(92)91220-x. [DOI] [PubMed] [Google Scholar]
- 10.Esteki Ghashghaei F, Sadeghi M, Marandi M, Esteki Ghashghaei S. Exercise-based cardiac rehabilitation improves hemodynamic responses after coronary artery bypass graft surgery. ARYA Atheroscler. 2011:7. [PMC free article] [PubMed] [Google Scholar]
- 11.Kida K, Osada N, Akashi YJ, Sekizuka H, Omiya K, Miyake F. The exercise training effects of skeletal muscle strength and muscle volume to improve functional capacity in patients with myocardial infarction. Int J Cardiol. 2008;129:180–6. doi: 10.1016/j.ijcard.2008.04.031. [DOI] [PubMed] [Google Scholar]
- 12.Afzalaghaiee E, Hadian MR, Attarbashi Moghadam B, Tavakol K, Zandparsa AF, Jalaei S, et al. The effects of cardiac rehabilitation on changes in the lipid profile of Iranian male and female with coronary artery disease refered to Emam Khomeini Hospital complex. Mod Rehabil. 2010;4:45–50. [Google Scholar]
- 13.Friedewald WT, Levy RI, Fridrikson DS. Estimation of concentrations oflow-density lipoprotein cholesterol in plasma without use of preparativeultracentrifuge. Clin Chem. 1972;18:499–502. [PubMed] [Google Scholar]
- 14.Leon SA, Franklin AB, Costa F, Balady JG, Berra AK, Stewart J, et al. An American Heart Association Scientific Statement from the Council on Clinical Cardiology (Subcommittee on Exercise, Cardiac Rehabilitation, and Prevention) and the Council on Nutrition, Physical Activity, and Metabolism (Subcommittee on Physical Activity), in collaboration with the American Association of Cardiovascular and Pulmonary Rehabilitation. Circulation. 2005;111:369–76. doi: 10.1161/01.CIR.0000151788.08740.5C. [DOI] [PubMed] [Google Scholar]
- 15.Fard NM, Zadegan NS, Sajadi F, Rafiei M, Abdar N. Effect of cardiac rehabilitation on lipid profile. J Assoc Physicians India. 2003;51:12–5. [PubMed] [Google Scholar]
- 16.Plaza I, García S, Madero R, Zapata MA, Perea J, Sobrino JA, et al. Secondary prevention program: Impact on cardiovascular risk. Rev Esp Cardiol. 2007;60:205–8. [PubMed] [Google Scholar]
- 17.Yang AL, Lee SH, Su CT, Wang JL, Lin KL. Effects of exercise intervention on patients with stroke with prior coronary artery disease: Aerobic capacity, functional ability and lipid profile: A pilot study. J Rehabil Med. 2007;39:88–90. doi: 10.2340/16501977-0021. [DOI] [PubMed] [Google Scholar]
- 18.Toufan M, Afrasiabi A. Benefits of cardiacrehabilitation on lipidprofile in patients with coronary artery disease. Pak J Biol Sci. 2009;12:1307–13. doi: 10.3923/pjbs.2009.1307.1313. [DOI] [PubMed] [Google Scholar]
- 19.Kennedy MD, Haykowsky M, Daub B, Van Lohuizen K, Knapik G, Black B. Effects of a comprehensive cardiac rehabilitation program on quality of life and exercise tolerance in women. A retrospective analysis. Curr Control Trials Cardiovasc Med. 2003;4:1–6. doi: 10.1186/1468-6708-4-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Jankowska EA, Wegrzynowska K, Superlak M, Nowakowska K, Lazorczyk M, Biel B, et al. The 12-week progressive quadriceps resistance training improves muscle strength, exercise capacity and quality of life in patients with stable chronic heart failure. Int J Cardiol. 2008;130:36–43. doi: 10.1016/j.ijcard.2007.07.158. [DOI] [PubMed] [Google Scholar]
- 21.Larsen AL, Aarsland T, Kristiansen M, Haugland A, Dickstein K. Assessing the effect of exercise training in men with heart failure. Comparison of maximal, submaximal and endurance exercise protocols. Eur Heart J. 2001;22:684–92. doi: 10.1053/euhj.2000.2286. [DOI] [PubMed] [Google Scholar]
- 22.Sarrafzadegan N, Rabiei K, Kabir A, Sadeghi M, Khosravi A, Asgari S, et al. Gender differences in risk factors and outcomes after cardiac rehabilitation. Acta Cardiol. 2008;63:763–70. doi: 10.2143/AC.63.6.2033395. [DOI] [PubMed] [Google Scholar]
- 23.Schuster PM, Waldron J. Gender differences in cardiac rehabilitation patients. Rehabil Nurs. 1991;16:248–53. doi: 10.1002/j.2048-7940.1991.tb01229.x. [DOI] [PubMed] [Google Scholar]
- 24.Brochu M, Poehlman ET, Savage P, Fragnoli-Munn K, Ross S, Ades PA. Modest effects of exercise training alone on coronary risk factors and body composition in coronary patients. J Cardiopulm Rehabil. 2000;20:180–8. doi: 10.1097/00008483-200005000-00006. [DOI] [PubMed] [Google Scholar]
- 25.Ades PA, Waldmann ML, Meyer WL. Skeletal muscle and cardiovascular adaptations to exercise conditioning in older coronary patients. Circulation. 1996;94:323–30. doi: 10.1161/01.cir.94.3.323. [DOI] [PubMed] [Google Scholar]
- 26.Hambrecht R, Wolf A, Gielen S, Geilen S, Hamann C, Kaiser R, et al. Effect of exercise on coronary endothelial function in patients with coronary artery disease. N Engl J Med. 2000;342:454–60. doi: 10.1056/NEJM200002173420702. [DOI] [PubMed] [Google Scholar]