

Abstract
Background:
Anterior fixation using two 3.5 mm screws is typically recommended for type II odontoid fractures. However, it is unsuitable in patients with an odontoid diameter of <9.0 mm. There is no data regarding the morphology of odontoid process in the Indian population. The aim of our study was to: a) Measure the external diameters of odontoid process in the Indian population using CT scan and thus determine the feasibility of two 3.5 mm screw fixation in them. b) Determine if any correlation exists between body height (Ht) and weight (Wt) and external odontoid diameters.
Materials and Methods:
CT images of odontoid process of 100 consecutive patients were analyzed. Antero- posterior (AP) and transverse (TD), outer diameters of the odontoid process were measured from the base and at 1 mm interval upwards on axial CT images.
Results:
The mean AP and mean TD were 11.52 mm and 9.85 mm, respectively. Fifty-five (55%) of the patients had at least one TD <9.0 mm. Five (5%) patients had at least one TD <7.4 mm. None of the patients had any diameter <5.5 mm. Body Ht correlated significantly with mean AP and mean TD of the odontoid process (AP: r = 0.276, P = 0.013; TD: r = 0.359, P = 0.001), whereas body Wt correlated significantly only with mean TD (AP: r = 0.162, P = 0.15; TD: r = 0.297, P = 0.007).
Conclusion:
More than half of the study population (55%) was unsuitable for two 3.5 mm screw fixation for type II odontoid fracture. Two 2.7 mm screws can be safely used in 95% of the population. A 4.5 mm Herbert screw can be safely used in the entire population. We recommend two 2.7 mm screws or a 4.5 mm Herbert screw for fixation of these fractures in the Indian population. Body height showed a significant correlation with external odontoid diameters, whereas weight showed significant correlation only with TD of the odontoid process.
Keywords: Indian population, internal fixation, odontoid morphology, odontoid process, type II odontoid fracture
INTRODUCTION
Fractures of the odontoid process at its junction with the body are the commonest odontoid fractures.1 Management of these fractures has evolved from external immobilization, through C1- C2 fusion to anterior screw fixation.1,2,3 When managed only with external immobilization, these are associated with high incidence of nonunion, neck stiffness, atlanto- axial instability and cervical myelopathy.1,4 C1-C2 fusion is associated with loss of up to 50% rotation and 10% flexion extension at the cervical spine.2,5,6 Anterior screw fixation for these fractures can preserve C1-C2 mobility and can be considered as a treatment of choice.4,7,8 Though, initial reports suggested use of two small fragment screws for fixation of odontoid fractures,8,9,10,11 subsequent reports have shown that the dimensions of odontoid process might be too narrow to accommodate two screws in a large section of the population.3,6,7,12,13 Moreover, morphometric analyses of pedicles of dorsolumbar spine have shown significant differences between the Caucasian and Indian population.14 This may significantly influence the method of internal fixation of odontoid fractures in the Indian population. To the best of our knowledge, there is no data regarding odontoid morphology in the Indian population. Thus, the aim of our study was a) to measure the external diameters of odontoid process in the Indian population using CT scan, b) to determine the feasibility of two 3.5 mm screw fixation and thus, recommend a safe method of fixation of type II odontoid fractures in the Indian population and c) to determine if any correlation exists between body height (Ht) and weight (Wt) and external odontoid diameters.
MATERIALS AND METHODS
Institutional Review Board's (IRB) approval was obtained prior to the commencement of the study. Cervical spine CT scans in 100 consecutive patients, who were undergoing CT for an unrelated clinical problem during 2008-09 were analyzed. Sample size representative of a large population was calculated at 95% confidence interval and with a margin of error <0.1. All patients were above 18 years of age and those with atlanto-axial pathology were excluded from the study. CT scans were performed with a 64-detector CT scanner [Somatom Sensation 64, Siemens, Erlangen, Germany; Software: Somaris/5 Syngo CT, 2006 (A)]. Postprocessing and analysis was performed on Wizard (Siemens) workstation. Axial sections of the odontoid process were taken at the base and at 1 mm intervals upward. The base of the odontoid process was defined as the lowermost axial CT picture, with most well- delineated odontoid image [Figure 1]. Antero-posterior (AP) and Transverse (TD) outer diameters of the odontoid process were measured at each of these levels with the help of digital callipers. These measurements represent the actual dimensions of the odontoid process. Internal fixation of the odontoid process using screws is based on the principle of interfragmentary compression, achieved by the ‘lag screw effect’. Lag screw fixation requires tapping the far cortex- the ‘thread hole’. The outer diameter of the odontoid process is relevant when screws are inserted after tapping.12 Hence, we measured the outer diameters of odontoid process in our study. All measurements were made perpendicular to the long axis of the odontoid process. As sections were made from the base upwards, there was a decreasing trend in both the AP and the TD of odontoid process [Figure 2] till the waist was reached [Figure 3]. For practical purposes, the waist of the odontoid process was defined as the level with narrowest TD. As sections were taken above the waist, there was now an increasing trend in both the AP and the TD, confirming the location of the waist [Figures 1–4].
Figure 1.
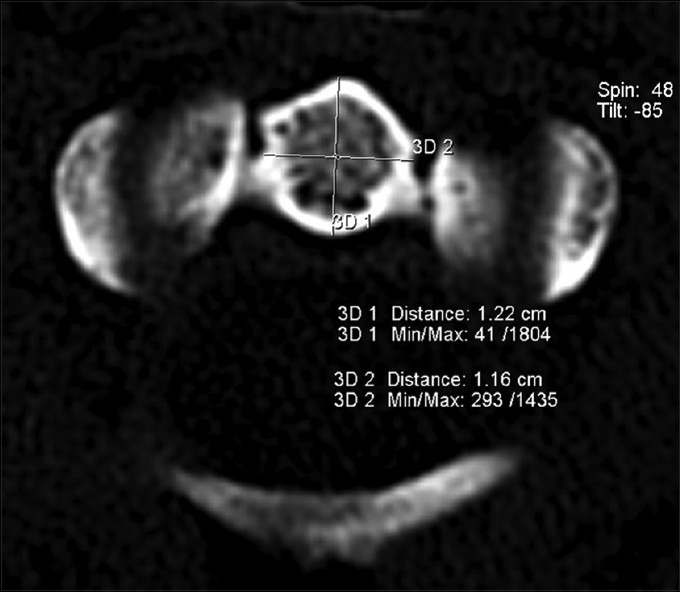
Axial CT image at the level of base of the odontoid process, showing AP (3D1) and TD (3D2) dimensions
Figure 2.
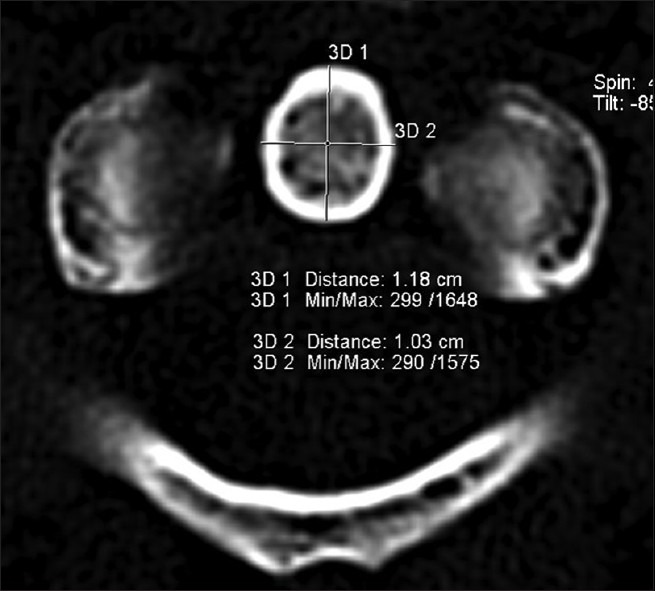
Axial CT image at 2 mm from the base, showing decrease in AP and TD
Figure 3.
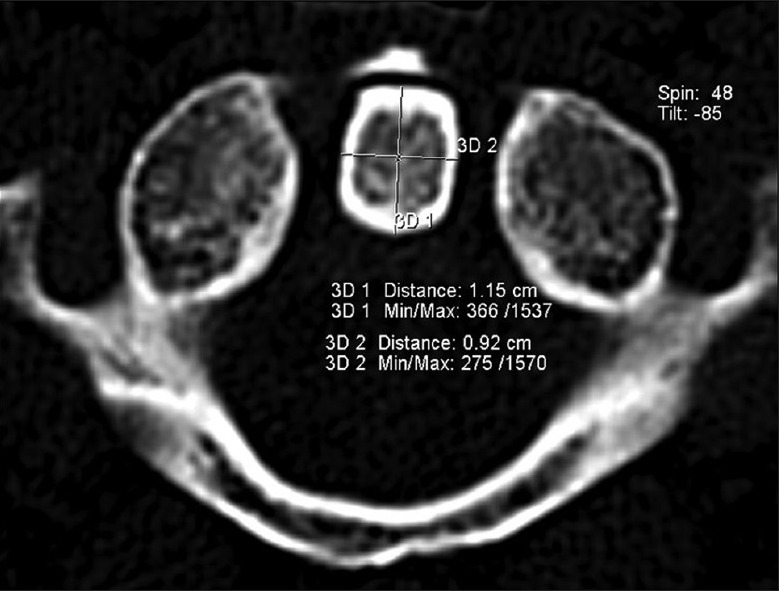
Axial CT image at 4 mm from the base, showing the narrowest TD (Waist)
Figure 4.
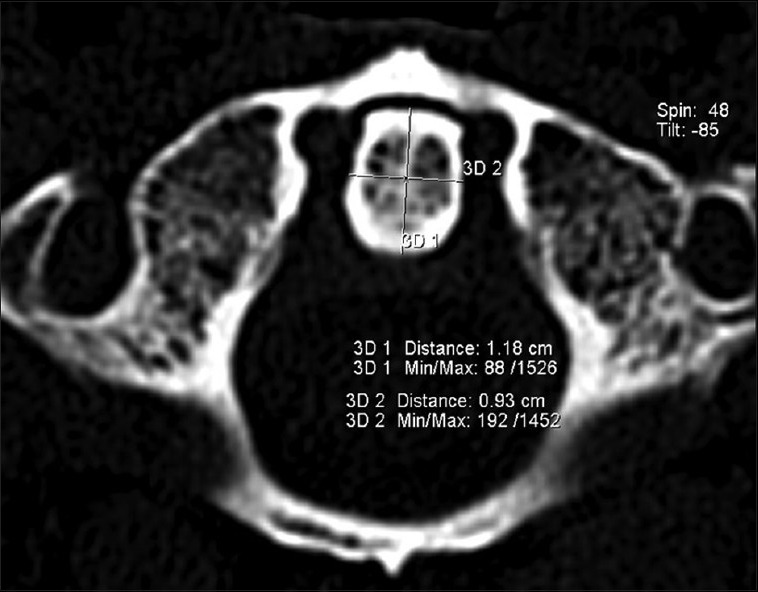
Axial CT image at 1 mm above the waist, showing an increase in AP and TD, confirming the location of the waist
Comparison of mean odontoid dimensions between groups was performed using Student t-test. Qualitative data was analyzed using ‘Fisher's exact test’ or the ‘Chi-squared test’. Correlation between body height and weight with odontoid dimensions was determined using ‘Pearson's correlation co-efficient’. Statistical analysis was carried out using SPSS statistics software (version 17.0, Chicago, IL). ‘P’ values <0.05 and <0.001 were considered ‘significant’ and ‘highly significant’ respectively.
RESULTS
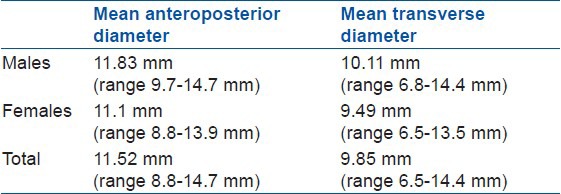
The mean age of the population was 52.14 years (range 19-88 years, SD 15.53 years). Fifty eight (58%) were males (mean age 51.88 years, range 19-85 years, SD 17.65 years) and 42 (42%) were females (mean age 52.5 years, range 27-88 years, SD 12.2 years). The distribution of age in the two sexes was comparable (P = 0.8447). The mean AP and mean TD [Table 1] of the odontoid process were 11.83 mm (range 9.7-14.7 mm, SD: 0.89 mm) and 10.11 mm (range 6.8-14.4 mm, SD 0.90 mm) respectively in males and 11.1 mm (range 8.8-13.9 mm, SD 0.79 mm) and 9.49 mm (range 6.5-13.5 mm, SD 0.79 mm) respectively in females. The difference between mean diameters of males and females was highly significant (AP: P < 0.0001; TD: P = 0.0005). Mean AP and mean TD of the entire population were 11.52 mm (range 8.8-14.7 mm, SD 0.92 mm) and 9.85 mm (range 6.5-14.4 mm, SD 0.90 mm) respectively. The difference between mean AP and mean TD was highly significant (P < 0.0001). Fifty five (55%) patients had at least one TD < 9.0 mm. This proportion was significantly greater in the females (26/58- males, 29/42- females, P = 0.0246). Five (5%) patients had at least one TD < 7.4 mm and these proportions were not significantly different between the two sexes (1/58- male, 4/42- females, P = 0.1689). None of the patients had any diameter <5.5 mm. Each of the 2 (2%) patients, had one AP diameter <9.0 mm; but the proportions were not significantly different between the two sexes (0/58- male, 2/42- females, P = 0.1739).
Table 1.
The mean anteroposterior and transverse diameter of the odontoid process
Correlation of body height and weight with mean AP and mean TD of the odontoid process was assessed in 80 patients (n = 80; M:F = 46:34) [Table 2]. We found a significant positive correlation of body height with mean AP and mean TD of the odontoid process (height with mean AP: r = 0.276, P = 0.013; height with mean TD: r = 0.359, P = 0.001). Though body weight showed significant positive correlation with mean TD of the odontoid process, it did not correlate significantly with the mean AP diameter (weight with mean TD: r = 0.297, P = 0.007; weight with mean AP: r = 0.162, P = 0.15). The following table shows correlation of body height and weight with mean AP and mean TD of the odontoid process, in our population.
Table 2.
Correlation of height and weight with anteroposterior and transverse diameter of the odontoid process

DISCUSSION
Anderson and D’ Alonzo type II, are the commonest odontoid fractures.1 Internal fixation for odontoid fractures without compromising C1- C2 motion was initially reported by Bohler et al.,9 and Nakanishi et al.,10 Several authors have shown comparable union rates between anterior screw fixation and C1- C2 fusion.3,9,15 Theoretically, two screws afford better stability and avoid rotation that may occur during or after insertion of a single screw.5,6,7 However, insertion of the second screw can be technically difficult.2,3 Moreover, the odontoid process might be too narrow to accommodate two screws in a substantial section of the population.6,7,12,13
The TD of odontoid process is more relevant than the AP, as two screws are usually placed in the coronal plane. The minimum TD that can safely accommodate two 3.5 mm screws is 9.0 mm.12 Though 95% of the odontoid processes in the Caucasian population could safely accommodate two 3.5 mm screws,12 33% of the Malaysian7 and 35% of the Brazilian13 population was unsuitable for the same. This number was as high as 55% in our study population.
If two 3.5 mm screw fixation is contemplated when one or more TD is <9.0 mm, it can be done by changing the orientation of the two screws. If none of the AP diameters is less than 9.0 mm, two 3.5 mm screws can be placed in the odontoid process in the sagittal plane.7 This however, is a technically demanding procedure that is not commonly performed.
To overcome the difficulty with two 3.5 mm screws in narrow odontoid processes use of two 2.7 mm screws is recommended by some authors.7,12,16 Two 2.7 mm screws can be safely placed in the odontoid process, if none of the TD < 7.4 mm.7 Barring a small fraction (5%), two 2.7 mm screws can be safely used in almost all the patients, in our population. In a prospective review of 30 patients (German population) with a type II odontoid fracture who were managed with two 2.7 mm screws, no nonunions or major complications were reported. However, the authors did admit that the dual screw technique is technically challenging.16
In a biomechanical study, Sasso et al., showed that there is no significant difference in the strength of fixation between one and two screws.5 They believed that the interdigitation of the fracture site appears to be more important for fracture stability than the number of screws. Subsequent clinical studies showed comparable union rates between two and one screw fixation.2,3,4 However, screw breakage was seen in 10% cases, when a single screw was used for fixation.2 This resulted in union of the odontoid process in a retrospondylolisthesis position.2
Recently, a 4.5 mm cannulated Herbert screw has been introduced for fixation of these fractures. In a biomechanical study, a 4.5 mm Herbert screw was shown to have significantly greater torsional stiffness and greater shear stiffness, when compared to two 3.5 mm screws.17 The compressive force generated by a 4.5 mm Herbert screw, was two times greater than a 3.5 mm cannulated screw.18 Union rates with a 4.5 mm Herbert screw are comparable to two screw fixation.19 There is no report of implant failure associated with a 4.5 mm Herbert screw, as against a single 3.5 mm screw.2,19 Considering that a minimum of 0.5 mm rim of normal bone must be present around the screw, a 4.5 mm Herbert screw can be safely placed, if none of the TD < 5.5 mm. Since none of the TD was <5.5 mm in our population, it can be safely used in the entire population.
We found a significant correlation between body height and mean AP and TD of the odontoid process; and body weight and mean TD of the odontoid process, unlike other authors. They did not find any significant correlation between body height and weight and external diameters of the odontoid process.6,7 We believe that a larger sample size may perhaps help, establish a significant correlation between body weight and mean AP diameter also, which we have not been able to establish currently. In view of considerable variability in the dimensions of the odontoid process, like other authors, we also believe that a preoperative CT scan can help determine the method of fixation, its safety and feasibility.6,7,20
To conclude, more than half of our study population (55%) is not suitable for two 3.5 mm screw fixation, for type II odontoid fracture. Two 2.7 mm screws can be safely used in 95% of the population. A 4.5 mm Herbert screw, can be safely used in the entire population. We recommend two 2.7 mm screws or a 4.5 mm Herbert screw for fixation of these fractures in the Indian population. These recommendations may also apply to other populations of the Indian subcontinent who are likely to have a narrower odontoid process than the Caucasians. A preoperative CT scan can help determine the appropriate method of fixation and its safety. Body height showed significant positive correlation with mean AP and mean TD of the odontoid process. Though, we found significant positive correlation of body weight with mean TD only, we believe that a larger sample size may help establish its correlation with mean AP diameter too.
Footnotes
Source of Support: Nil
Conflict of Interest: None
REFERENCES
- 1.Anderson LD, D’ Alonzo RT. Fractures of the odontoid process of the axis. J Bone Joint Surg Am. 1974;56:1663–74. [PubMed] [Google Scholar]
- 2.Jenkins JD, Coric D, Branch CL. A clinical comparison of one and two screw odontoid fixation. J Neurosurg. 1998;89:366–70. doi: 10.3171/jns.1998.89.3.0366. [DOI] [PubMed] [Google Scholar]
- 3.Esses SI, Bednar DA. Screw fixation of odontoid fractures and nonunions. Spine (Phila Pa 1976) 1991;16(Suppl 10):S483–5. doi: 10.1097/00007632-199110001-00005. [DOI] [PubMed] [Google Scholar]
- 4.Henry AD, Bohly J, Grosse A. Fixation of odontoid fractures by an anterior screw. J Bone Joint Surg Br. 1999;81:472–7. doi: 10.1302/0301-620x.81b3.9109. [DOI] [PubMed] [Google Scholar]
- 5.Sasso R, Doherty BJ, Crawford MJ, Heggeness MH. Biomechanics of odontoid fracture fixation. Spine (Phila Pa 1976) 1993;18:1950–3. doi: 10.1097/00007632-199310001-00004. [DOI] [PubMed] [Google Scholar]
- 6.Schaffler MB, Alson MD, Heller JG, Garfin SR. Morphology of the Dens. Spine (Phila Pa 1976) 1992;17:738–43. doi: 10.1097/00007632-199207000-00002. [DOI] [PubMed] [Google Scholar]
- 7.Yusof MI, Yusof AH, Abdullah MS, Hussain TM. Computed tomographic evaluation of the odontoid process for two screw fixation in type II fracture: A Malaysian perspective. J Orthop Surg (Hong Kong) 2007;15:67–72. doi: 10.1177/230949900701500115. [DOI] [PubMed] [Google Scholar]
- 8.Jeanneret B, Vernet O, Frei S, Magerl F. Atlantoaxial mobility after screw fixation of the odontoid: A computed tomographic study. J Spinal Disord. 1991;4:203–11. doi: 10.1097/00002517-199106000-00011. [DOI] [PubMed] [Google Scholar]
- 9.Bohler J. Anterior stabilization for acute fractures and nonunions of the dens. J Bone Joint Surg Am. 1982;6:18–27. [PubMed] [Google Scholar]
- 10.Nakanishi T, Sasaki T, Tokita N, Hirabayashi K. Internal fixation for the odontoid fracture. Orthop Trans. 1982;6:176. [Google Scholar]
- 11.Aebi M, Etter C, Coscia M. Fractures of the odontoid process: Treatment with anterior screw fixation. Spine (Phila Pa 1976) 1989;14:1065–70. doi: 10.1097/00007632-198910000-00007. [DOI] [PubMed] [Google Scholar]
- 12.Nucci RC, Seigal S, Merola AA, Gorup J, Mroczek KJ, Dryer J, et al. Computed tomographic evaluation of the normal adult odontoid: Implications for internal fixation. Spine (Phila Pa 1976) 1995;20:264–70. doi: 10.1097/00007632-199502000-00002. [DOI] [PubMed] [Google Scholar]
- 13.Daher MT, Daher S, Nogueira-Barbosa MH, Defino HL. Computed tomographic evaluation of odontoid process: Implications for anterior screw fixation of odontoid fractures in an adult population. Eur Spine J. 2011;20:1908–14. doi: 10.1007/s00586-011-1879-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Chadha M, Balain B, Maini L, Dhaon BK. Pedicle morphology of the lower thoracic, lumbar and S1 vertebrae: An Indian perspective. Spine (Phila Pa 1976) 2003;28:744–9. [PubMed] [Google Scholar]
- 15.Apuzzo ML, Heiden JS, Weiss MH, Ackerson TT, Harvey JP, Kurze T. Acute fractures of the odontoid process: An analysis of 45 cases. J Neurosurg. 1978;48:85–91. doi: 10.3171/jns.1978.48.1.0085. [DOI] [PubMed] [Google Scholar]
- 16.El Saghir H, Bohm H. Anderson type II fracture of the odontoid process: Results of anterior screw fixation. J Spinal Disord. 2000;13:527–31. doi: 10.1097/00002517-200012000-00011. [DOI] [PubMed] [Google Scholar]
- 17.McBride AD, Mukherjee DP, Kruse RN, Albright JA. Anterior screw fixation of type II odontoid fractures: A biomechanical study. Spine (Phila Pa 1976) 1995;20:1855–60. doi: 10.1097/00007632-199509000-00001. [DOI] [PubMed] [Google Scholar]
- 18.Shaw JA. Biomechanical comparison of cannulated small bone screws: A brief followup study. J Hand Surg Am. 1991;16:998–1001. doi: 10.1016/s0363-5023(10)80058-9. [DOI] [PubMed] [Google Scholar]
- 19.Lee SH, Sung JK. Anterior Odontoid fixation using a 4.5 mm Herbert screw: The first report of 20 consecutive cases with Odontoid fracture. Surg Neurol. 2006;66:361–6. doi: 10.1016/j.surneu.2006.04.018. [DOI] [PubMed] [Google Scholar]
- 20.Xu R, Nadaud MC, Ebraheim NA, Yeasting RA. Morphology of the second cervical vertebra and posterior projection of the C2 pedicle axis. Spine (Phila Pa 1976) 1995;20:259–63. doi: 10.1097/00007632-199502000-00001. [DOI] [PubMed] [Google Scholar]