

Abstract
Objectives
Whole Body Vibration (WBV) devices are used as a means to augment training, and their potential to treat a range of musculoskeletal diseases and injuries is now being considered. The goal of this work is to determine the degree to which acceleration delivered by WBV devices at the plantar surfaces of a standing human is transmitted through the axial and appendicular skeleton, and how this mechanical challenge corresponds to the safety Threshold Limit Values (TLV) established by the International Standards Organization ISO-2631.
Design
Non-blinded laboratory assessment of a range of WBV devices as it pertains to acceleration transmission to healthy volunteers.
Methods
Using skin and bite-bar mounted accelerometers, transmissibility to the tibia and cranium was determined in six healthy adults standing on a programmable WBV device as a function of frequency and intensity. Measures of transmissibility were then made from three distinct types of WBV platforms, which delivered a 50-fold range of peak-to-peak acceleration intensities (0.3 to 15.1g p-p; where 1g is earth’s gravitational field).
Results
For a given frequency, transmissibility was independent of intensity when below 1g. Transmissibility declined non-linearly with increasing frequency. Depending on the WBV device, vibration ranged from levels considered safe by ISO-2631 for up to eight hours each day (0.3gp-p @ 30Hz), to levels that were seven times higher than what is considered a safe threshold for even one minute of exposure each day (15.1g p-p @ 30Hz). Transmissibility to the cranium was markedly attenuated by the degree of flexion in the knees.
Conclusions
Vibration can have adverse effects on a number of physiologic systems. This work indicates that readily accessible WBV devices markedly exceed ISO guidelines for safety, and extreme caution must be practiced when considering their use.
Keywords: Back Pain, Muscle Strength, Rehabilitation, Physical Therapy, Injury, Sports Medicine
Introduction
For decades, attempts have been made to limit exposure of the human body to vibration, as these mechanical signals are readily recognized as a major contributor to a multitude of diseases and ailments, including low-back pain,1 circulatory disorders,2 and neural dysfunction.3 Despite tremendous efforts to minimize the amplitude and duration of work-place exposure to limb-specific or whole body vibration,4 occupational exposure to vibration continues to produce adverse health conditions in many workers, including pronounced lower back pain, hearing loss, blurred vision and chronic nerve and vascular damage to arms and hands.5 So severe is the potential damage to organs and tissues that advisories for human tolerance limits for vibration have been introduced by the International Organization for Standardization,6 in essence a warning which urges stringent oversight of duration limits as prescribed by Threshold Limit Values (ISO-TLV) for a given intensity of vibration. These guidelines are endorsed by the U.S. Occupational Safety and Health Association (OSHA) and the National Institute for Occupational Safety and Health (NIOSH), who work towards reducing acute and chronic injuries ascribed to vibration in the environment and workplace.
Despite strong advisories to limit human exposure to vibration, there is growing interest in the voluntary use of Whole Body Vibration (WBV) as a surrogate or supplement for exercise,7 as well as an intervention in preventative medicine or physical therapy.8 Consideration in this regard should not be particularly surprising, given the musculoskeletal system’s strong sensitivity to mechanical loading,9 whether WBV is used to strengthen the elite athlete7 or augment rehabilitation10 in the injured or infirm. As demonstrated in animal models, WBV introduced in the range of 20 to 90 Hz is anabolic to bone and muscle, and can prevent and reverse osteoporosis in these preclinical models as introduced by disuse, age, or endocrine dysfunction.11, 12
Translated to the clinic, there is early – albeit inconclusive – evidence that WBV may someday be used as a non-drug therapy for the treatment of musculoskeletal injury and/or disease. Using extremely low-magnitude, (0.3 g, where 1 g = earth’s gravitational field), 30 Hz vibrations have been shown as anabolic to bone and muscle in the hip and spine of young women with osteoporosis,13 promote volumetric bone density in the proximal tibia of children with disabling conditions such as cerebral palsy,14 enhance bone quality in adolescents with idiopathic scoliosis,15 and help protect balance control in those subject to chronic bed rest.16 Using WBV at much greater magnitudes (7.4g), a six-month study has shown in post-menopausal women that vibration can also inhibit the progression of osteoporosis.17 But is the potential risk of vibration exposure worth the potential reward?
WBV devices are readily available to the general public, but concern for their safety has only recently been apparent,18, 19 with recommendations which call for the requirement of 1:1 supervision from those trained in the use of these devices.20 Google-based internet searches on WBV devices identify close to 50 distinct devices from around the world that are readily available for immediate shipping, but very few of the key vibration characteristics of the devices provided.
Without knowledge of the intensity of the acceleration delivered by the WBV device, it is impossible to extrapolate how close a platform approaches the ISO-TLV. The majority of WBV web-sites provide no more than DISPLACEMENT (D) and/or the FREQUENCY (Hz) at which a platform might operate. However, ISO-TLV focuses on the INTENSITY of the vibration, which is reported in “g”, or g-force, as calculated by:
Without addressing the efficacy of any of these devices, the work presented here was designed to quantify the vibration exposure delivered by three distinct WBV platforms available on the market, and report the results with respect to the TLV advisories made on human exposure limits to vibration as determined by ISO-2631.
Methods
This study was reviewed and approved by the Stony Brook University’s Committee on Research in Human Subjects. Investigators ran the study with the understanding that ISO-2631 guidelines advised against even brief exposure beyond extremes of the TLV boundaries. Six young, active, healthy adults were recruited from the undergraduate and graduate student population at Stony Brook University through campus postings.
Tri-axial accelerometers, sensitive within the range of ± 10g (CXL10HF3 Crossbow Technology Inc., California), each weighing 27 grams, were used to measure transmission of plantar based WBV to specific weight bearing regions of the volunteers as they stood through a range of flexed-knee positions. Acceleration measurements were made at the medial aspect of the proximal tibia, 10cm below the knee, affixing an accelerometer to the skin with two-sided adhesive tape, covered by elastic wrap. Despite the limitations of skin-mounted accelerometers,21 they provide an accurate first-order approximation of vibration.22 Acceleration at the cranium was approximated by attaching the accelerometer to a bite bar, which was clenched between molars. An accelerometer was also fixed to the top surface of the WBV platform, to determine the specific amount of acceleration delivered by the device.
Accelerometers were connected to a National Instruments SCXI-1000 data acquisition system through a SCXI-1531 8 channel Accelerometer Input Module (National Instruments Corp., TX), connected to a laptop using a DAQCard-6036E 16 Input 200 kS•s−1 acquisition card. A custom LABVIEW 7.1 program collected 15 second samples, at 1000Hz, data from the three accelerometers, in all three planes. Accelerometer output was digitized and reported as g-force, where:
The signal was filtered with a 30Hz band pass filter centered on the primary frequency to remove high frequency noise and low frequency signal drift due to the volunteer’s postural motions.16 Average peak to peak (p-p) acceleration was calculated from the filtered signal, while RMS acceleration and the resultant vector magnitude were calculated from the raw signal. Acceleration was measured in all three axes, where Rp-p is the resultant vector acceleration.
In the first phase of the protocol, each volunteer stood on a custom-made, programmable WBV platform, designed such that both frequency and intensity could be independently controlled by the investigator. Frequency ranges from 30 to 99 Hz, introduced at intensities ranging from 0.05 to 0.6g, were examined (n.b., as these studies required extended subject exposure, higher g-forces could not be evaluated due to restrictions enforced by the University IRB). Drive frequency was first set at 30Hz, and intensity increased from 0.05 g to 0.6 g, as performed in 25 steps. Intensity was then set at 0.2g, and the frequency varied from 30 to 99Hz, as performed in 33 steps of 3Hz. Steps in this phase of the protocol were not randomized, and the sequence of events followed the increases as presented. Transmission was calculated as the ratio of acceleration measured at the cranium or tibia to that measured at the plate surface, and reported as transmissibility:
The second phase of the protocol evaluated the delivered acceleration and transmissibility of three distinct types of WBV devices: uni-directional high magnitude WBV platform, uni-directional low magnitude WBV platform, and a multi-directional high magnitude WBV platform. The first platform (Power Plate, Badhovendorp, Netherlands) provided a fixed-frequency vertical acceleration at two operator settings (‘low’ and ‘high’), both of which were ≫ 3.0g. The second plate (LivMD, Marodyne Inc., Lakeland, FL) delivered a fixed frequency vertical acceleration at a single fixed acceleration (≪1.0g). The third plate (Vibrafit GmbH, Solms, Germany) delivered a horizontal rotational vibration combined with a vertical component, at five acceleration intensities as selected by the user, with each setting also varying the frequency.
Acceleration measurements were collected with volunteers in four different stances: A deep knee bend, with the angle of the knee joint set to 90°, moderate flexion of 135°, legs straight with knees relaxed, and legs straight and knees locked. Data were collected 3x in each position, with the volunteer stepping off the platform between measures. The sequence of platform use was randomized using a computer program.
Acceleration was reported as the mean peak to peak (p-p) intensity averaged over each of the 15 second recordings. For each device, the surface acceleration of the plate and the resultant vector acceleration on the body were also compared. Data are also presented as they relate to ISO-2631 TLV 6.
Results
Six subjects volunteered for the protocol (4m & 2f), with a mean age of 24.1 ± 3.3 years, a mean height of 176.1 ± 9.2 cm, and a mean weight of 74.3 ± 8.5 kg. Accelerations were recorded from each volunteer at both the tibia and cranium, and transmissibility of accelerations from the plate to the tibia and cranium were completed for each protocol with one exception, noted below. Accelerometer readings collected from the tibia and cranium reflected the accelerations of the plate, but were markedly out-of-phase with the peaks (θ = 120° at the tibia, 240° at the head), emphasizing the complexity of the multi-body problem.23
Within the range tested, transmissibility of WBV to the body was independent of vibration intensity (R2 = 0.019, F = 2.38, p > 0.05). In contrast, transmission of acceleration was negatively correlated to frequency, with the greatest magnitude of loss accruing between 40 and 60 Hz. When fit to an exponential curve, a coefficient of determination of −0.845 was calculated (F = 100.91; p < 0.0001). It is important to note that is may be difficult to extrapolate these data to WBV that exceed 1.0g, as uncoupling of the feet and platen is inevitable once earth’s gravitational field is exceeded, and the nature of the multi-body problem becomes even more complex.
In evaluating the intensity and transmissibility of the three commercially available devices, with subjects standing on the device plate surface accelerations of the Power Plate at the low power setting averaged 8.16gp-p ± 0.42 in the vertical, and 1.06gp-p ± 0.25 in the horizontal direction (Table 1). At the high power setting, acceleration of the Power Plate reached 15.09gp-p ± 0.53 in the vertical and 1.51g ± 0.30 in the horizontal direction (Figure 1). The vibration frequency for the Power Plate was 34Hz on both power settings. Displacement at the lower setting was approximately 1.7mm, and at the higher setting displacement reached 3.3mm.
Table 1.
Vibration intensity measured at the surface of three distinct WBV platforms.
| Total (Rp-p) | Vertical (azp-p) | Horizontal (axp-p) | Horizontal (ayp-p) | Frequency | TLVvert | TLVtotal | |
|---|---|---|---|---|---|---|---|
| Power Plate low setting | 8.29 ±0.42 | 8.16 ±0.29 | 1.06 ±0.25 | 1.05 ±0.32 | 34 Hz | ≪ 1 Min | ≪ 1 Min |
| Power Plate high setting | 15.25 ±0.77 | 15.09 ±0.53 | 1.20 ±0.67 | 0.77 ±0.59| | 34 Hz | ≪ 1 Min | ≪ 1 Min |
| Marodyne LivMD | 0.34 ±0.05 | 0.31 ±0.05 | 0.03 ±0.008 | 0.03 ±0.008 | 33 Hz | <8 Hrs | <8 Hrs |
| Vibrafit setting 1 | 2.97 ±1.01 | 0.50 ±0.27| | 2.34 ±0.95 | 1.75 ±0.64 | 23 Hz | <2.5 Hrs | ≪ 1 Min |
| Vibrafit setting 2 | 4.08 ±1.62 | 0.97 ±0.57 | 3.28 ±1.55 | 2.22 ±0.93 | 28 Hz | <1 Hr | ≪ 1 Min |
| Vibrafit setting 3 | 5.01 ±1.90 | 1.64 ±1.08 | 3.45 ±1.70 | 3.24 ±1.08 | 33 Hz | <25 Min | ≪ 1 Min |
| Vibrafit setting 4 | 6.32 ±2.25 | 1.74 ±1.25 | 5.13 ±2.28 | 3.26 ±1.25 | 39 Hz | <25 Min | ≪ 1 Min |
| Vibrafit setting 5 | 7.75 ±2.44 | 2.17 ±1.57 | 6.57 ±2.39 | 3.50 ±1.57 | 43 Hz | <25 Min | ≪ 1 Min |
Total and direction specific acceleration, ± S.D., measured from the surface of three vibration platforms. Acceleration intensity reported in g’s, where 1g = earth’s gravitational field. Acceleration of both Power Plate and Marodyne devices is delivered predominantly in the vertical direction, while the Vibrafit device was comprised of both vertical and transverse accelerations, with acceleration intensity increasing with frequency. The TLV duration is the length of exposure considered generally safe by ISO standards, with the second to last column representing the vertical acceleration TLV limit, and the last column providing the total intensity TLV. Importantly, TLV does not consider transmissibility to the body, but only that to which the body is exposed. While ISO-2631-1 considers the inherent risks of acceleration only in the vertical direction, other ISO TLV standards emphasize the potential dangers of vibration in the horizontal axes.
Figure 1.
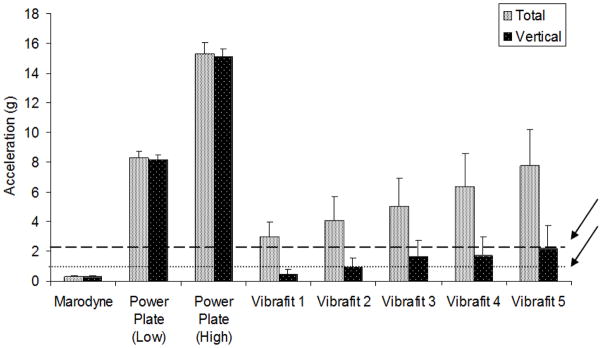
Resultant (gray) and vertical (black) acceleration of the top surface of the three vibration platforms at a range of settings. The amplitude of the vibrations is also shown relative to the ISO-2631 limit for human tolerance for 30 Hz WBV at both 1 minute (dotted line) and 4 hours of daily exposure (dashed line). The Threshold limit value (TLV) is the total daily exposure considered “generally safe” by the National Institute for Occupational Safety and Health (NIOSH), as prescribed by ISO-2631-1, which focuses only on the inherent risks of vibration in the vertical direction. Other ISO guidelines which focus on exposure limits for vibration emphasize the potential risks of vibration in other axes, with particular attention to the vector sum of vibration in three axes.
The Marodyne Medical LivMD device generated a sinusoidal vertical acceleration through a linear actuator. Surface accelerations of the Marodyne Medical plate averaged 0.31gp-p ± 0.05 in the vertical direction and 0.03gp-p ± 0.01 in the horizontal (Figure 1). Acceleration frequency was 33Hz. Displacement of the top platen was less than 100 microns.
The Vibrafit device generated a vibration through the use of an unbalanced mass motor attached to the top platen with a vertical axis of rotation, generating a horizontal acceleration. Vertical acceleration of the Vibrafit device ranged from 2.9g at 23Hz, to 7.9g at 48Hz (Figure 1). Vertical displacement at the lowest setting was approximately 1.4mm, while at the higher g-force displacement in the vertical direction fell to 0.85mm.
While on the low-setting of the Power Plate, acceleration of the subject with knees bent at 90° produced average acceleration at the tibia of 5.48gp-p ± 0.97, and at the cranium of 0.78gp-p ± 0.38. In a shallow squat, tibia acceleration was 3.58gp-p ± 1.56 and the cranium 0.40gp-p ± 0.25. At the high setting, accelerations in a deep bend measured 10.54 gp-p ± 2.10 and 1.20gp-p ± 0.67 at the tibia and cranium, respectively. While holding a shallow knee bend, the signals averaged 7.32gp-p ± 2.15 and 0.77gp-p ± 0.59, for the tibia and cranium, respectively. The test was briefly attempted with straight legs, but caused immediate discomfort in several volunteers and was abandoned.
On the Marodyne device, with knees at 90°, accelerations at the tibia reached 0.28gp-p ± 0.11, and at the cranium reached 0.05gp-p ± 0.01. With knees at 135°, accelerations at the tibia were 0.29gp-p ± 0.07, while the cranium reached 0.07gp-p ± 0.04. With knees straight but relaxed, acceleration at the tibia exceeded the intensity delivered by the plate, such that it reached 0.36gp-p ± 0.09 at the tibia, and 0.29gp-p ± 0.17 at cranium. With knees locked, acceleration at the tibia reached 0.42gp-p ± 0.10, and the cranium 0.37gp-p ± 0.23.
On the Vibrafit, accelerations at the tibia varied from 0.88gp-p to 2.16gp-p, while the cranium varied from 0.14gp-p to 0.37gp-p with increasing accelerations of the platform. As with the other devices, transmissibility was attenuated with flexion of the knees.
Transmissibility on the Power Plate averaged 69.9 ± 14.1% and 50.6 ± 14.5% at the tibia in deep and shallow bend stances respectively; with 8.1 ± 4.5% and 5.5 ± 4.4% transmissibility to the cranium (straight leg stance was not attempted). Transmissibility of the Marodyne device increased with straightness of stance: minimal transmission was observed with knees in a deep bend (63.0 ± 28.4% and 10.3 ± 2.0% at the tibia and cranium), while maximal transmission occurred with knees locked (90.2 ± 24.4% and 78.9 ± 43.4% at the tibia and cranium). Standing on the Vibrafit, transmission at the tibia ranged from 28 to 50%, falling at the cranium to 2 to 11%.
Discussion
Daily exposure to whole body vibration has fostered a range of injuries and impairments. Chronic exposure to low- and mid-frequency whole body vibration, such as that which truck drivers and heavy machinery operators’ typically experience, is a recognized etiologic factor in low back pain, arm numbness, and visual impairment.1, 24 Further, as demonstrated in workers in the agricultural, forestry, food and construction industries, high frequency, high intensity vibration of arms and hands by portable machinery can lead to permanent vascular damage and nerve dysfunction.25, 26 Despite the recognized risks of vibration exposure, a large number of WBV devices are available to the consumer, with little if any attention given to the potential inherent risks of voluntary exposure to the mechanical signals that these devices deliver.
The three WBV platforms analyzed in this study were chosen to represent three distinct varieties of WBV devices; high intensity vertical vibration (Power Plate), low intensity vertical vibration (Marodyne LivMD), and three-degree of freedom high intensity vibration (Vibrafit). To assess the risk to users, the vibration intensities of these devices were compared to the daily Threshold Limit Values (TLVs), as determined by the International Standards Organization (ISO), and accepted by NIOSH and OSHA, reflecting what these agencies consider as the maximum daily occupational exposure that could be considered safe. Two of the three platforms tested, Power Plate and Vibrafit, far exceeded the TLVs established by ISO ISO- 2631, with delivered vibrations not considered safe for even seconds, much less minutes, of daily exposure (Figure 2). If the ISO-TLV are to be considered relevant to voluntary use of home-, hospital or gym-based devices, it must be concluded that even brief exposure to such WBV levels may be extremely dangerous, particularly in the aged, adolescent, or infirm, and to a range of physiologic systems.19, 20
Figure 2.

A direct representation of ISO-2631 guidelines for human exposure limits to whole body vibration, defining areas of high risk (red: < 1 minute of exposure), caution (yellow: between 1 hour and 1 minute of exposure), and a region of safety (green: > 1 hour of exposure), which change as a function of frequency (x-axis) and acceleration intensity (y-axis). The solid lines, each in the shape of a hockey stick, represent the daily exposure limits across the 1 to 50 Hz range. The peak g-force measured from the top surface of the Marodyne (A; single setting), Vibrafit vertical vibration (B; five settings; open circles), Vibrafit resultant (C; five settings; solid circles), and Power Plate (D; low setting as open circle; and high setting as solid circle) devices are shown. Points which lie in the ‘green zone’ are considered safe for exposures up to one hour each day, points which fall in the ‘yellow zone’ have duration limits of between one minute and one hour of exposure each day, while points marked in the ‘red zone’ are not considered safe for even one minute exposure each day. This graph considers only the inherent risks of vibration in the vertical direction, as prescribed by ISO-2631-1. This is not meant to imply that vibration in the horizontal axes, or that a vector sum of vibration from the three axes, should be ignored.
Plate acceleration of the Power Plate, even at the lowest settings, show acceleration measurements well in excess of even the briefest band evaluated in the ISO threshold TLV limits. According to ISO 2631-1, daily exposure of a 31Hz WBV should not exceed even 1 minute when accelerations are greater than 5.6 m•s−2 rms (root mean square) in the vertical direction. However, surface measurements show that accelerations of the Power Plate averaged 28.7 m•s−2 (8.3g) on the low power setting, while on the high power setting the surface vibration reached 52.9 m•s−2 (15.3g). For an individual using the device for 10 minutes, the magnitude of vertical vibration would be 3.6x the maximum allowed level on the low power setting, and 6.6x the maximum allowed level on the high power setting. The Marodyne LivMD device remained well below the TLV with a surface acceleration of 1.07 ± 0.05 m•s−2, with such exposure considered safe for between 4 to 8 hours daily. The Vibrafit device exceeded TLV values by 1.7 to 2.4x, depending on the power setting, for the 10 minute recommended usage, when total 3-dimensional vibration intensity was taken into account. It is important to point out that ISO-2631-1, pointing directly to vibrations in the workplace, consider only the vertical component of the vibration. Other ISO guidelines for vibration (e.g., 2631-2,3 &4), all consider the vector sum of the vibration in three directions in the threshold advisories, and may someday be considered relevant with regard to devices that deliver WBV.
Tri-axial accelerometers allow for measure of vibration in any direction, and can account fully for the transmission of ground-based vibration to selected regions of the appendicular, axial and cranial skeleton, taking into account extenuating factors such as posture. Knowing that transmission of vibration can be assessed through non-invasive surface measurement, experiments to assess the magnitude of acceleration transmission generated by vibration platforms can be performed.22 While not as accurate as direct bone measurement, skin surface mounted accelerometers allow for greater freedom of measure, simplified (and safer) volunteer recruitment and for multiple repeat measures over time. Previous studies have indicated that relatively small (<10%) overestimation of accelerations on the skeleton may be incurred through the use of skin mounted accelerometers as compared to those measured from pins inserted into the bone.27, 28
In all measures, there was a phase delay between the waveform measured at the platform and the acceleration measured on the body. This is indicative of the multiple mass-spring-dampener units that make up the musculoskeletal system of the human body,23 which act to absorb and pad vital organs from dangerous impact accelerations which occur during locomotion,29, 30 or contribute to the resonance of the system such that the tibia or cranium can exceed the amount of acceleration delivered at the foot.30 It is also important to recognize the loss of energy that is evident as transmissibility falls from the top of the platform to the top of the axial skeleton. The cause of the 75 to 90% of the energy of the mechanical vibration being lost at the bite-bar when the knees are bent is unknown, but perhaps is lost as energy absorbed in the joint space and dissipated in articular cartilage.31
Even recognizing vibration exposure as deleterious to circulatory, respiratory, neurologic and musculoskeletal systems, relatively little is known about the consequences of chronic WBV exposure on brain health.32 Accelerations at the head with volunteers on the Power Plate were recorded up to 1.85g, with participants in a bent-knee stance, which minimizes transmission to the cranium. Although a straight-legged stance was abandoned in this study due to safety concerns, a user who closely followed the documented exercises included with this device, which included upright stance as well as arm exercises directly resisting the top platen, may experience accelerations to the head equaling (or exceeding) the g-force delivered at the foot. With some similarities in the clinical expression, epidemiology and pathogenesis of chronic traumatic encephalopathy (CTE) and Alzheimer’s disease, as well as their representation by neurofibrillary tangle formation, it has been postulated that sub-concussive insults to the brain may predispose an individual to susceptibility to neurodegenerative diseases most often evident in the elderly.3 The implications on brain health with chronic exposure of such accelerations is unknown, and research is needed to show that traumatic brain injury would not be fostered by use of such high-intensity WBV devices. At the very least, supervised use of high-g devices by trained therapists should be employed, and straight-legged stance studiously avoided.
Conclusions
Threshold Limits for Vibration (TLV) provided by ISO-2631 were established to minimize occupational health risk from exposure to vibration in the workplace.6, 30 The vibration intensity levels are defined by ISO as the acceleration of the floor under the foot of a standing subject, which in the case of the WBV platforms correlates to the acceleration generated by the platform itself. While TLVs were established to provide guidelines of what should be generally considered safe for daily exposure in a work environment, such advisories may not be entirely applicable to the accelerations of exercise or medical devices. It could be presumed that the acute or chronic exercise or medical benefits realized by the use of WBV devices may offset the risks generated by exposure, and because the TLVs are only approximates of risk, actual physiological damage may occur significantly above or below the presented values. Regardless, considering that the vibration intensities far exceed the ISO guidelines, even if mandated for occupational exposure, it must be concluded that some WBV devices may present significant risk to users, and those users should be fully informed of the ultimate risk to a range of physiologic systems.
Practical Implications.
The use of Whole Body Vibration is escalating as an adjuvant or surrogate for exercise, and is being considered as an intervention to augment or accelerate rehabilitation.
Vibration is a known to cause both acute and chronic injury to a range of physiologic systems, including musculoskeletal, circulatory and nervous.
Several Whole Body Vibration devices far exceed what is considered safe for even brief exposure to the healthy standing human.
Caution must be employed when considering the use of Whole Body Vibration, particularly in the case of the elderly or infirm.
It is recommended that only those WBV devices which conform to ISO-2631 guidelines and exposure limits are utilized.
Acknowledgments
This work supported by the National Institutes of Health through NIAMS grant #AR043498 and NIA grant #AG025489. The authors are also very grateful to the volunteers that volunteered for this study.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Bovenzi M. Low back pain disorders and exposure to whole-body vibration in the workplace. Semin Perinatol. 1996;20(1):38–53. doi: 10.1016/s0146-0005(96)80056-5. [DOI] [PubMed] [Google Scholar]
- 2.Curry BD, Bain JL, Yan JG, et al. Vibration injury damages arterial endothelial cells. Muscle Nerve. 2002;25(4):527–34. doi: 10.1002/mus.10058. [DOI] [PubMed] [Google Scholar]
- 3.Costanza A, Weber K, Gandy S, et al. Review: Contact sport-related chronic traumatic encephalopathy in the elderly: clinical expression and structural substrates. Neuropathology and applied neurobiology. 2011;37(6):570–84. doi: 10.1111/j.1365-2990.2011.01186.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Seidel H, Heide R. Long-term effects of whole-body vibration: a critical survey of the literature. Int Arch Occup Environ Health. 1986;58(1):1–26. doi: 10.1007/BF00378536. [DOI] [PubMed] [Google Scholar]
- 5.Boshuizen HC, Bongers PM, Hulshof CT. Self-reported back pain in fork-lift truck and freight-container tractor drivers exposed to whole-body vibration. Spine (Phila Pa 1976) 1992;17(1):59–65. doi: 10.1097/00007632-199201000-00010. [DOI] [PubMed] [Google Scholar]
- 6.Evaluation of Human Exposure to Whole Body Vibration. Geneva: International Standards Organization; 1997. Available from: International Standards Organization. Specific to ISO-2631. [Google Scholar]
- 7.Delecluse C, Roelants M, Diels R, et al. Effects of whole body vibration training on muscle strength and sprint performance in sprint-trained athletes. Int J Sports Med. 2005;26(8):662–8. doi: 10.1055/s-2004-830381. [DOI] [PubMed] [Google Scholar]
- 8.Rittweger J, Just K, Kautzsch K, et al. Treatment of chronic lower back pain with lumbar extension and whole-body vibration exercise: a randomized controlled trial. Spine. 2002;27(17):1829–34. doi: 10.1097/00007632-200209010-00003. [DOI] [PubMed] [Google Scholar]
- 9.Thompson WR, Rubin CT, Rubin J. Mechanical regulation of signaling pathways in bone. Gene. 2012;503(2):179–93. doi: 10.1016/j.gene.2012.04.076. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Reyes ML, Hernandez M, Holmgren LJ, et al. High-Frequency, Low-Intensity Vibrations Increase Bone Mass and Muscle Strength in Upper Limbs, Improving Autonomy in Disabled Children. Journal of Bone and Mineral Research. 2011;26(8):1759–66. doi: 10.1002/jbmr.402. [DOI] [PubMed] [Google Scholar]
- 11.Judex S, Zhong N, Squire ME, et al. Mechanical modulation of molecular signals which regulate anabolic and catabolic activity in bone tissue. J Cell Biochem. 2005;94(5):982–94. doi: 10.1002/jcb.20363. [DOI] [PubMed] [Google Scholar]
- 12.Rubin C, Turner AS, Bain S, et al. Anabolism: Low mechanical signals strengthen long bones. Nature. 2001;412(6847):603–4. doi: 10.1038/35088122. [DOI] [PubMed] [Google Scholar]
- 13.Gilsanz V, Wren TA, Sanchez M, et al. Low-Level, High-Frequency Mechanical Signals Enhance Musculoskeletal Development of Young Women With Low BMD. J Bone Miner Res. 2006;21(9):1464– 74. doi: 10.1359/jbmr.060612. [DOI] [PubMed] [Google Scholar]
- 14.Ward K, Alsop C, Caulton J, et al. Low magnitude mechanical loading is osteogenic in children with disabling conditions. J Bone Miner Res. 2004;19(3):360–9. doi: 10.1359/JBMR.040129. [DOI] [PubMed] [Google Scholar]
- 15.Lam TP, Ng BK, Cheung LW, et al. Effect of whole body vibration (WBV) therapy on bone density and bone quality in osteopenic girls with adolescent idiopathic scoliosis: a randomized, controlled trial. Osteoporosis International. 2012 doi: 10.1007/s00198-012-2144-1. epub ahead of print. [DOI] [PubMed] [Google Scholar]
- 16.Muir J, Judex S, Qin YX, et al. Postural instability caused by extended bed rest is alleviated by brief daily exposure to low magnitude mechanical signals. Gait Posture. 2011;33(3):429–35. doi: 10.1016/j.gaitpost.2010.12.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Verschueren SM, Roelants M, Delecluse C, et al. Effect of 6-month whole body vibration training on hip density, muscle strength, and postural control in postmenopausal women: a randomized controlled pilot study. J Bone Miner Res. 2004;19(3):352–9. doi: 10.1359/JBMR.0301245. [DOI] [PubMed] [Google Scholar]
- 18.Abercromby AF, Amonette WE, Layne CS, et al. Vibration exposure and biodynamic responses during whole-body vibration training. Med Sci Sports Exerc. 2007;39(10):1794–800. doi: 10.1249/mss.0b013e3181238a0f. [DOI] [PubMed] [Google Scholar]
- 19.Pel JJ, Bagheri J, van Dam LM, et al. Platform accelerations of three different whole-body vibration devices and the transmission of vibrations to the lower limbs. Med Eng Phys. 2009;31(8):937–44. doi: 10.1016/j.medengphy.2009.05.005. [DOI] [PubMed] [Google Scholar]
- 20.Kiiski J, Heinonen A, Jarvinen TL, et al. Transmission of vertical whole body vibration to the human body. J Bone Miner Res. 2008;23(8):1318–25. doi: 10.1359/jbmr.080315. [DOI] [PubMed] [Google Scholar]
- 21.Rubin C, Pope M, Chris FJ, et al. Transmissibility of 15-hertz to 35-hertz vibrations to the human hip and lumbar spine: determining the physiologic feasibility of delivering low-level anabolic mechanical stimuli to skeletal regions at greatest risk of fracture because of osteoporosis. Spine. 2003;28(23):2621–7. doi: 10.1097/01.BRS.0000102682.61791.C9. [DOI] [PubMed] [Google Scholar]
- 22.Pope MH, Magnusson M, Wilder DG. Kappa Delta Award. Low back pain and whole body vibration. Clin Orthop. 1998;(354):241–8. doi: 10.1097/00003086-199809000-00029. [DOI] [PubMed] [Google Scholar]
- 23.Fritton JC, Rubin CT, Qin YX, et al. Whole-body vibration in the skeleton: development of a resonance- based testing device. Ann Biomed Eng. 1997;25(5):831–9. doi: 10.1007/BF02684167. [DOI] [PubMed] [Google Scholar]
- 24.Gerr F, Mani L. Work-related low back pain. Prim Care. 2000;27(4):865–76. doi: 10.1016/s0095-4543(05)70181-0. [DOI] [PubMed] [Google Scholar]
- 25.Sutinen P, Toppila E, Starck J, et al. Hand-arm vibration syndrome with use of anti-vibration chain saws: 19-year follow-up study of forestry workers. Int Arch Occup Environ Health. 2006;79(8):665–71. doi: 10.1007/s00420-006-0099-2. [DOI] [PubMed] [Google Scholar]
- 26.Harkonen H, Riihimaki H, Tola S, et al. Symptoms of vibration syndrome and radiographic findings in the wrists of lumberjacks. Br J Ind Med. 1984;41(1):133–6. doi: 10.1136/oem.41.1.133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kim W, Voloshin AS, Johnson SH, et al. Measurement of the impulsive bone motion by skin-mounted accelerometers. J Biomech Eng. 1993;115(1):47–52. doi: 10.1115/1.2895470. [DOI] [PubMed] [Google Scholar]
- 28.Nokes L, Fairclough JA, Mintowt-Czyz WJ, et al. Vibration analysis of human tibia: the effect of soft tissue on the output from skin-mounted accelerometers. J Biomed Eng. 1984;6(3):223–6. doi: 10.1016/0141-5425(84)90107-9. [DOI] [PubMed] [Google Scholar]
- 29.McNitt-Gray JL. Kinetics of the lower extremities during drop landings from three heights. Journal of Biomechanics. 1993;26(9):1037–46. doi: 10.1016/s0021-9290(05)80003-x. [DOI] [PubMed] [Google Scholar]
- 30.Griffin JJ. Handbook of human vibration. London: Academic Press; 2001. [Google Scholar]
- 31.Beckett J, Jin W, Schultz M, et al. Excessive running induces cartilage degeneration in knee joints and alters gait of rats. Journal of orthopaedic research: official publication of the Orthopaedic Research Society. 2012;30(10):1604–10. doi: 10.1002/jor.22124. [DOI] [PubMed] [Google Scholar]
- 32.Stern RA, Riley DO, Daneshvar DH, et al. Long-term consequences of repetitive brain trauma: chronic traumatic encephalopathy. PM & R: the journal of injury, function, and rehabilitation. 2011;3(10):S460–7. doi: 10.1016/j.pmrj.2011.08.008. [DOI] [PubMed] [Google Scholar]