

Dear Editor,
A 61-year-old female with the past medical history of hypertension and osteoarthritis presented to Emergency Department with sudden onset of shortness of breath and non-productive cough 30 min, after taking white willow bark supplement. The patient denied any history of the drug or supplement allergy. Pulse oximetry demonstrated oxygen desaturation; SpO2 of 75% on ambient air and 94% on nasal cannula with the flow of oxygen 20 L/min. Arterial blood gas although on FiO2 of 100% showed severe hypoxemia with the high A-a gradient, metabolic acidosis with respiratory compensation (pH 7.28, PCO2 36 mmHg, PaO2 75 mmHg, and HCO3 19 mmol/L). Blood tests demonstrated evidence of wide anion gap (AG) metabolic acidosis (AG 14 mmol/L) from lactic acidosis (lactic acid 4.9 mmol/L) with the normal gap metabolic acidosis (∆AG/∆Bicarb = 0.4) and the patient had no osmolal gap. Furthermore, serum ketone and salicylate levels were undetectable and her chest X-ray showed bilateral interstitial infiltrates [Figure 1]. Transthoracic echocardiogram revealed normal systolic and diastolic function. The diagnosis of acute hypoxic respiratory failure secondary to severe acute respiratory distress syndrome (ARDS) from reaction to white willow bark was made; the PaO2/FiO2 of 75 mmHg. The patient was promptly started on intravenous venous methylprednisolone and oral antihistamines including diphenhydramine and ranitidine. The patient responded well with our treatment and her oxygen requirement gradually improved from 94% on FiO2 of 100% to 95% on room air. Lactic acidosis also subsided after maintaining adequate oxygenation.
Figure 1.
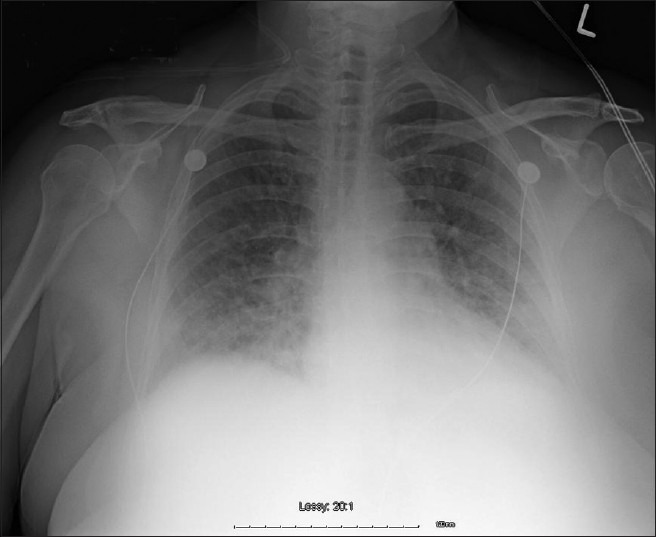
Chest X-ray demonstrated bilateral interstitial infiltrates
The use of white willow bark supplement was first reported back to the time of Hippocrates (400 BC) when patients were advised to chew on the bark for pain relief and fever reduction. Willow bark is also included in weight-loss products.[1] There have been a remarkably small number of reported cases of adverse reactions to willow bark extract. These adverse drug reactions are usually mild (maculopapular rashes). White willow bark induced anaphylaxis is rare; however, a few cases have been reported.[2,3] To our knowledge, this is the first report of white willow bark induced ARDS. People who are allergic or sensitive to salicylates (such as aspirin) should not use willow bark.
References
- 1.Astrup A, Toubro S, Cannon S, Hein P, Madsen J. Thermogenic synergism between ephedrine and caffeine in healthy volunteers: A double-blind, placebo-controlled study. Metabolism. 1991;40:323–9. doi: 10.1016/0026-0495(91)90117-f. [DOI] [PubMed] [Google Scholar]
- 2.Chivato T, Juan F, Montoro A, Laguna R. Anaphylaxis induced by ingestion of a pollen compound. J Investig Allergol Clin Immunol. 1996;6:208–9. [PubMed] [Google Scholar]
- 3.Boullata JI, McDonnell PJ, Oliva CD. Anaphylactic reaction to a dietary supplement containing willow bark. Ann Pharmacother. 2003;37:832–5. doi: 10.1345/aph.1D027. [DOI] [PubMed] [Google Scholar]