

Abstract
Purpose
This study was performed to investigate the clinical usefulness of teleradiology in general dental practice.
Materials and Methods
Two hundred and seventy five cases were submitted for inquiry to the case presentation board of the website of The Korean Academy of Oral and Maxillofacial Radiology for a 5 year periods. The diagnosis results of those cases were analyzed according to the disease classification, the correlation with the patient's chief complaint, the necessity of additional examinations or treatments, the image modalities, and the number of dentists inquiring.
Results
Differential diagnoses of normal anatomic structures were the most frequently submitted cases, covering 15.6% of all cases. Among 275 cases, 164 cases required no additional treatments or examinations. Panoramic radiographs were the most frequently submitted images, accounting for 248 inquiries. The 275 cases were submitted by 96 dentists. Fifty-two dentists wrote one inquiry, and 44 inquired 2 or more times. The average inquiry number of the latter group was 5.0 cases.
Conclusion
A teleradiology system in general dental practice could be helpful in the differential diagnosis of common lesions and reduce unnecessary costs.
Keywords: Teleradiology; General Practice, Dental
Introduction
According to the American College of Radiology (ACR) standard for teleradiology, teleradiology is the electronic transmission of radiologic images from one location to another for the purposes of interpretation and/or consultation. The concept of teleradiology has a long history with the first record of transmission of dental radiographs in 1929.1 However, teleradiology systems began to be actively utilized only after the introduction of digital images, the development of telecommunication technology, and the emergence of the internet. Nowadays, images can be easily sent not only to another part of the hospital but also to other locations around the world.
A teleradiology system can provide timely diagnosis and patient care, especially for nighttime coverage of the emergency room or for small community hospitals with insufficient staffing. Therefore, teleradiology systems have been widely used in the medical field and even studies of remote interpretation via a mobile hand held device have been reported.2-4 However, little research has addressed the application of teleradiology to dentistry, and most such studies are limited to investigation of specific diseases such as maxillofacial pathoses requiring surgery or temporomandibular joint (TMJ) disorder.5-8 Furthermore, no study has been conducted to evaluate the usefulness of teleradiology in general dental practice.
Panoramic and periapical radiography are the most frequently used image modalities in general dental practice. Panoramic radiography has been widely used for decades because of its convenience, low dose and good diagnostic performance.9 In fact, the American Dental Association has recommended the use of panoramic radiography with selected periapical radiographs for examination of new patients with permanent dentition.10
Accordingly, the purpose of this study was to investigate the clinical usefulness of teleradiology and determine the image modality that has been most submitted for inquiry from general dental practices by analyzing the cases of usage of a teleradiology service that has been run by the Korean Academy of Oral and Maxillofacial Radiology (KAOMFR) for five years.
Materials and Methods
The Korean Academy of Oral and Maxillofacial Radiology has been running the case presentation board on its website as a pilot service for teleradiology since 2007. Dentists who have subscribed to the website of the KAOMFR can submit inquiries including a number of images and clinical information to this board free of charge, and receive replies from the professors of the departments of oral and maxillofacial radiology affiliated with KAOMFR. It is suggested that the written posts include the chief complaint, signs and symptoms.
A total of 275 cases were submitted for inquiry from May 2007 to June 2012. The results of the case interpretation were retrospectively analyzed in this study. All diagnosis results made by oral and maxillofacial radiology professors were reviewed and recorded by one professor. In cases in which a final diagnosis could not be made due to insufficient images, clinical information, biopsy results, the tentative diagnosis results were recorded.
Even though many kinds of lesions were found in the transmitted images, only the lesions about which the inquiries were submitted were included in this study. Since this study was not aimed to evaluate the diagnostic performance of radiologists, but to determine the diseases that require a differential diagnosis by radiologists in general dental practice.
The collected data were analyzed according to the disease classification, the correlation with the patient's chief complaint (CC), the necessity of additional examinations or treatments, the modalities of images, and the number of dentists submitted inquiries.
The disease classification used the following categories: normal anatomic structures, inflammatory lesions, idiopathic osteoscleroses, fibro-osseous lesions, cysts, tooth-related lesions, maxillary sinus lesions, static bone cavities, simple bone cysts, soft tissue calcifications, benign tumors, temporomandibular joint disorders, implant-related lesions, malignant tumors, and other.
Among the normal anatomic structures, soft tissue shadows, margin of hard tissue, cancellous bone pattern, and absence of pathologic changes were included. Among the inflammatory lesions, periapical lesions, osteomyelitis, and osteitis were included. Dental caries, periodontitis, and supernumerary tooth were classified into tooth-related lesions. Inquiries about quality control, foreign bodies, and image artifacts were classified as other category.
Results
A total of 275 cases were classified into the following diagnosis results: 43 cases of normal anatomic structure, 39 cases of inflammatory lesion, 38 cases of idiopathic osteosclerosis, 33 cases of fibro-osseous lesion, 29 cases of cyst, 23 cases of tooth-related lesion, 14 cases of maxillary sinus lesion, and 8 other lesions, each type of which was less than 5% of all cases (Table 1).
Table 1.
Disease classifications of the cases submitted to the website for inquiry
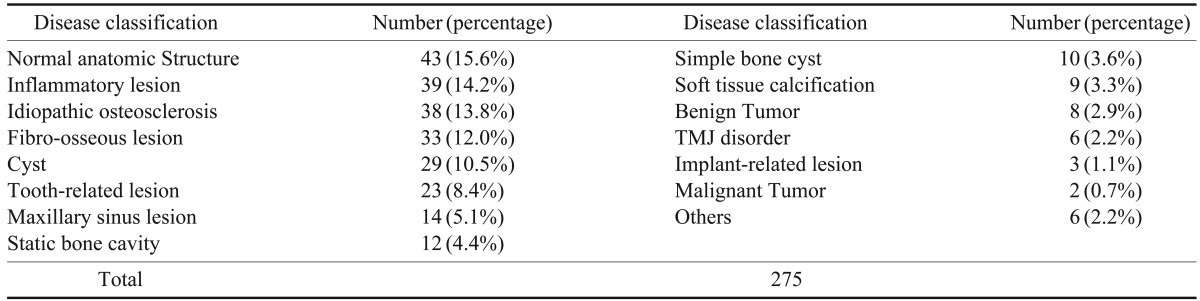
Differential diagnoses of normal anatomic structures were most frequently submitted, covering 15.6% of all cases. The second most common type of case was inflammatory lesions, comprising 21 cases of periapical rarefying osteitis, 5 cases of periapical abscess, 4 cases of osteomyelitis, 4 cases of condensing osteitis and others (Table 2). The fibro-osseous lesions included 17 cases of periapical cemental dysplasia, 8 cases of focal-osseous dysplasia, 5 cases of florid-osseous dysplasia, and 3 cases of fibrous dysplasia. The tooth-related lesions included 9 cases of periodontitis, 7 cases of supernumerary tooth, 3 cases of dental caries, 2 cases of tooth fracture, 1 case of a missing tooth, and 1 case of root resorption.
Table 2.
Disease classification of inflammatory lesions

In the correlation between the classification of cases and the patients' chief complaints, 174 cases had been submitted with a patient's chief complaint, and 101 cases were not. Among the 174 cases associated with a patient's chief complaint, 89 cases required additional treatments or examinations (Fig. 1). They consisted of 34 cases of inflammatory lesion, 21 cases of cyst, 20 cases of tooth-related lesion, and other cases, each type of which accounted for less than 5% of the cases (Table 3). Meanwhile, the remaining 85 cases required no additional treatments or examinations. The distribution by disease classification is summarized in Table 4. Among the 101 cases that were not associated with the patient's chief complaints, 22 cases required additional treatments or examinations (Table 5).
Fig. 1.
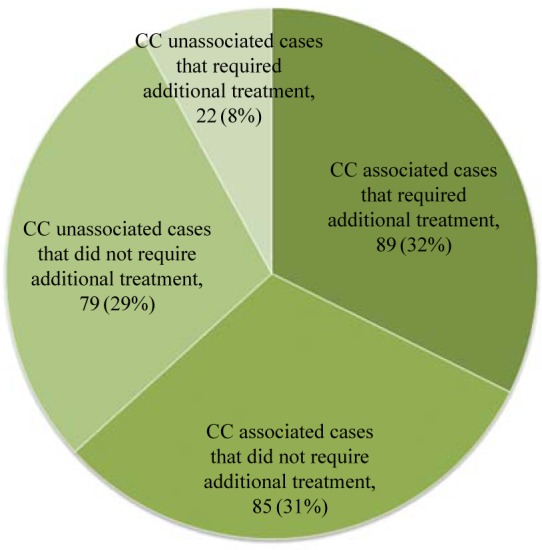
Classification according to the association with the chief complaint (CC) of patients and the requirement for additional treatment.
Table 3.
Disease classification of lesions that were associated with the chief complaint and required additional treatment

Table 4.
Disease classification of lesions that were associated with the chief complaint and did not require additional treatment

Table 5.
Disease classification of lesions that were not associated with the chief complaint and required additional treatment

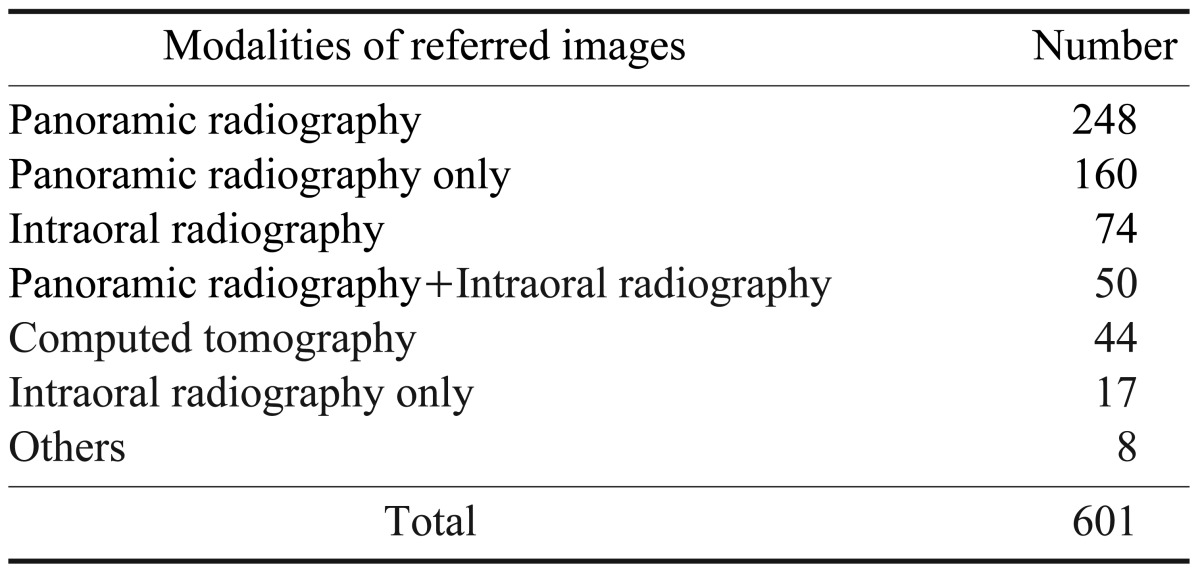
The type and number of images used in inquiry was analyzed by the image modalities. The image modalities were counted redundantly. The most frequently submitted image was panoramic radiographs, which accounted for 248 cases. Among those 248 cases, 160 cases contained only panoramic radiographs. The second most submitted image was intraoral radiographs, which accounted for 74 cases. Seventeen cases out of these 74 cases contained intraoral radiographs only. Both panoramic and intraoral radiographs were included in 50 cases, and computed tomographic images were included in 44 cases. Other images such as Waters' view, temporomandibular joint panoramic image, and cephalometric image, were included in 8 cases (Table 6).
Table 6.
Modality and number of images (redundantly counted)
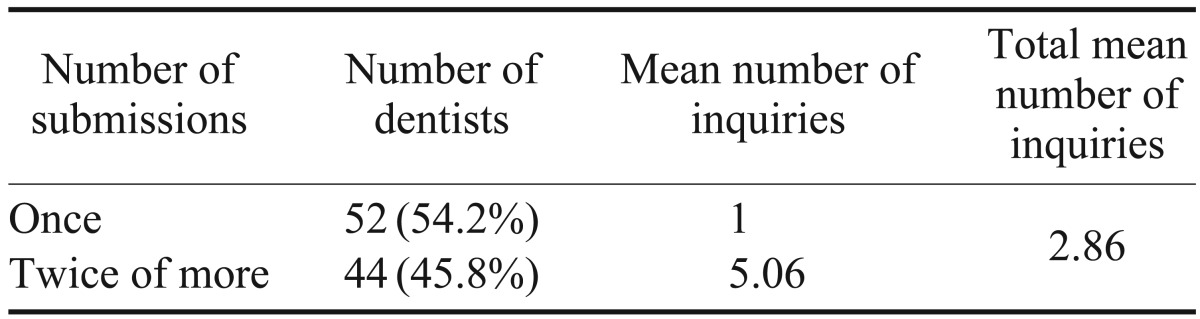
The 275 cases were submitted by 96 dentists. A given dentist submitted about 2.9 cases on average. Among these 96 dentists, 52 wrote one inquiry, and 44 inquired two or more times. The average inquiry number of the latter group was 5.0 cases (Table 7).
Table 7.
Number of submitting dentists
Discussion
This study aimed to investigate the disease classification referred via the teleradiology system, and the usefulness of the system in general dental practice. Previous studies about teleradiology in dental practice have focused mainly on specific diseases such as maxillofacial pathoses that require surgery, TMJ disorder.5-8 However, this study proved that differential diagnosis of common diseases such as normal anatomic structure, inflammatory lesion, and idiopathic osteosclerosis, was also in demand. On the other hand, there was no case classified as trauma to the jaw bone since patients with bony fractures might not be treated by general practitioners.
The use of a teleradiology system is efficient from an economic perspective. Salazar-Fernandez reported that telemedicine shortens the delay in treatment after diagnosis and reduces lost working hours in the treatment of patients with TMJ disorder.6 It was also reported that the unnecessary transfer of patients was decreased by 50% when a teleradiology system was used.5 In this study, no additional treatment was required in 165 of the 275 cases, which meant that unnecessary costs could be reduced by up to 60%. This proportion was further increased up to 78.2% in the chief complaint-unassociated group, which were found by chance. On the other hand, the remaining 21.8% of the chief complaint-unassociated group required additional examinations or treatments, and this rate could not be regarded as negligible.
Forty four dentists referred to the pilot service for teleradiology more than two times among the 96 dentists and the system showed a 45.6% reuse rate. The 44 dentists inquired about five cases on average and could be regarded as being satisfied with the teleradiology system. Salazar-Fernandez reported that more than 99% of patients were also satisfied with a teleradiology system.6 These results show the efficiency of teleradiology systems for general dental practice.
As expected, the most frequently submitted images were panoramic radiographs; 90% of cases included a panoramic image. The second most referred images were intraoral radiographs, which accounted for 74 cases (27%). Computed tomographic images including cone-beam computed tomograms were included in 44 cases. Other images were composed of 6 cases of temporomandibular joint panoramic image, 1 case of cephalometric image, and 1 case of Waters' radiograph. Therefore, a panoramic image with selected periapical radiographs might be most useful in teleradiology for general dental practice.
Since the teleradiology system was introduced, the main concern has been its diagnostic accuracy. In 2002, Jacobs et al reported that telemedical diagnosis of condylar fractures was similarly accurate compared to direct visualization; however, transmitted plain films of midfacial fractures showed mediocre quality and the accuracy of diagnosis was lower than with direct visualization.11 On the other hand, other previous studies have revealed no significant differences between the assessment of periapical lesions using traditional radiographs and transmitted radiographs by clinicians.12,13
Torres-Pereira also reported that distant diagnosis could be an effective approach for oral lesions,14 while Rollert et al reported that telemedicine consultations were as reliable as those conducted by traditional methods.7 Agrawal et al. found 227 discrepancies in 126,449 cases of international teleradiology services. Of these errors, the majority (167/227) were levels 2 and 3 (minor error and error of long-term significance but not in the acute setting). The error rate was less than 0.2% and the authors reported that international teleradiology services were associated with very low rates of clinically significant errors.15
This study did not evaluate the accuracy of the diagnosis since neither computed tomographic images nor biopsy results were obtained. However, the results of previous studies supported the accuracy of teleradiology.7,12,13,15 Moreover, the diagnoses of this study were made by oral and maxillofacial radiology professors for more accurate results. Thus the results of this study might be considered to be reliable.
In the running of the teleradiology service on the website, there were issues such as uploading of images containing a patient's personal information. The patient's personal information should be treated as confidential in the transmission of medical records using a teleradiology system; therefore, the users of such system should be educated about this matter.
A few cases included a digitized image of analog film. In those cases, the quality of the image was not good enough to interpret. A previous study showed that transmission of analog film should be expected to cause image degradation and the use of film images could be difficult in teleradiology.11 In addition, the quality of a transmitted image cannot be higher than that of the original image; therefore, quality control of the image taking process would be important in each clinic.
The total number of cases, at 275, seemed to be insufficient considering the period of five years; however, it should be taken into account that this was a free pilot service and that no particular advertising was done for lack of professional human resources.
In conclusion, the introduction of a teleradiology system in general dental practice could be helpful for the differential diagnosis of common lesions and the reduccion of unnecessary costs.
Footnotes
The present research was conducted by the research fund of Dankook University in 2011.
References
- 1.Farman AG. Image communication: mailed, wired, and wireless. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;103:585–586. doi: 10.1016/j.tripleo.2006.12.034. [DOI] [PubMed] [Google Scholar]
- 2.Park W, Lee HN, Jeong JS, Kwon JH, Lee GH, Kim KD. Optimal protocol for teleconsultation with a cellular phone for dentoalveolar trauma: an in-vitro study. Imaging Sci Dent. 2012;42:71–75. doi: 10.5624/isd.2012.42.2.71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.LaBounty TM, Kim RJ, Lin FY, Budoff MJ, Weinsaft JW, Min JK. Diagnostic accuracy of coronary computed tomography angiography as interpreted on a mobile handheld phone device. JACC Cardiovasc Imaging. 2010;3:482–490. doi: 10.1016/j.jcmg.2009.11.018. [DOI] [PubMed] [Google Scholar]
- 4.Aziz SR, Ziccardi VB. Telemedicine using smartphones for oral and maxillofacial surgery consultation, communication, and treatment planning. J Oral Maxillofac Surg. 2009;67:2505–2509. doi: 10.1016/j.joms.2009.03.015. [DOI] [PubMed] [Google Scholar]
- 5.Roccia F, Spada MC, Milani B, Berrone S. Telemedicine in maxillofacial trauma: a 2-year clinical experience. J Oral Maxillofac Surg. 2005;63:1101–1105. doi: 10.1016/j.joms.2005.04.020. [DOI] [PubMed] [Google Scholar]
- 6.Salazar-Fernandez CI, Herce J, Garcia-Palma A, Delgado J, Martín JF, Soto T. Telemedicine as an effective tool for the management of temporomandibular joint disorders. J Oral Maxillofac Surg. 2012;70:295–301. doi: 10.1016/j.joms.2011.03.053. [DOI] [PubMed] [Google Scholar]
- 7.Rollert MK, Strauss RA, Abubaker AO, Hampton C. Telemedicine consultations in oral and maxillofacial surgery. J Oral Maxillofac Surg. 1999;57:136–138. doi: 10.1016/s0278-2391(99)90226-4. [DOI] [PubMed] [Google Scholar]
- 8.Brownrigg P, Lowry JC, Edmondson MJ, Langton SG. Telemedicine in oral surgery and maxillofacial trauma: a descriptive account. Telemed J E Health. 2004;10:27–31. doi: 10.1089/153056204773644544. [DOI] [PubMed] [Google Scholar]
- 9.Choi JW. Assessment of panoramic radiography as a national oral examination tool: review of the literature. Imaging Sci Dent. 2011;41:1–6. doi: 10.5624/isd.2011.41.1.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.American Dental Association, U.S. Department of Health and Human Services. The selection of patients for dental radiographic examinations [Internet] Silver Spring: American Dental Association; 2004. [cited 2012 Oct 20]. Available from: https://www.ada.org/sections/advocacy/pdfs/topics_radiography_examinations(2).pdf. [Google Scholar]
- 11.Jacobs MJ, Edmondson MJ, Lowry JC. Accuracy of diagnosis of fractures by maxillofacial and accident and emergency doctors using plain radiography compared with a telemedicine system: a prospective study. Br J Oral Maxillofac Surg. 2002;40:156–162. doi: 10.1054/bjom.2001.0751. [DOI] [PubMed] [Google Scholar]
- 12.Mistak EJ, Loushine RJ, Primack PD, West LA, Runyan DA. Interpretation of periapical lesions comparing conventional, direct digital, and telephonically transmitted radiographic images. J Endod. 1998;24:262–266. doi: 10.1016/S0099-2399(98)80110-6. [DOI] [PubMed] [Google Scholar]
- 13.Baker WP, Loushine RJ, West LA, Kudryk LV, Zadinsky JR. Interpretation of artificial and in vivo periapical bone lesions comparing conventional viewing versus a video conferencing system. J Endod. 2000;26:39–41. doi: 10.1097/00004770-200001000-00010. [DOI] [PubMed] [Google Scholar]
- 14.Torres-Pereira C, Possebon RS, Simões A, Bortoluzzi MC, Leão JC, Giovanini AF, et al. Email for distance diagnosis of oral diseases: a preliminary study of teledentistry. J Telemed Telecare. 2008;14:435–438. doi: 10.1258/jtt.2008.080510. [DOI] [PubMed] [Google Scholar]
- 15.Agrawal A, Agrawal A, Pandit M, Kalyanpur A. Systematic survey of discrepancy rates in an international teleradiology service. Emerg Radiol. 2011;18:23–29. doi: 10.1007/s10140-010-0899-2. [DOI] [PubMed] [Google Scholar]