

Abstract
In Sudan, like most developing countries, the incidence and histologic patterns of primary glomerulonephritis (GN) remains undetermined. A cross-sectional hospital-based prospective study was performed to determine the pattern of primary GN among adult Sudanese patients. The study was conducted at Khartoum Teaching Hospital from September 2010 to August 2011. It included all adult patients with suspected primary glomerular disease and who underwent native kidney biopsy. A total of 83 adult patients were biopsied with 71 patients (85.5%) being diagnosed as having primary GN. Among those with primary GN the mean age was 34.6 ± 18 years and males represent 54.9%. In 46.5% kidney biopsy was indicated by the presence of nephrotic syndrome, whereas in 33.8% biopsies were performed due to unexplained elevations in renal parameters. Primary focal segmental glomerulosclerosis (FSGS) was diagnosed in 29.6% of patients, followed by membrano-proliferative glomerulonephritis (MPGN) in 26.8% and minimal change disease in 16.9%. IgA nephropathy was observed in 5.6%. Complications following kidney biopsies were reported in 9.6% of biopsied patients. Nephrotic syndrome in an adult was the most common indication for kidney biopsy in our unit. A large number of patients were biopsied due to elevated renal parameters, which reflected the increasing awareness toward thoroughly diagnosing patients with suspected reversible kidney damage. In conclusion, FSGS and MPGN make the most common causes of primary GN among Sudanese adults. Creation of a national renal registry is essential for obtaining more specified epidemiological data.
Keywords: Adults, glomerulonephritis, kidney biopsy, Sudan
Introduction
Primary glomerulonephritis (GN) remains the leading cause of end-stage renal disease (ESRD) in many developing countries;[1] and is presumed to be responsible for 52% of patients with ESRD in Africa.[2–4] In Sudan, the overall prevalence of treated ESRD is 106 patients per million population, among these the incidence of primary GN is underdiagnosed and reported as 5.5%; whereas in more than 40%, the primary kidney disease leading to ESRD is undetermined, the patients being late presenters with established ESRD. GN remains the most probable underlying etiology in this group labeled as having ESRD of uncertain etiology.[5] Accordingly, we performed a hospital-based study, aiming to determine the pattern of primary GN among Sudanese adults.
Materials and Methods
This was a cross-sectional hospital-based prospective study aimed to determine the pattern of primary glomerular disease among adult Sudanese patients. All adult patients over the age of 15 years referred to Khartoum Teaching Hospital Renal Unit from September 2010 to August 2011, with suspected primary glomerular disease and underwent native kidney biopsies were included in the study.
Excluded from the study were kidney transplant patients, patients with lupus nephritis, diabetes mellitus, long-standing hypertension, suspected secondary glomerular disease, tubular, interstitial, or drug-induced kidney damage. Those who were found to be reactive to human immunodeficiency, hepatitis B, and hepatitis C viruses were also excluded from the study.
Ultrasound-guided kidney biopsy was performed for all selected patients using 16–18 G Tru-cut needles. Two kidney biopsy cores were taken from each patient for light microscopy and immunofluorescence techniques. For light microscopy, samples were fixed in 10% formaldehyde solution and the sections were stained with hematoxylin and eosin, periodic acid Schiff, and silver methenamine. Masson Trichrome and congo-red stains were used whenever required. Immunofluorescence microscopy panel included staining for IgA, IgG, IgM, C3, C1q, and fibrinogen. Electron microscopy study was not available for diagnostic purposes in our country. All specimens were studied by an experienced histopathologist. Repeat biopsy was performed for those with inconclusive reports or inadequate sampling.[6]
Patients’ demography, clinical presentation, diagnostic tests, indications for kidney biopsy, biopsy reports, and the observed post-biopsy complications were all noted and inputted into a specially designed questionnaire. Data were analyzed using Statistical Package for Social Sciences version 17.0 (SPSS Inc., Chicago, IL) computer software. Results were expressed as median or mean ± standard deviation for continuous data and as frequencies with percentages for categorical data. The Chi-square test was applied with statistical significance of data being considered at a P value less than 0.05.
The study was approved by the ethical committee of the Sudan Medical Specialization Board. A written consent was obtained from all patients.
Results
The study included a total of 83 adult patients with complete demographic data, clinical characteristics, laboratory investigations, and conclusive kidney biopsy reports including light microscopy and immunofluorescence techniques. In 12 out of 83 patients (14.5%) the histologic diagnosis showed atypical presentations of acute tubular necrosis, interstitial nephritis, multiple myeloma, lupus nephritis, and vasculitis whereas in 71 patients (85.5%), the diagnosis of primary GN was confirmed by kidney biopsy.
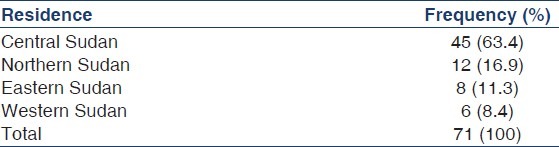
Considering those with primary GN, the majority of patients were males 39 (54.9%) whereas 32 were females (44.1%), they were predominantly housewives, 28 females, comprising 39.4% of the studied population. The mean age of the studied population was 34.6 ± 18 years (range 15–63 years). Most patients were from central Sudan 45 (63.4%), though the various geographical sectors of the country were represented in the study, as shown in Table 1.
Table 1.
Geographical distribution of the studied population
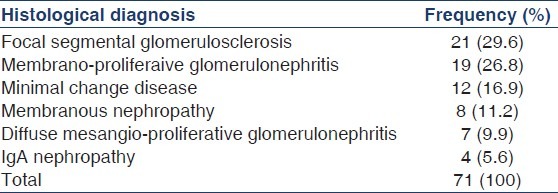
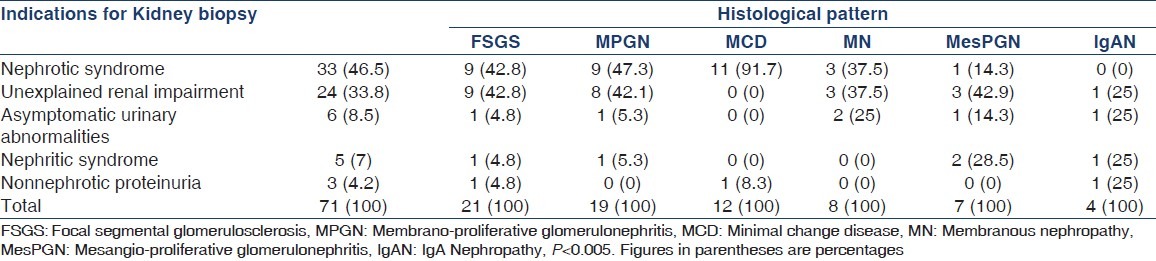
Indications for kidney biopsy were nephrotic syndrome in 33 patients (46.5%), unexplained renal impairment in 24 patients (33.8%), asymptomatic microscopic hematuria with minimal non-nephrotic range proteinuria in six patients (8.5%), nephritic syndrome in five patients (7%), and isolated non-nephrotic range proteinuria in three patients (4.2%). Focal segmental glomerulosclerosis (FSGS) was the most common glomerular lesion diagnosed in 21 patients (29.6%) followed by membrano-proliferative glomerulonephritis (MPGN) in 19 patients (26.8%), and minimal change disease (MCD) in 12 patients (16.9%), as shown in Table 2.
Table 2.
Histologic pattern of primary glomerular disease among the studied population
Regarding the various age groups of the studied population, primary GN was mostly observed between 15 and 45 years of age. There were no statistically significant correlations noted between a specific age group and the pattern of glomerular lesions diagnosed, with the P > 0.2, as shown in Table 3.
Table 3.
Pattern of primary glomerulonephritis among the various age groups

Nephrotic syndrome was the most common indication for kidney biopsy in those with FSGS, MPGN, and MCD. These findings were statistically significant with the P value less than 0.005, as shown in Table 4.
Table 4.
Clinical presentations of the various histological variants of glomerulonephritis
Complications following kidney biopsies were minimal, noticed in eight out of all biopsied patients (9.6%). These were mostly disabling pain at the site of biopsy in four patients (4.8%), massive hematuria in three patients (3.6%), and in one more patient (1.2%) the procedure was complicated by severe pain together with massive hematuria. Most patients, 75 out of 83 (90.4%), underwent the procedure without complications. Two patients (2.4%) required blood transfusions due to massive bleeding. None of our patients required further surgical or radiologic interventions and no mortality was observed following kidney biopsies.
During the 12-month study, 15 out of 21 patients with FSGS (71.4%) were controlled by steroids and maintained on immunosuppressive therapy whereas all the remaining six patients with FSGS (28.6%) required long-term dialysis replacement therapy. All patients diagnosed as having MCD during this study were treated and were able to attain complete remission with an initial course of steroids. Most of the remaining patients with primary GN, 29 out of 71 patients (40.8%) were lost to follow-up.
Discussion
There are no previous population-based epidemiological data regarding the pattern of primary GN in Sudan. This was a single centre prospective study aimed to reflect the pattern of primary GN among Sudanese adults. It was conducted at Khartoum Teaching Hospital, the biggest tertiary hospital in the country.
Similar to most previous reports, nephrotic syndrome in an adult was the most common indication for kidney biopsy in our unit, observed in 46.5% of patients. It remains the most common reported indication for adult kidney biopsy in Africa and Europe. Again a large number of patients (33.8%) were biopsied due to the presence of unexplained elevations in their renal parameters; this in turn reflected the increasing interest toward identifying the etiology in patients with renal impairment as well as in those with atypical presentations, together with the awareness regarding early referral of patients to nephrology services.[4,7]
A previous report from two renal centers in Sudan, included data from 86 renal patients, concluded that FSGS and MPGN were the most common causes of primary GN among Sudanese adults.[8] Regarding the regional description of primary GN, FSGS was the most common glomerular disease described during a 5-year study with 924 Egyptian patients, it accounted for 21% of cases of primary GN.[9] Again both FSGS and MPGN were reported by the Saudi renal registry as the leading causes of primary GN among Saudi patients.[10] From Pakistan, one retrospective study which included 1793 adult patients, reported FSGS as the most prevalent primary GN lesion noticed in 29% of patients.[11] In developed countries with registered renal data, it is known that FSGS is more prevalent among those of African descent, with a rapidly rising incidence. It was reported that the incidence of FSGS patients reaching ESRD in the United States had increased by 11-folds during the past two decades.[12]
IgA nephropathy was rarely spotted among Sudanese adults, it accounted for 5.6% of our patients and previously diagnosed in 4.7% of adult Sudanese patients with primary GN.[8] Unlike the reports from Europe and the United States, IgA nephropathy is rarely spotted in Africa accounting for 2.5-5.8% of primary GN.[4] In Saudi Arabia, Egypt, Pakistan, and India IgA nephropathy was reported as 6.5%, 9.8%, 3%, and 6.3%, respectively, among all primary GN.[10,7,13,14] It is well known that the incidence and prevalence of IgA nephropathy largely depends on the policy used in performing kidney biopsy in patients with isolated persistent microscopic hematuria and/or recurrent gross hematuria with normal renal function.[15] In our center patients with isolated micro or macroscopic hematuria are not indicated for kidney biopsy. The low incidence of IgA nephropathy thus reported is mostly due to the benign presentation of the disease.[10]
In conclusion, the most common indications for kidney biopsy were nephrosis and the presence of unexplained elevations in renal parameters in 80.3% of biopsied patients. The kidney biopsy technique was associated with minimal incidence of complications in our unit. Primary FSGS and MPGN make the most common causes of primary GN in Sudan. Like most surrounding African and Asian countries IgA nephropathy seems to be uncommon. The data available so far regarding the pattern of GN in Sudan are wholly obtained as part of experiences from a single center and reported series.[5,6,8] Only the presence of a renal registry with uniform protocols for referral and diagnosing patients with suspected GN will allow for obtaining specific epidemiological data.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Barsoum RS. Overview: End-stage renal disease in the developing world. Artif Organs. 2002;26:737–46. doi: 10.1046/j.1525-1594.2002.07061.x. [DOI] [PubMed] [Google Scholar]
- 2.Arogundade FA, Sanusi AA, Hassan MO, Akinsola A. The pattern, clinical characteristics and outcome of ESRD in Ile-Ife, Nigeria: Is there a change in trend? Afr Health Sci. 2011;11:594–601. [PMC free article] [PubMed] [Google Scholar]
- 3.Diouf B, Ka EF, Niang A, Diouf ML, Mbengue M, Diop TM. Etiologies of chronic renal insufficiency in a adult internal medicine service in Dakar. Dakar Med. 2000;45:62–5. [PubMed] [Google Scholar]
- 4.Okpechi IG, Duffield M, Swanepoe CR. Primary glomerular diseases: Variations in disease types seen in Africa and Europe. Port J Nephrol Hypert. 2012;26:25–31. [Google Scholar]
- 5.Elamin S, Obeid W, Abu-Aisha H. Renal replacement therapy in Sudan, 2009. Arab J Nephrol Transplant. 2010;3:31–6. [Google Scholar]
- 6.Abdelraheem MB, Ali el-TM, Mohamed RM, Hassan EG, Abdalla OA, Mekki SO, et al. Pattern of glomerular diseases in Sudanese children: A clinico-pathological study. Saudi J Kidney Dis Transpl. 2010;21:778–83. [PubMed] [Google Scholar]
- 7.Barsoum RS, Francis MR. Spectrum of glomerulonephritis in Egypt. Saudi J Kidney Dis Transpl. 2000;11:421–9. [PubMed] [Google Scholar]
- 8.Khalifa EH, Kaballo BG, Suleiman SM, Khalil EA, El-Hassan AM. Pattern of glomerulonephritis in Sudan: Histopathological and immunofluorescence study. Saudi J Kidney Dis Transpl. 2004;15:176–9. [PubMed] [Google Scholar]
- 9.Ibrahim S, Fayed A. The incidence of biopsy-proven glomerulonephritis in Cairo University. Egypt: A 5-year study. NDT Plus. 2009;2:431–2. doi: 10.1093/ndtplus/sfp070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Huraib S, Al Khader A, Shaheen FA, Abu Aisha H, Souqiyyeh MZ, Al Mohana F, et al. The spectrum of glomerulonephritis in Saudi Arabia: The results of the saudi registry. Saudi J Kidney Dis Transpl. 2000;11:434–41. [PubMed] [Google Scholar]
- 11.Mubarak M, Kazi JI, Naqvi R, Ahmed E, Akhter F, Naqvi SA, et al. Pattern of renal diseases observed in native renal biopsies in adults in a single centre in Pakistan. Nephrology (Carlton) 2011;16:87–92. doi: 10.1111/j.1440-1797.2010.01410.x. [DOI] [PubMed] [Google Scholar]
- 12.Kitiyakara C, Eggers P, Kopp JB. Twenty-one-year trend in ESRD due to focal segmental glomerulosclerosis in the United States. Am J Kidney Dis. 2004;44:815–25. [PubMed] [Google Scholar]
- 13.Rabbani MA, Memon GM, Ahmad B, Memon S, Tahir SA, Tahir S. Percutaneous renal biopsy results: A retrospective analysis of 511 consecutive cases. Saudi J Kidney Dis Transpl. 2012;23:614–8. [PubMed] [Google Scholar]
- 14.Das U, Dakshinamurty KV, Prayaga A. Pattern of biopsy-proven renal disease in a single center of south India: 19 years experience. Indian J Nephrol. 2011;21:250–7. doi: 10.4103/0971-4065.85482. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Muzaffar S, Azad NS, Kayani N, Pervaz S, Ahmed A, Hasan SH. The frequency of IgA nephropathy at a single centre in Pakistan. J Pak Med Assoc. 2003;53:301–5. [Google Scholar]