

Abstract
Background:
The styloid process and the attached ligaments have the potential for calcification and ossification in specific conditions. The purpose of this study was to evaluate the relationship between the elongated styloid process (ESP) frequency and some of the systemic health factors of patients over 40 years of age.
Materials and Methods:
In this analytical-descriptive study, 296 panoramic radiographs of patients over 40 years of age (165 female and 131 male) referred to the Dental School of Khorasgan Azad University were selected. The length of the styloid process was measured by a special ruler and recorded in a questionnaire form. Other data such as sex, age, height, weight, blood pressure, heartbeat and the number of teeth present in the mouth were also recorded. The lengths equal to or more than 30 mm on the radiographs were considered as ESP. Data analysis were done by independent t-test, Pearson correlation coefficient and Chi-square test at a significance level of < 0.05.
Results:
ESP was observed in 135 cases (45.6%). There was a significant relationship between ESP and the body height, weight and the blood pressure, but there was no significant correlation between ESP, the heartbeat and the number of teeth present in the mouth.
Conclusion:
Because of the significant relationship between the length of the styloid process and the blood pressure, height and weight it is reasonable to evaluate a patient's systemic health conditions when radiographic signs of ESP are observed.
Keywords: Calcification, panoramic radiograph, styloid process, systemic health factors
INTRODUCTION
The styloid process is a slender bony projection that originates from the inferior aspect of the temporal bone, anterior and medial to the stylomastoid foramen. The external and internal carotid arteries lay on either side or it is in the lateral part of the tonsil fossa and the lateral wall of the pharynx. The mean radiographic length of the process in a normal state is 20-30 mm. Although stylohyoid ligament is formed of connective tissue sometimes some amount of cartilage remains and can cause mineralization in this structure that usually develops from the base of the skull.[1] The patient may experience vague facial pain, especially while swallowing, turning the head, or opening the mouth. Other symptoms may include dysphagia, dysphonia, otalgia, headache, dizziness, and transient syncope. These symptoms are caused by impingement or compression of the adjacent nerve e.g., glossopharyngeal. Among the factors causing the elongation of the styloid process we can mention trauma to the neck region of the stylohyoid ligament e.g., tonsillectomy, developmental anatomic deviance theory and aging theory.[2,3] Elongation of the stylohyoid ligament can be seen on panoramic or lateral cephalometery radiographs.[1]
Most of the previous studies were about the prevalence of ESP and its local adverse effects. But few studies have been designed to evaluate the correlation between general health conditions such as blood pressure, heartbeat, weight, height, number of teeth and the length of the styloid process. In a recent study, it was determined that the incidence of calcified stylohyoid ligament is higher in patients with systemic diseases such as goiter, heart disease, hypertension and diabetes mellitus.[4] Another author reported that there is a correlation between the length of the styloid process, serum calcium concentration and the heel bone density in 80-year-old subjects.[5]
The clinical significance of calcified stylohyoid chain on general health is ambiguous. From an anatomic aspect the external and internal carotid arteries lay on either side and the internal jugular vein is in the medial of the styloid process so the compression of the adjacent blood vessels may be the reason for the possible relationship between blood pressure, pulse and the length of the styloid process.[6] The number of studies addressing the effect of ESP on systemic disorders must be increased to obtain more definite results. This is especially important in elderly people with various systemic and oral diseases.
The aim of this study was to determine the relationship between the elongated styloid process and some of the general health conditions (weight, blood pressure,…) in a limited Iranian population.
MATERIALS AND METHODS
In this analytical-descriptive study the sample was composed of 296 panoramic radiographs of patients over 40 years of age, referred to the Department of Radiology in Khorasgan Faculty of Dentistry. The informed consent was taken from the patients to participate in the study.
The radiographs were obtained with a Planmeca (EC Com. Finland) radiographic machine on Agfa film (15 × 30 cm. Belguim) with exposure factors depending on the subject's jaw size.
Standard position was obtained by perpendicular midsagittal plane, horizontal Frankfort plane and adjustment of mid-canine line. The radiographs with good qulity, no unevaen magnification and clear and distinctive image of styloid process on both sides, were selected. Under the supervision of the radiologist, the length of styloid process were measured by using a standard viewing box and a special ruler (RadioDent Oy, PM 2002 cc) with magnification of ½ and one millimeter error.
The measurement were done from the translucent line disrupting the base of the process from temporal bone to the bony end of the process whether it was integrated or segmented. In the case of a curved process the measurement of segments was done separately.
In this study a length of 30 mm or more was defined as an elongated styloid process.[3,7,8]
The height of the patients was measured by a standard meter and their body weight was determined by a balance (Beurer, Germany). Assessment of the blood pressure was done by a digital indicator (Beurer, B.M 50, Germany), which measured systolic and diastolic blood pressure and heartbeat of the patient. The number of teeth were counted on panoramic radiographs. Data was analyzed by independent t-test, pearson correlation relation test and Chi-Square using SPSS software.
RESULTS
Two hundred and ninety-six panoramic radiographs of 40-76-year-old patients, 165 female (55.7%) and 131 male (44.3%), were evaluated.
In general, in 135 radiographs the length of the styloid process was 30 mm or more in one or both sides. The frequency of ESP was 45.6% in the whole population (17.2% unilateral and 28.4% bilateral). The mean length of the process in patients without ESP was 27.1 mm and it was 34.5 mm in patients with ESP.
Sixty-eight males (51.9%) and 67 female (40.6%) had elongated styloid process. The Chi-square test showed a significant relationship between gender and ESP (P value = 0.03).
According to the independent t-test there was a significant relationship between height and ESP (P value = 0.001) [Table 1].
Table 1.
Correlation between elongated styloid process and various parameters of general and dental health conditions
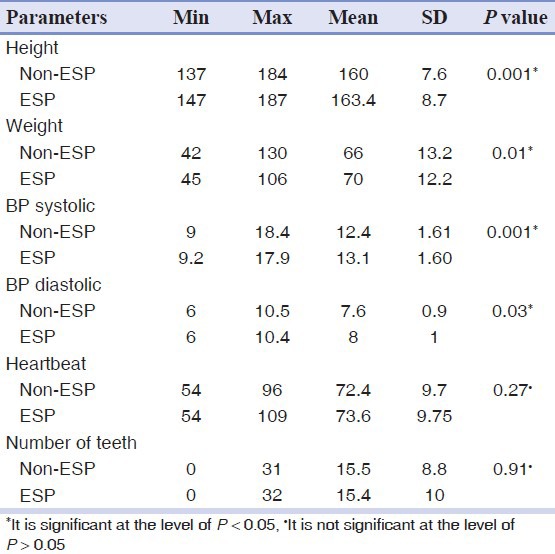
The average height in non-ESP patients was lower than unilateral and bilateral ESP patients [Figure 1]. The Pearson correlation test revealed that there was a direct, strong relation between height and ESP (P value = 0.001, r = 0.238).
Figure 1.
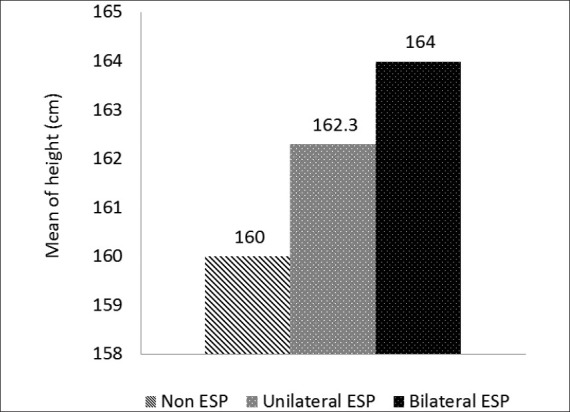
Comparison mean of height in Non-ESP, Unilateral ESP and Bilateral ESP patients
The independent t-test showed that there was a significant relationship between the weight and ESP (P value = 0.01) [Table 1].
The average weight in bilateral ESP patients was greater than unilateral and non-ESP patients [Figure 2]. The Pearson correlation test revealed that there was a direct relation between weight and ESP (P value = 0.01, r = 0.153).
Figure 2.
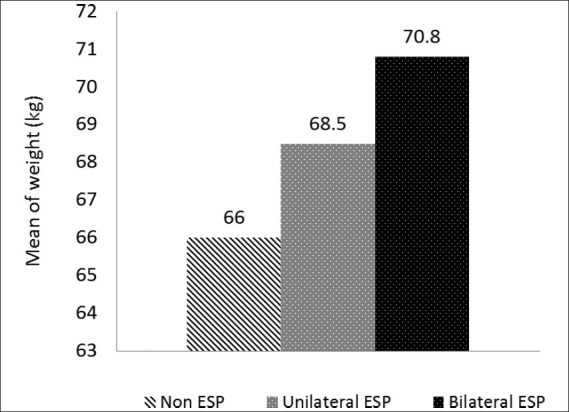
Comparison mean of weight in Non-ESP, Unilateral ESP and Bilateral ESP patients
According to the independent t-test there was a significant relationship between the systolic blood pressure and ESP (P value = 0.001) and diastolic blood pressure and ESP (P value = 0.03) [Table 1].
The average blood pressure in bilateral ESP patients was higher than in unilateral and non-ESP patients [Figures 3 and 4]. The Pearson correlation test revealed that there was a direct relation between systolic blood pressure and ESP (P value = 0.001, r = 0.210) and diastolic blood pressure and ESP (P value = 0.03, r = 0.126).
Figure 3.
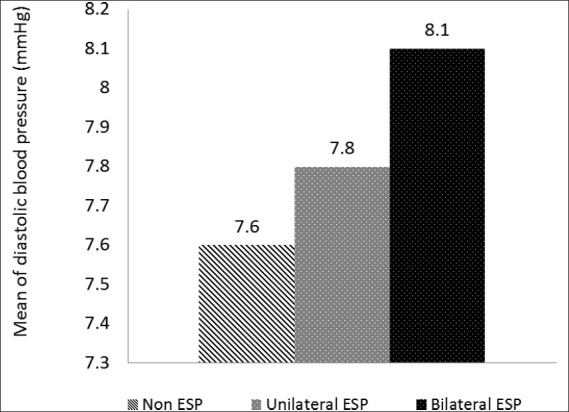
Comparison mean of diastolic blood pressure in Non-ESP, Unilateral ESP and Bilateral ESP patients
Figure 4.
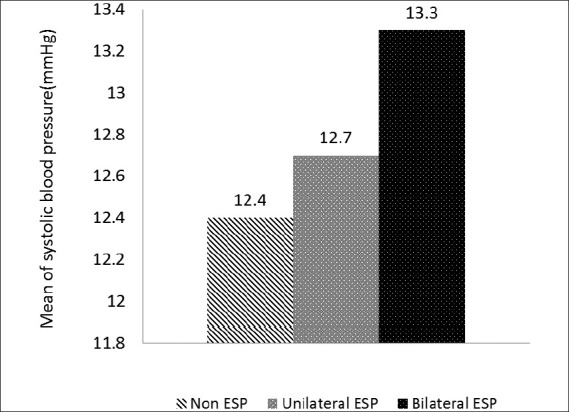
Comparison mean of systolic blood pressure in Non-ESP, Unilateral ESP and Bilateral ESP patients
The independent t-test showed that there was no significant relationship between the heartbeat and ESP (P value = 0.27).
The independent t-test revealed that there was no significant correlation between the number of teeth in the mouth and ESP (P value = 0.91).
DISCUSSION
The studies in which ESP prevalence in different populations have been reported indicate a wide range of prevalence.[7,9,10,11,12,13] In the present study, the average length of the process in non-ESP patients was 27.1 mm and it was 34.5 mm in those with elongated styloid process. The ESP rate was 45.6% which is high. The prevalence could be high in the Iranian population as demonstrated by a study conducted by Ghafari-Abdollahpur on 1 1-70 5-year–old patients from the Gilan province in which the prevalence was reported to be 36.4%.[6] Since the ESP rate increases with age[4] and the age range in this study is over 40, the rate of an elongated process in this study is greater than that of Ghafari-Abdollahpur study which was conducted over a wide range of ages. Some studies reported 1 8-40 0% prevalence in the population.[9] According to Ferrario et al., it is impossible to compare the results from ESP occurrence, because the differential radiographic criteria, unit magnification, and sample size vary in different studies.[11]
In this study, the rate of ESP was greater in males than in females. In most studies, the possibility of ESP involvement is reported to be equal in both sexes.[2,5,7,8,10,11,14,15] By selecting an equal sample size of edentulous males and females, Bozkir demonstrated that statistically there was no significant difference between the two sexes.[1] In a study by Ilguy, the ratio of female to male involvement was reported to be 3 to 1.[13] In two separate studies by Young et al., and Ghafari-Abdullahpur, the rate of ESP was reported to be greater in males than in females,[6,16] a result which agrees with the results of the present study. Racial, cultural, climatic, nutrition and physiological (sexual hormones) differences may be responsible for the higher incidence of ESP in males in the community being studied.[6]
In the present study, bilateral ESP involvement was 1.6 times more than the unilateral involvement. In a study which was done by Bozkir in Turkey and also in another study by Ghafari-Abdullahpur, the frequency of bilateral involvement was reported to be three times greater than that of the unilateral one.[1,6] This is perhaps because of a similarity in Iranian and Turkish genotypes and phenotypes. On the other hand Rizzatti Barbosa et al., reported an equal prevalence for both unilateral and bilateral ESP.[12] However, Scaf et al., stated that 90.5% of ESP involvements were unilateral. They demonstrated that the muscle tension from occlusal disarrangements could be a probable factor.[2]
In the present study, we evaluated the general health conditions including body height, weight, blood pressure, and heartbeat in patients with and without ESP. There was a significant correlation between the elongation of the process and the patients’ height and weight which supports the growth theory. Although in Okabe's study this correlation was not confirmed.[5]
A significant correlation between the blood pressure and the elongation of the styloid process was found that can be due to the anatomy of the area, for example, compression of the external carotid artery of symptomatic patients was viewed on angiographic images.[17] In addition, Oztas reported that there was a significant relation between systemic disorders (e.g., hypertension, heart disease,…) and styloid ligament calcification.[4] However, in a study by Okabe et al., there was no significant correlation between blood pressure and the elongation of the styloid process.[5]
There was no significant correlation between the frequency of the heartbeat and the elongation of the styloid process which agrees with the findings in a study by Okabe et al.[5]
Since the muscle tension from occlusal disarrangements and changes in bone height in partial or complete edentulous patients can be a probable factor in the incidence of ESP[2] the association between the number of teeth present in the mouth and the elongation of the styloid process was studied, but no significant correlation was found between the two, which was consistent with the study conducted by Okabe et al.[5]
CONCLUSION
The present study indicates that panoramic radiographs include information on general health conditions as well as on teeth and jaws.
Because of the significant relationship between the length of the styloid process and the blood pressure, height and weight it is reasonable to evaluate a patient's systemic health conditions when radiographic signs of ESP are observed.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Bozkir MG, Boga H, Dere F. The Evaluation of Elongated Styloid Process in Panoramic Radiographs in Edentulous Patients. J Med Sci. 1999;29:481–5. [Google Scholar]
- 2.Scaf G, Freitas DQ, Loffredo Lde C. Diagnostic Reproducibility of the Elongated Styloid Process. J Appl Oral Sci. 2003;11:120–4. doi: 10.1590/s1678-77572003000200007. [DOI] [PubMed] [Google Scholar]
- 3.Zaki HS, Greco CM, Rudy TE, Kubinski JA. Elongated styloid process in a temporomandibular disorder sample: Prevalence and treatment outcome. J Prosthet Dent. 1996;75:399–405. doi: 10.1016/s0022-3913(96)90032-3. [DOI] [PubMed] [Google Scholar]
- 4.Oztas B, Orhan K. Investigation of the incidence of stylohyoid ligament calcification with panoramic radiographs. J Investig Clin Dent. 2012;3:30–5. doi: 10.1111/j.2041-1626.2011.00081.x. [DOI] [PubMed] [Google Scholar]
- 5.Okabe S, Morimoto Y, Ansai T, Yamada K, Tanaka T, Awano S, et al. Clinical significance and variation of the advanced calcified stylohyoid complex detected by panoramic radiographs among 80-year-old subjects. Dentomaxillofac Radiol. 2006;35:191–9. doi: 10.1259/dmfr/12056500. [DOI] [PubMed] [Google Scholar]
- 6.Ghafari R, Dalili Z, Abdolahpur S. A study on the frequency of elongated styloid process and eagle's syndrome among patients admitted to Guilan dental school clinic (2005-2006) J Isfahan Dent Sch. 2010;6:108–15. [Google Scholar]
- 7.Correll RW, Jensen JL, Taylor JB, Rhyne RR. Mineralization of the stylohyoid-stylomandibular ligament complex. A radiographic incidence study. Oral Surg Oral Med Oral Pathol. 1979;48:286–91. doi: 10.1016/0030-4220(79)90025-2. [DOI] [PubMed] [Google Scholar]
- 8.Keur JJ, Campbell JP, McCarthy JF, Ralph WJ. The clinical significance of the elongated styloid process. Oral Surg Oral Med Oral Pathol. 1986;61:399–404. doi: 10.1016/0030-4220(86)90426-3. [DOI] [PubMed] [Google Scholar]
- 9.Neville B, Damm D, Allen C, Bouquot J. J Oral and maxillofacial pathology. 3rd ed. Saunders Elsevier; 2009. pp. 23–4. chap 1. [Google Scholar]
- 10.MacDonald-Jankowski DS. Calcification of the stylohyoid complex in Londoners and Hong Kong Chinese. Dentomaxillofac Radiol. 2001;30:35–9. doi: 10.1038/sj/dmfr/4600574. [DOI] [PubMed] [Google Scholar]
- 11.Ferrario VF, Sigurtá D, Daddona A, Dalloca L, Miani A, Tafuro F, et al. Calcification of the stylohyoid ligament: Incidence and morphoquantitative evaluations. Oral Surg Oral Med Oral Pathol. 1990;69:524–9. doi: 10.1016/0030-4220(90)90390-e. [DOI] [PubMed] [Google Scholar]
- 12.Rizzatti-Barbosa CM, Ribeiro MC, Silva-Concilio LR, Di Hipolito O, Ambrosano GM. Is an elongated stylohyoid process prevalent in the elderly? A radiographic study in a Brazilian population? Gerodontology. 2005;22:112–5. doi: 10.1111/j.1741-2358.2005.00046.x. [DOI] [PubMed] [Google Scholar]
- 13.Ilgüy M, Ilgüy D, Güler N, Bayirli G. Incidence of The type and calcification patterns in patients with elongated styloid process. J Int Med Res. 2005;33:96–102. doi: 10.1177/147323000503300110. [DOI] [PubMed] [Google Scholar]
- 14.Monsour PA, Yougn WG. Variability of the styloid process and stylohyoid ligament in panoracmic radiographs. Oral Surg Oral Med Oral Pathol. 1986;61:522–6. doi: 10.1016/0030-4220(86)90399-3. [DOI] [PubMed] [Google Scholar]
- 15.Carmada AJ, Deschamps C, Forest D. Stylohyoid chain ossification: A Discussion of etiology. Oral Surg Oral Med Oral Pathol. 1989;67:515–20. doi: 10.1016/0030-4220(89)90265-x. [DOI] [PubMed] [Google Scholar]
- 16.Young Hwang J, Hwang EH, Lee SR. A study on the styloid process in panoramic radiographs. Korean J Oral Maxillofac Radiol. 2005;35:105–10. [Google Scholar]
- 17.Ohtsuka K, Tomita H, Murakami G. Anatomical study of the tonsillar bed-hetopographical relationship between the palatine tonsil and the lingual branch of the glossopharyngeal nerve. Nihon Jibiinkoka Gakkai Kaiho. 1994;97:1481–93. doi: 10.3950/jibiinkoka.97.1481. [DOI] [PubMed] [Google Scholar]