

Abstract
The presence of salivary gland tissue in the sella turcica has rarely been reported, mainly after pituitary examination at autopsy. Only five symptomatic cases have previously been described, mainly associated with Rathke’s cleft cyst. We report a 17-year-old boy presenting with headaches and hyperprolactinemia. The MRI showed a 19 mm sellar mass that at surgery revealed as a cystic lesion filled with mucinous fluid. The histological examination documented the presence of ectopic salivary gland tissue in the wall of a Rathke’s cleft cyst. The present report focuses on the possible pitfalls when dealing with unusual sellar lesions, and the need of increased awareness of this rare condition.
Keywords: Salivary gland tissue, pituitary, Rathke’s cleft cyst
Introduction
The first report of salivary tissue in the pituitary gland was made in 1940 by Erdheim [1]. By investigating pituitary glands in 2,300 consecutive autopsies on both adults and children, Schochet et al. found the presence of salivary gland rests in 78 cases [2]. Few cases of ectopic normal salivary gland tissue associated with Rathke’s cleft cyst and accompanied by hormonal abnormalities, as well as rare salivary gland-like tumors in the sellar region have been reported [3-9]. Both clinically and radiologically these entities frequently mimic pituitary neoplasms, primarily adenomas.
We report a 17-year-old man with a pituitary symptomatic mass that, at histological examination, consisted of a Rathke’s cleft cyst containing salivary tissue in the wall. Furthermore, we will briefly discuss the possible pathogenesis for this rare condition.
Case report
A 17-year-old male presented with a six-month history of headaches and nausea. No other neuro-ophthalmological symptoms were present. Magnetic resonance imaging (MRI) revealed an intra-suprasellar lesion (19 mm in diameter) which showed no enhancement after gadolinium administration (Figure 1). Hormonal assays documented hyperprolactinemia (83.5 ng/ml; normal range: 3.5-15.5 ng/ml), but others pituitary hormone levels were within normal range.
Figure 1.
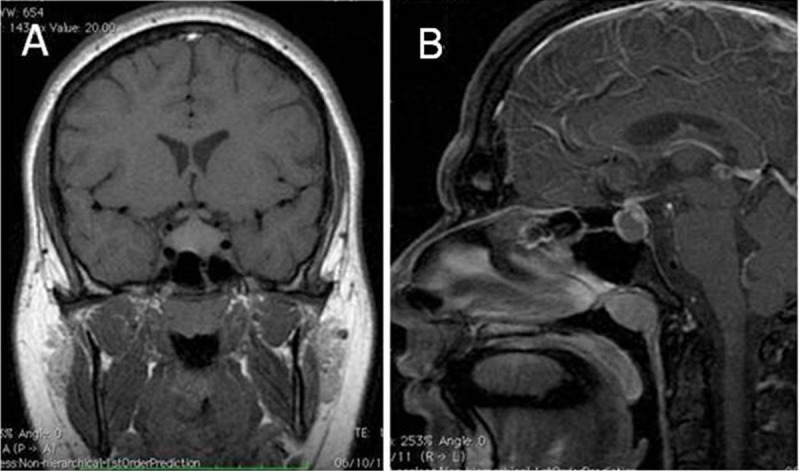
Coronal T1w (A) and sagittal T1w (B) brain MRI with gadolinium display an intra-suprasellar non enhancing mass lesion, contacting the medial cavernous sinuses walls bilaterally, and with cranial extension in close proximity of the optic chiasm.
The patient underwent transphenoidal excision of the lesion, that intraoperatively appeared cystic and filled with a yellowish, mucinous fluid (Figure 2). The postoperative course was uneventful, and the prolactin level lowered to 33.1 ng/ml. A postoperative MRI examination documented the absence of further evident abnormalities. Macroscopically, the specimen was composed of mucoid material and small tissue fragments. The biopsy was formalin fixed and paraffin embedded. Five micron sections were stained with hematoxylin and eosin. For immunohistochemistry, the sections were stained with antibodies against CAM 5.2, glial fibrillary acidic antigen, epithelial membrane antigen, synaptophysin and Ki-67, using the ABC method. Histological examination showed fragments of normal pituitary tissue admixed with normal-appearing salivary tissue, organized in lobules of seromucous glands, embedded in a fibrovascular network (Figure 3A).Fragments of ciliated or squamous epithelium, constituting the lining of the Rathke’s cyst were also found (Figure 3B). No atypias were observed. Immunohistochemical analysis showed immunoreactivity for synaptophysin and cytokeratin in the adenohypophyseal tissue and the proliferative activity, assessed by anti-Ki67 antibody, was unnoticeable. The histological diagnosis was ectopic salivary tissue in Rathke’s cleft cyst.
Figure 2.
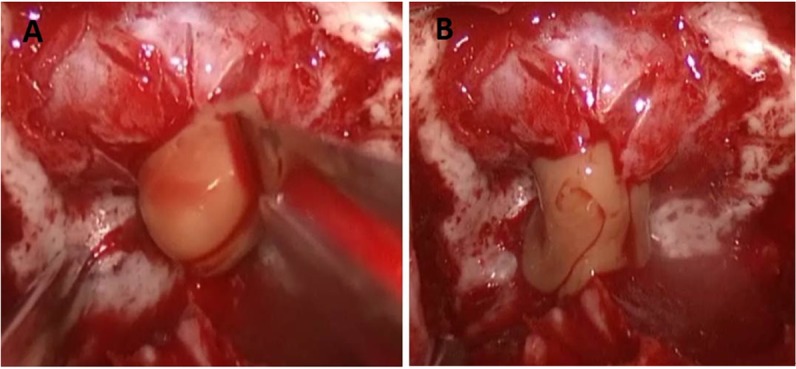
Intraoperative picture before (A) and after (B) sellar dura incision, showing a mucinous yellowish fluid flowing from the cyst.
Figure 3.
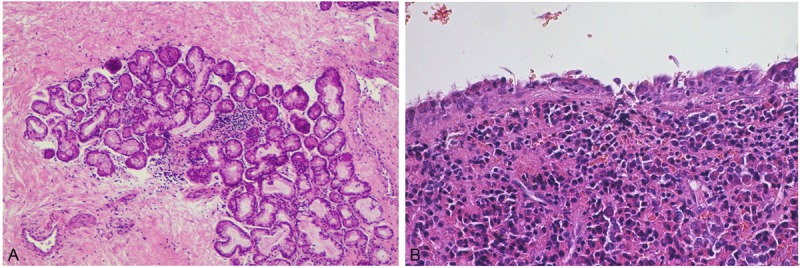
Microscopic features. A: Salivary tissue contained in the cyst wall (HE, x100). B: Ciliated epithelial lining of the Rathke cleft cyst abutting on adenohypophyseal tissue (HE, x200).
Discussion
Heterotopic salivary gland tissue is usually described in the head and neck region, where it is subject to the same pathologic changes as its orthotopic counterpart, including cyst formation, oncocytic metaplasia, ductal hyperplasia, and neoplasms [10].
Presence of ectopic salivary tissue in the pituitary gland is a rare finding. Erdheim was the first to describe “tubular glands” in the pituitary, recognizing their salivary nature [1]. Schochet et al, investigating pituitary glands at autopsy, found presence of salivary gland rests in about 3% of 2,300 autopsies [2]. However, the presence of salivary ectopic tissue rarely becomes symptomatic for a mass effect or endocrine abnormalities: in these cases, an association with a Rathke’s cleft cyst has been more frequently reported [3-7]. In addition, occasional salivary gland-derived tumors have been described in the pituitary [8,9].
The presence of salivary gland rests in the sellar region is probably related to the embryologic development of the pituitary gland from Rathke’s pouch, which, by the fourth to fifth week of human gestation, invaginates from the primitive oral cavity, migrates towards the base of the brain, and fuses with an extension of the floor of the third ventricle, giving rise to the pituitary gland [11]. The pouch closes early in embryonic life, but its apical extremity persists in postnatal life as a cleft between the anterior and posterior lobe of the hypophysis [3]. One possible explanation for this abnormal finding is the direct transfer of preexisting seromucous glands from the oral cavity to the sellar region, driven by the Rathke’s pouch migration. An alternative explanation could be a differentiation into both salivary and adenohypophyseal tissues of Rathke’s pouch components. In this respect, experimental in vivo studies have documented that during murine organogenesis salivary gland-like tissue can develop from pituitary epithelium in vitro recombined with submandibular gland mesenchyme. In fact, it is possible that during human embryogenesis, mesenchymal components, accompanying Rathke’ s pouch in the sella, can induce primitive pituitary epithelium to differentiate towards salivary gland tissue.
Moreover, it is possible that in rare cases this “ectopic” salivary tissue undergoes neoplastic transformation, giving rise to a spectrum of neoplasms similar to those found in salivary glands, as reported in the literature [8,9]. The present report emphasizes the risk of pitfalls when dealing with unusual sellar lesions, and the need of increased awareness of this rare condition.
Disclosure of conflict of interest
The authors have no conflict of interest.
References
- 1.Romeis B. Innersekretorische Drüsen II. Hypophyse. In: von Möllendorff W, editor. Handbuch der Mikroskopischen Anatomie des Menschen. Berlin: Springer Verlag; 1940. pp. 338–349. [Google Scholar]
- 2.Schochet SS Jr, McCormick WF, Halmi NS. Salivary gland rests in the human pituitary. Light and electron microscopical study. Arch Pathol. 1974;98:193–200. [PubMed] [Google Scholar]
- 3.Fager CA, Carter H. Intrasellar epithelial cysts. J Neurosurg. 1966;24:77–81. doi: 10.3171/jns.1966.24.1.0077. [DOI] [PubMed] [Google Scholar]
- 4.Kato T, Aida T, Abe H, Miyamachi K, Hida K, Taneda M, Ogata A. Ectopic salivary gland within the pituitary gland. Neurol Med Chir. 1988;28:930–933. doi: 10.2176/nmc.28.930. [DOI] [PubMed] [Google Scholar]
- 5.Tatter SB, Edgar MA, Klibanski A, Swearingen B. Symptomatic salivary-rest cyst of the sella turcica. Acta Neurochir (Wien) 1995;135:150–153. doi: 10.1007/BF02187760. [DOI] [PubMed] [Google Scholar]
- 6.Chen CH, Hsu SS, Lai PH, Lo YS. Intrasellar symptomatic salivary gland rest. J Chin Med Ass. 2007;70:215–217. doi: 10.1016/S1726-4901(09)70361-2. [DOI] [PubMed] [Google Scholar]
- 7.Stefanits H, Matula C, Frischer JM, Furtner J, Hainfellner JA, Woehrer A. Innervated ectopic salivary gland associated with Rathke’s cleft cyst clinically mimicking pituitary adenoma. Clin Neuropathol. 2013;32:171–175. doi: 10.5414/NP300560. [DOI] [PubMed] [Google Scholar]
- 8.Hampton TA, Scheithauer BW, Rojiani AM, Kovacs K, Horvath E, Vogt P. Salivary gland-like tumors of the sellar region. Am J Surg Pathol. 1997;21:424–434. doi: 10.1097/00000478-199704000-00008. [DOI] [PubMed] [Google Scholar]
- 9.Chimelli L, Gadelha MR, Une K, Carlos S, Pereira PJM, Santos JL, Niemeyer Filho P, Duarte F. Intra-sellar salivary gland-like pleomorphic adenoma arising within the wall of a Rathke’s cleft cyst. Pituitary. 2000;3:257–261. doi: 10.1023/a:1012888315577. [DOI] [PubMed] [Google Scholar]
- 10.Rosai J. Rosai and Ackerman’s Surgical Pathology. Mosby; 2011. p. 818. [Google Scholar]
- 11.Kusakabe M, Sakakura T, Sano M, Nishizuka Y. A pituitary-salivary mixed gland induced by tissue recombination of embryonic pituitary epithelium and embryonic submandibular gland mesenchyme in mice. Dev Biol. 1985;110:382–391. doi: 10.1016/0012-1606(85)90097-1. [DOI] [PubMed] [Google Scholar]