

Abstract
We report a rare case of adenocarcinoma in retroperitoneal teratoma in a 38 year old female patient who attended surgical OPD with complaints of dragging pain and heaviness in left lumbar region. Straight x-ray abdomen showed few irregular calcifications in left lumbar region. USG and CT showed it to be adrenal tumor and retroperitoneal teratoma respectively. Excised specimen confirmed it as mucin secreting adenocarcinoma in a case of retroperitoneal teratoma.
Keywords: Adenocarcinoma, Retroperitoneal, Teratoma
Introduction
Teratoma contains somatic cell types from two or more germ layers i.e. ectoderm, mesoderm and endoderm. Malignant transformation of different somatic cell type may occur and these resemble non-germ cell tumor (GCT) somatic cancers. Though malignant change of retroperitoneal teratoma is less common, it may occur rarely but conversion to adenocarcinoma is rarer. Only 16 cases have been reported so far.
Case Report
A 38 year old female, attended surgical OPD with occasional pain and heaviness in left middle abdomen. History of vomiting, dysuria, haematuria, diarrhoea and menstrual irregularities were absent.
Straight x-ray abdomen showed few irregular calcifications in left lumbar region. USG abdomen showed a large complex mass lesion showing cystic, solid and calcific areas in left adrenal region measuring 10 × 7 cm. (Fig. 1). IVU showed normal functioning kidneys. CECT abdomen showed an intra abdominal mixed lesion in left side of abdomen with multi septated cystic component, fat attenuating areas, solid components, marginal and intra lesional calcifications with,tooth element, likely teratodermoid cyst (Fig. 2).
Fig. 1.

USG abdomen
Fig. 2.
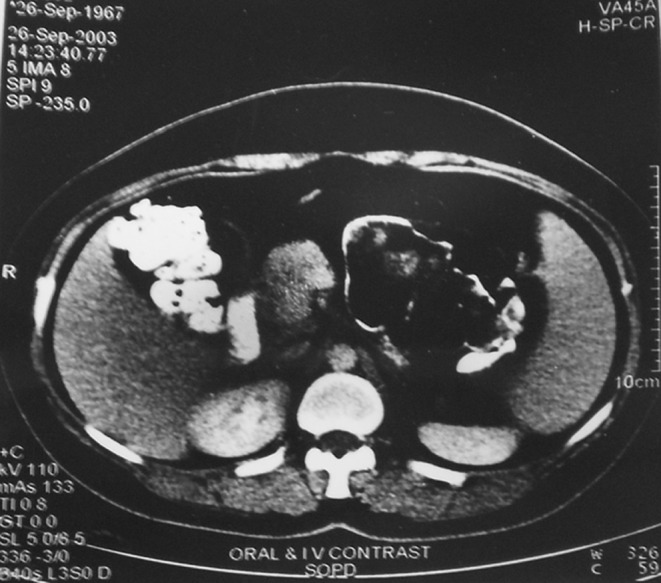
CT scan abdomen
On exploration of abdomen, a large swelling in retroperitoneum, about 14 × 8 cm in size, in between kidney and stomach that was firm and lobulated was found. The mass was removed without difficulty. Cut surface showed circumscribed nodular mass, with cystic degeneration and calcification. Fatty tissue, hair and solid mucoid areas were found (Fig. 3).
Fig. 3.
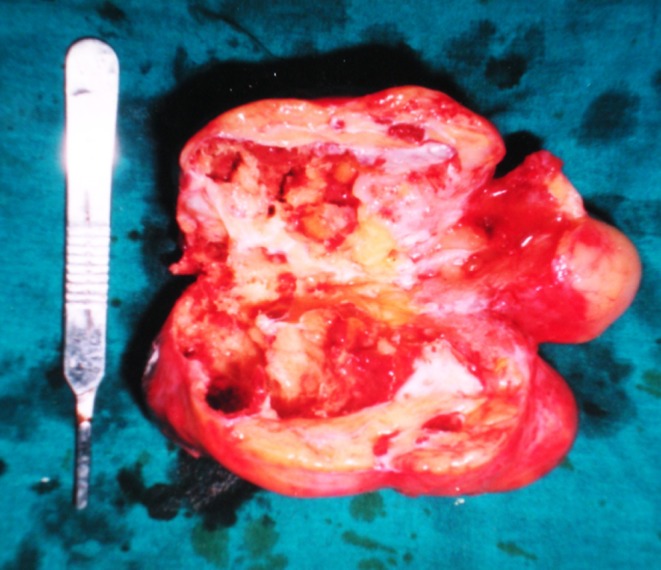
Specimen (cut surface)
Microscopical examination showed tumor composed of ectodermal, mesodermal and entodermal elements. Mature adipose tissues, bundles of muscle fibres, cartilage, respiratory epithelium, lymphoid tissue, bronchial epithelium, glial tissue and stratified squamous epithelium were present. The mucoid areas showed mucin secreting adenocarcinoma (Fig. 4).
Fig. 4.
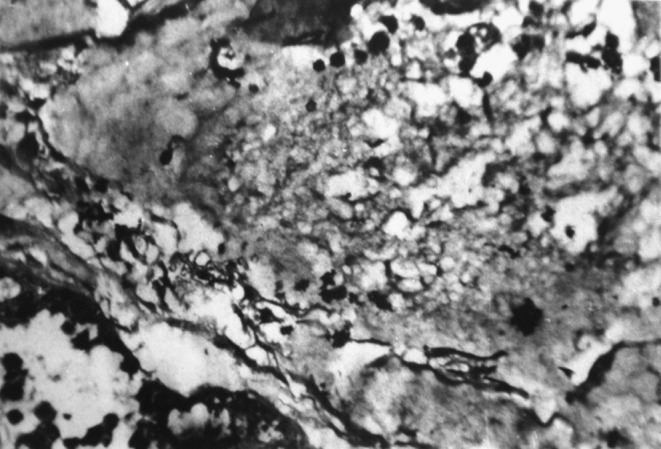
Microscopic examination
Discussion
Teratoma are of two types—immature and mature which are histologically benign tumors but malignant transformation may occur which resemble non-GCT somatic cancers [1]. Teratoma may be cystic or solid. Cystic tumors are usually benign but solid tumors are usually malignant [2]. Somatic non-GCT malignancy arising in teratoma behaves like cancer at de novo site and treatment should be directed accordingly [3]. During operation frozen section biopsy can diagnose the condition. Levels of raised CEA and CA19-9 may be present but are not very helpful [4].
Cases with different types of adenocarcinomas have been reported viz., gastric, small intestinal and colonic [5].
Definitive diagnosis is mainly done post-operatively. Mucinous changes in a teratoma as shown by CT/MRI may be an indicator together with invasion to surrounding tissues. The CT and MRI can differentiate malignant changes from benign tumor early [6].
As adenocarcinoma in teratoma is resistant to chemotherapy and recurrence is common, complete surgical resection must be done. Adhesion, adenocarcinoma and tumor rupture indicates poor prognosis. Post-operative chemotherapy, radiotherapy is not very effective. Paclitaxel with cisplatin or carboplatin combination therapy may be used [7].
Conclusion
The case—a rare one—was referred to our hospital from the periphery centre as left sided adrenal mass. CT confirmed it as retroperitoneal teratodermoid cyst. Histopathological examination of the solid mass in the swelling showed adenocarcinoma. Chemotherapy was administered though effect was not established. Patient was followed-up for 6 months and then lost. There was no recurrence within this period.
Contributor Information
Sushil Ranjan Ghosal, Email: srghosal@gmail.com.
Subhabrata Das, Email: puludas@gmail.com.
Abhiram Maji, Email: dr.abhiram09@gmail.com.
Krishna Kamal Dey, Email: krishnakamalburdwan@yahoo.com.in.
Dibakar Bagchi, Email: drdibakarbagchi@gmail.com.
References
- 1.DeVita, Hellman, Rosenberg (2008) Principles & practice of oncology Vol. I, 8th edn. Lippencott Williams & Wilkins, p 1465
- 2.Renato F, Paolo V, Giralamo M, Vigano L, Alessandro P, Claudio V, et al. Malignant retroperitoneal teratoma: case report and literature review. Acta Urol Belg. 1996;64:49–54. [PubMed] [Google Scholar]
- 3.Donadio AC, Motzer RJ, Bajorin DF, et al. Chemotherapy for teratoma with malignant transformation. J Clin Oncol. 2003;21:4285. doi: 10.1200/JCO.2003.01.019. [DOI] [PubMed] [Google Scholar]
- 4.Joseph LD, Karmani Deus M, Sandara S, Rajendra S. Squamous cell carcinoma arising from primary retroperitoneal mature teratoma. JAPI. 2007;55:374. [PubMed] [Google Scholar]
- 5.Cao D, Cheung WL. Colonic type adenocarcinoma arising in primary retroperitoneal mature cystic teratoma. Path Int. 2008;58(12):792–796. doi: 10.1111/j.1440-1827.2008.02313.x. [DOI] [PubMed] [Google Scholar]
- 6.Wang LJ, Chu SH, Ng KF, Wong YC. Adenocarcinoma arising from primary retroperitoneal mature teratomas: CT and MR imaging. Eur Radiol. 2002;12:1546–1549. doi: 10.1007/s003300101105. [DOI] [PubMed] [Google Scholar]
- 7.Kim JH, Lee TS, Oh Hk, Choi Ys. A case of mucinous adenocarcinoma arising from retroperitoneal teratoma treated with chemoradiation. J Gynae Oncol. 2009;20:126–128. doi: 10.3802/jgo.2009.20.2.126. [DOI] [PMC free article] [PubMed] [Google Scholar]