

Abstract
An obturator hernia is a rare variety of abdominal hernia that presents with a confusing clinical picture. We present a case of 74-year-old woman who admitted to our hospital because of abdominal distention, abdominal pain, and vomiting for 3 days. Incarcerated intestinal obstruction due to the right-sided obturator hernia was found preoperatively. Perforation of the small bowel due to incarceration was noted during laparotomy. Bowel resection and anastomosis were done. She was recovered after 15 days of postoperative care. In this case report, we emphasize that preoperative high index of suspicion is required for diagnosis and treatment.
Keywords: Intestinal obstruction, Obturator hernia
Introduction
The obturator hernia was first described in 1724 and was recently reported in 0.07–1.0% of all hernias and 0.2–1.6% of all cases of mechanical bowel obstruction of small bowel [1].
The higher incidence rate has been shown in Asians compared with white western population [1].
There are three stages of the obturator hernia:
Entrance of preperitoneal fat
Dimple in peritoneum overlying the canal
Onset of symptoms due to entrances of the organ into the canal
The organ can be small bowel, large bowel, omentum, fallopian tube, and appendix [2].
In our case the small bowel was obstructed in the obturator canal that results in bowel perforation, septic shock.
Case Report
A 74-year-old woman (multiparous) admitted to our ward with complaints of abdominal distension, abdominal pain, and vomiting for 3 days. The vitals of patients were stable.
Physical examination revealed that abdomen was distended and tympanic. There was tenderness in the lower abdomen which seemed that bowel loops were together in the lower abdomen.
Abdominal X-rays in upright position showed multiple air-fluid levels. The leucocytes count was raised, but all other biochemical investigations were within normal limits.
The patient was taken to the operation theater for urgent surgery with diagnosis of acute intestinal obstruction.
Abdominal exploration was performed through a mid midline incision, and it was observed that great portion of small intestine was distended.
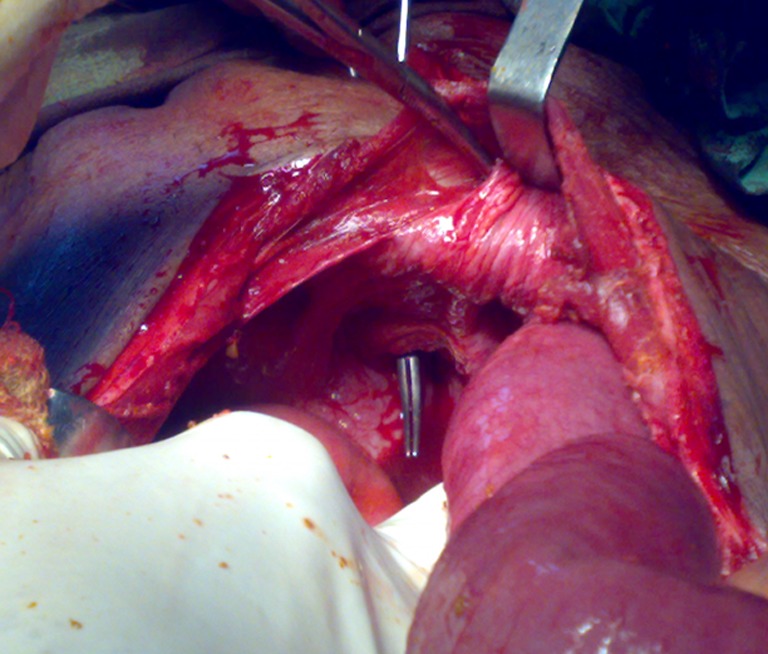
Approximately 1.5 ft proximal to ileocecal junction, a loop of small bowel was found incarcerated within the right obturator foramen (Fig. 1).
Fig. 1.

Incarcerated and perforated bowel in the right-sided obturator canal
The intestinal loop in the hernia sac was freed and taken into the abdominal cavity by loosening the obturator canal with a small anteromedial incision and with the aid of a clamp (Fig. 2).
Fig. 2.
An obturator canal with the aid of a clamp
During evaluation other hernial sites were normal (Fig. 3).
Fig. 3.

Other hernial sites
About 5 cm incarcerated and perforated part of gut was resected and anastomosis was done. For the obturator hernia, single suture of Prolene 2-0 was taken to occlude the lumen.
After thorough wash of the abdominal cavity, an abdominal drain was fixed and the abdominal cavity was closed.
Postoperatively the patient developed septic shock, but she fully recovered after 12 days and discharged on day 15.
Discussion
The obturator hernia was initially described by Arnaudde Ronsil in 1724 and was first successfully repaired in 1851 by Henry Obre [3].
The obturator hernia occurs through the obturator canal, which is 2–3 cm long and 1 cm wide, and contains the obturator nerve and vessels. It is bounded superiorly and laterally by the pubic bone and inferiorly by the obturator membrane. Corpus adiposum is a cushion for the obturator nerve. The obturator hernia is nine times more common in females due to their wider pelvis, more triangular obturator canal opening, and greater transverse diameter. It occurs most frequently in emaciated patients aged between 70 and 90 years, and hence its nickname “little old lady’s hernia.” The loss of protective preperitoneal fat and lymphatic tissue (corpus adiposum) around the obturator vessels and nerves facilitates the formation of hernia [4].
Symptoms of bowel obstruction, including dull, cramping abdominal pain, nausea, and vomiting, are reported in more than 80% of patients with the obturator hernia [5].
Compression of the obturator nerve by the hernial sac produces the pathognomonic Howship-Romberg sign in 12.5–65.0% of patients [5]. The loss of adductor reflex due to compression of the obturator nerve has been termed Hannington-Kiff sign [5]. These signs were absent in our case or overlooked because of low index of suspicion.
Abdominal radiography is most often nonspecific, showing features of bowel obstruction as seen in our case, but recent series have obtained a 75–100% preoperative diagnosis by using ultrasonography and computed tomography [6].
Delay in diagnosis or operative intervention contributes substantially to morbidity and mortality [7].
The intra-abdominal approach through a low midline incision is most commonly used as it can establish the diagnosis, avoid the obturator vessels, expose the obturator ring, and facilitate bowel resection [8].
The close of the obturator canal defect can be done primarily if contamination due to perforation of gut is there (as in our case) or mesh fixation can be done with polypropylene mesh [8]. Contralateral obturator canal defect is rarely repaired due to low recurrence rate [8].
In conclusion, the obturator hernia remains an unusual but important diagnosis in elderly thin patients with intestinal obstruction.
Contributor Information
Dhiraj Agarwal, Email: drdhiraj17@rediffmail.com.
Jagdeep Rao, Email: drjagdeeprao@yahoo.com.
References
- 1.Yip AW, AhChong AK, Lam KH. Obturator hernia: a continuing diagnostic challenge. Surgery. 1993;113:266–269. [PubMed] [Google Scholar]
- 2.Gray SW, Skandalakis JE, Soria RE, Rowe JS., Jr Strangulated obturator hernia. Surgery. 1974;75:20–27. [PubMed] [Google Scholar]
- 3.Chang SS, Shan YS, Lin YJ, Tai YS, Lin PW. A review of obturator hernia and a proposed algorithm for its diagnosis and treatment. World J Surg. 2005;29:450–454. doi: 10.1007/s00268-004-7664-1. [DOI] [PubMed] [Google Scholar]
- 4.Bjork KJ, Mucha P, Jr, Cahill DR. Obturator hernia. Surg Gynecol Obstet. 1998;167:217–222. [PubMed] [Google Scholar]
- 5.Shipkov CD, Uchikov AP, Griqoriadis E. The obturator hernia: difficult to diagnose, easy to repair. Hernia. 2004;8:155–157. doi: 10.1007/s10029-003-0177-2. [DOI] [PubMed] [Google Scholar]
- 6.Chin LW, Chou MC, Wang HP, Bell W. Ultrasonography diagnosis of occult obturator hernia presenting as intestinal obstruction in ED. Am J Emerg Med. 2005;23:237–239. doi: 10.1016/j.ajem.2004.02.047. [DOI] [PubMed] [Google Scholar]
- 7.Kammori M, Mafune K, Hirashima T, Kawahara M, Hashimoto M, et al. Forty-three cases of obturator hernia. Am J Surg. 2004;187:549–552. doi: 10.1016/j.amjsurg.2003.12.041. [DOI] [PubMed] [Google Scholar]
- 8.Nakayama T, Kobayashi S, Shiraishi K, Nishiumi T, Mori S, Isobe K, et al. Diagnosis and treatment of obturator hernia. Keio J Med. 2002;51:129–132. doi: 10.2302/kjm.51.129. [DOI] [PubMed] [Google Scholar]