

Abstract
Congenital diaphragmatic hernias (CDHs) are known to present even after the neonatal period. Posterolateral Bochdalek hernias account for the majority of cases. About 85 % tend to occur on the left side, while the right side accounts for roughly 13 % of the cases. We present a case of a right-sided Bochdalek hernia in an elderly man who was asymptomatic for 60 years of life. The patient presented with vague right upper abdominal discomfort, and ultrasound abdomen revealed herniation of the small bowel into right hemithorax, showing sluggish peristalsis, raising a suspicion of impaired vascularity. He subsequently underwent contrast CT, which confirmed herniation of small bowel loops into right thorax with normal vascularity but dilatation of bowel loops and a possibility of closed-loop obstruction. He was taken up for emergency surgery. The patient had uneventful recovery.
Keywords: Congenital diaphragmatic hernia, Adults, Emergency
Introduction
Congenital diaphragmatic hernias (CDHs) are known to present even after the neonatal period. CDH can be of two types: posterolateral Bochdalek hernia and parasternal Morgagni hernia. The posterolateral hernia is the most common CDH, with an incidence of 1 in 2,000–5,000 live births [1]. About 85 % posterolateral Bochdalek hernias tend to occur on the left side and 15 % on the right side.
Case Report
We present a case of right-sided posterolateral Bochdalek hernia, which presented in an elderly man who was asymptomatic for 60 years of life. The patient presented with breathlessness of a few hours duration, along with periumbilical abdominal pain and a few episodes of vomiting. There was no history of trauma. Chest X-ray and ultrasound of the abdomen revealed herniation of the small bowel into right hemithorax. The herniated loops showed sluggish peristalsis, raising a suspicion of impaired vascularity, on ultrasound. He subsequently underwent contrast CT which revealed herniation of the small bowel into right thorax with normal vascularity but dilatation of bowel loops and a possibility of closed-loop obstruction (Fig. 1). He was taken up for emergency laparotomy, and small bowel loops were seen to herniate into the right thoracic cavity through a posterolateral defect of 3 cm × 2 cm (Fig. 2) on the right side of the diaphragm. There was no hernial sac. Herniated loops were pulled into the abdomen and the loops were found to have normal vascularity. The defect in the diaphragm was sutured with No. 1 Prolene interrupted sutures. The patient had uneventful postoperative recovery.
Fig. 1.

CT Scan showing herniated bowel loops through right hemidiaphragm and fluid in right pleual cavity
Fig. 2.
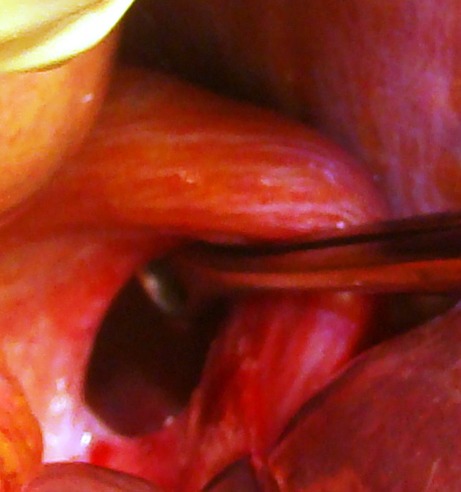
Operative photograph showing the defect in right hemidiaphragm with instrument tip within
Discussion
Although CDH was described by Bochdalek in 1848, the first successful repair in a neonate was not done until 1946 by Gross [2].
The diaphragm forms between 4 and 8 weeks of gestation and divides the celomic cavity into the pleural and peritoneal cavities. Between the eighth and tenth weeks of fetal life, septum transversum and pleuroperitoneal membranes fuse separating the abdominal and thoracic cavities. At about the same time, gastrointestine returns to the abdominal cavity. Herniation of abdominal contents can occur prior to the closure of pleuroperitoneal canal [3]. The central tendon derives from the transverse septum, and the peripheral muscular portion of the diaphragm arises from the posterolateral pleuroperitoneal membranes, which eventually fuse with the transverse septum. Failure of this fusion is the cause of posterolateral diaphragmatic hernia. Because the left side of the diaphragm closes after the right side, most diaphragmatic hernias occur on the left side.
The defects can vary significantly in size from 1 to 2 cm to complete absence of the hemidiaphragm. Absence of the diaphragm is associated with early symptoms and poor survival. High mortality with CDH is related to the degree of associated pulmonary hypoplasia [4]. Associated congenital malformations such as CHARGE syndrome (C—coloboma, H—heart defects, A—atresia of nasal choana, R—retardation of growth, G—genital and/or other defects, and E—ear difficulties) may be seen [5]. About 85–90 % of CDHs are on the left side, and most of these contain small bowel, spleen, stomach, and colon; occasionally the left lobe of the liver is found in the defect. Right-sided hernias usually contain the right lobe of the liver and intestine, and they sometimes have a delayed presentation. Laparoscopic approach is preferred for repair of these hernias than open methods. Defects less than 5 cm are repaired by Reider technique (interrupted sutures using 2–0 polydioxanone). Those more than 5 cm are repaired by tension-free mesh hernioplasty [6]. A combined approach (laparotomy plus thoracotomy) is preferred for the right-sided Bochdalek hernia to facilitate the replacement of the herniated viscera and to close the diaphragmatic defect to overcome the mass effect of the liver [7].
Mortality in CDH may have an iatrogenic contribution too due to insertion of the intercostal tube when the chest radiograph is misdiagnosed as pleural effusion. In one series, 18 % of cases of CDH were subjected to insertion of intercostal tubes [8].
Conclusion
Diaphragmatic hernias are known to present outside the neonatal age group in only 10 % of cases. Most of the cases who present in the later age group have better prognosis due to lesser degree of pulmonary hypoplasia. Early intervention in this patient helped in smooth postoperative recovery.
References
- 1.Gary EH. Nelson’s textbook of pediatrics. WB Saunders and Co: Philadelphia; 1966. p. 1161. [Google Scholar]
- 2.Gross RE. Congenital hernia of the diaphragm. Am J Dis Child. 1946;71:579–592. doi: 10.1001/archpedi.1946.02020290002001. [DOI] [PubMed] [Google Scholar]
- 3.Kirkland JA. Congenital posterolateral diaphragmatic hernia in the adult. Br J Surg. 1959;47:16–22. doi: 10.1002/bjs.18004720103. [DOI] [PubMed] [Google Scholar]
- 4.Areechon W, Reid L. Hypoplasia of the lung associated with congenital diaphragmatic hernia. Br Med J. 1963;1:230–233. doi: 10.1136/bmj.1.5325.230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Pagon RA, Graham JM, Zonana J, Yong SL. Coloboma, congenital heart disease, and choanal atresia with multiple anomalies: CHARGE association. J Pediatr. 1981;99(2):223–227. doi: 10.1016/S0022-3476(81)80454-4. [DOI] [PubMed] [Google Scholar]
- 6.Kavanagh DO, Ryan RS, Waldron R. Acute dyspnoea due to an incarcerated right-sided Bochdalek’s hernia. Acta Chir Belg. 2008;108:604–606. doi: 10.1080/00015458.2008.11680298. [DOI] [PubMed] [Google Scholar]
- 7.Kumar A, Maheshwari V, Ramakrishnan TS, Sahu S. Caecal perforation with faecal peritonitis—unusual presentation of Bochdalek hernia in an adult: a case report and review of literature. World J Emerg Surg. 2009;4:16. doi: 10.1186/1749-7922-4-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Berman L, Stringer D, Sigmund HE, Shandling B. The late presenting pediatric Bochdalek hernia: a 20 year review. J Pediatr Surg. 1988;23:735–739. doi: 10.1016/S0022-3468(88)80414-7. [DOI] [PubMed] [Google Scholar]