

Abstract
Synovial sarcoma is rare, aggressive, malignant mesenchymal neoplasm. The recent literature does not validate its only prevalence in the extremities of the adult population. Statistics reveal that adult population has the highest prevalence rate; 30 % of reported cases occur in the children and adolescents. It is very rare in pregnancy. Carcinomas may be diagnosed concurrently with pregnancy in approximately 0.1 % of cases, but sarcomas are rare. We report a 21-year-old woman with synovial sarcoma on anterior abdominal wall at 34th week of gestation, which was clinically diagnosed as desmoid tumor. Tumor was totally excised. After 6 months, it relapsed in the form of multiple abdominal wall swellings and ascites.
Keywords: Pregnancy, Synovial sarcoma, Desmoid tumor
Introduction
Synovial sarcoma (SS) is a malignant mesenchymal tumor that usually occurs in close association with joint capsule, tendon sheath, bursae, and fascial structures. It is accepted that synovial sarcoma is derived from primitive mesenchymal cells and it does not arise from the synovial cells. The predominant sites for synovial sarcomas include extremities, head, and neck region, but synovial sarcoma rarely occurs in anterior abdominal wall. The most common age group is second to fifth decade. Synovial sarcomas on histopathology are divided into three subtypes: monophasic, biphasic, and poorly differentiated. Synovial sarcomas are reported rarely in association with pregnancy.
Case Report
A 21-year-old primigravida presented with a history of slowly growing swelling in the anterior abdominal wall for 4 months. Local physical examination revealed a firm swelling in the subcutaneous plane of the anterior abdominal wall. Magnetic resonance imaging revealed a soft tissue mass attached to the anterior abdominal wall muscles without metastasis and it was diagnosed as desmoid tumor. Routine laboratory investigations were within normal limits. Fine-needle aspiration cytology from the lesion revealed a spindle cell tumor and biopsy was advised for the confirmation of diagnosis. Subsequently, the patient underwent a total excision of the mass.
Gross Examination
The specimen received showed a tumor mass of size 6.5 × 5 × 3 cm. The external surface showed nodularity. It was sharply circumscribed and invested by smooth glistening pseudocapsule. Cut surface of the tumor was solid, yellowish, fleshy, and glistening without areas of hemorrhages and necrosis (Fig. 1).
Fig. 1.

Solid, yellowish, fleshy, and glistening tumor mass
Microscopic Examination
The tumor predominantly shows crowded spindle cells in a wavy, short fascicular pattern along with pseudoglandular formation containing amorphous eosinophilic periodic acid-Schiff + secretions. Mitotic activities are 2/10 high-power field (Fig. 2).
Fig. 2.
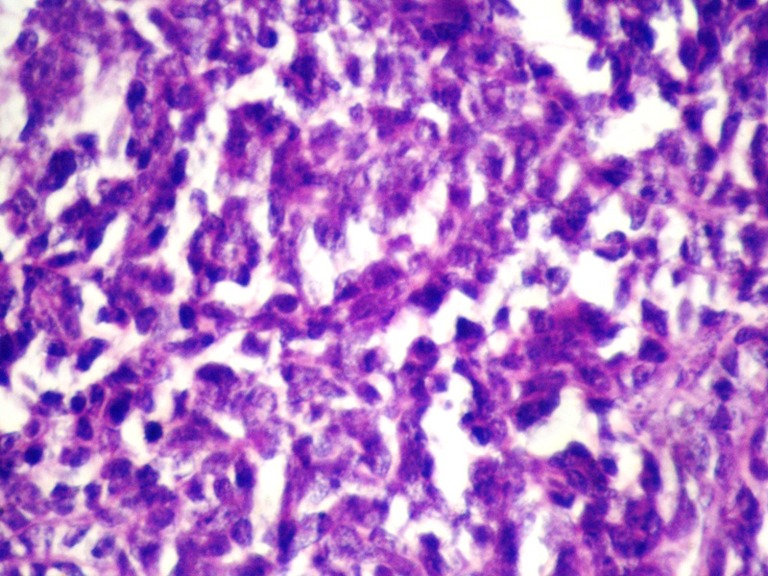
Biphasic pattern
Immunohistochemistry
Tumor cells were positive for cytokeratin, epithelial membrane antigen, Mic-2, and bcl-2 and immunonegative for calponin.
A pathological diagnosis of biphasic synovial sarcoma was made. The patient was postoperatively advised for local irradiation and chemotherapy. Patient denied the further line of treatment. After 6 months, she presented with local recurrence of tumor in the form of multiple anterior abdominal wall swellings with ascites. The patient refused to take treatment and took discharge against medical advice; hence, further follow-up was not possible.
Discussion
Abdominal wall sarcomas are quite rare with only 44 cases having been reported between 1950 and 2005 [1]. Isolated case reports are available showing presence of synovial sarcoma in the subcutaneous area or anterior abdominal wall or presentation as lipoma [2–4]. Al-Jubran et al. in 2005 studied 14 cases of bone and soft tissue sarcomas in pregnancy, but they did not find a case of synovial sarcoma [5]. Merimsky et al. in 1998 studied seven soft tissue and bone sarcomas in association with pregnancy, but there was not a single case of synovial sarcoma [6]. Jafari et al. in 1978 presented six cases of synovial sarcoma during pregnancy, but none of it was in the abdominal wall [7]. This proves the rarity of this case. Most studies reported desmoid tumor as the most common anterior abdominal wall tumor [8].
On microscopic examination, SS is divided into monophasic, biphasic, and poorly differentiated subtypes. The present case was of biphasic type. The prognostic factors for SS patients are divided into two groups: low- and high-risk groups. A low-risk group (patient age <25 years, tumor size <5 cm, and no histological evidence of poorly differentiated tumor) has 88 % disease-free survival and high-risk group (age of patient >25 years, tumor size >5 cm, and poorly differentiated tumor) has 18 % disease-free survival [9, 10]. In our case, tumor size proved to be the most important factor for recurrence.
Conclusion
A 21-year-old primigravida presented with an anterior abdominal wall tumor. It was clinically and cytologically diagnosed as desmoid tumor. The diagnosis of synovial sarcoma was not considered by clinician as well as by cytologist because of its rarity at this site and its rare concurrent occurrence with pregnancy. Therefore, while cytology in such presentations is reported, a possibility of synovial sarcoma should always be kept in mind and biopsy should be made mandatory to facilitate the treatment modality. A lesson that we learned from this case is that “all abdominal wall neoplasms are not desmoid tumor and sarcoma must always be considered in differential diagnosis.”
Footnotes
The article is submitted to the journal for first time and was not presented or submitted prior.
References
- 1.McNeill J, Nguyen YV. Synovial sarcoma of the abdominal wall. Radiol Case Rep [Online] 2007;2:108. doi: 10.2484/rcr.v2i4.108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Eduardo M, Enrique M. Synovial sarcoma of anterior abdominal wall. Ann Surg. 1968;168(5):928–930. doi: 10.1097/00000658-196811000-00023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Louis G, Jean B, Francoise B, et al. Histological grade but not SYT-SSX fusion type: an important prognostic factor in patients with synovial sarcoma. J Clin Oncol. 2004;22:4040–4050. doi: 10.1200/JCO.2004.11.093. [DOI] [PubMed] [Google Scholar]
- 4.Ismet O, Aslaner A (2005) Synovial sarcoma of anterior abdominal wall. Int J Surg 7 (1). http://www.ispub.com/journal/the-internet-journal-of-surgery/volume-7-number-1/synovial-sarcoma-on-the-anterior-abdominal-wall.html#sthash.hKvtXLfa.dpbs. Accessed 29 Dec 2012
- 5.Al-Jubran A, Abdel Salam M, El-Weshi A, et al. Bone and soft tissue sarcomas during pregnancy. J Clin Oncol. 2005;23:9077. [Google Scholar]
- 6.Merimsky O, Le Cesne A. Soft tissue and bone sarcomas in association with pregnancy. Acta Oncol. 1998;37:721–722. doi: 10.1080/028418698430106. [DOI] [PubMed] [Google Scholar]
- 7.Jafari K, Lash AF, Webster A. Pregnancy and sarcoma. Acta Obstet Gynecol Scand. 1978;57(3):265–271. doi: 10.3109/00016347809154896. [DOI] [PubMed] [Google Scholar]
- 8.Stojadinovic A, Hoos A, Karpoff HM, et al. Soft tissue tumor of abdominal wall. Arch Surg. 2001;136:70–79. doi: 10.1001/archsurg.136.1.70. [DOI] [PubMed] [Google Scholar]
- 9.Hasegawa T, et al. Prognostic significance of histologic grade and nuclear expression of beta catenin in synovial sarcoma. Hum Pathol. 2001;32:257–263. doi: 10.1053/hupa.2001.22764. [DOI] [PubMed] [Google Scholar]
- 10.Bergh P, Meis-Kindblom JM, et al. Synovial sarcoma: identification of low and high risk groups. Cancer. 1999;12:2596–2607. doi: 10.1002/(SICI)1097-0142(19990615)85:12<2596::AID-CNCR16>3.0.CO;2-K. [DOI] [PubMed] [Google Scholar]