

Abstract
Large retroperitoneal liposarcomas represent a unique situation and require a more aggressive surgical approach, including multiple resections for recurrences. We report a series of 5 cases of large retroperitoneal liposarcoma managed aggressively with surgical resection. All cases presented with lump and abdominal pain and diagnosis was established by Ultrasonography and CT scan. Post-operative course was uneventful and a median follow up of 3 years, all patients were free from recurrence.
Keywords: Retroperitoneal liposarcoma
Introduction
Retroperitoneal liposarcomas are rare malignant tumors, but are commonest among the soft tissue sarcomas. Primary retroperitoneal tumors are reported to account for 0.16% of all malignancies, and 10–20% of all primary retroperitoneal tumors are liposarcomas. At present, no etiological factors are known for the pathogenesis of liposarcomas.
Case 1
A 21-year-old male; a retroperitoneal tumor weighing about 7 kg was removed. Figures 1 and 2.
Fig. 1.

A CT scan showing a heterogeneous mass in the retroperitoneal space, containing hyperdense area suggestive of blood
Fig. 2.

Intraoperative photograph of a 7-kg retroperitoneal tumor with impending rupture, measuring 40 × 30 × 25 cm
Case 2
A 70-year-old male; right kidney was displaced to the left and lay anterior to the vertebral column. Mass was firm in consistency with smooth surface. Figures 3 and 4.
Fig. 3.

A CT scan showing a heterogeneous mass measuring about 30 × 22 × 12 cm in the retroperitoneal space with multiple areas of necrosis
Fig. 4.

Intraoperative photograph of a 9.3-kg retroperitoneal tumor, measuring 33 × 25 × 15 cm
Case 3
A 48-year-old male; operated thrice for retroperitoneal tumor. At the fourth exploration multiple tumor masses were removed. Figures 5, 6 and 7.
Fig. 5.

A CT scan of the abdomen showing multiple heterogeneous lesions arising from retroperitoneum
Fig. 6.
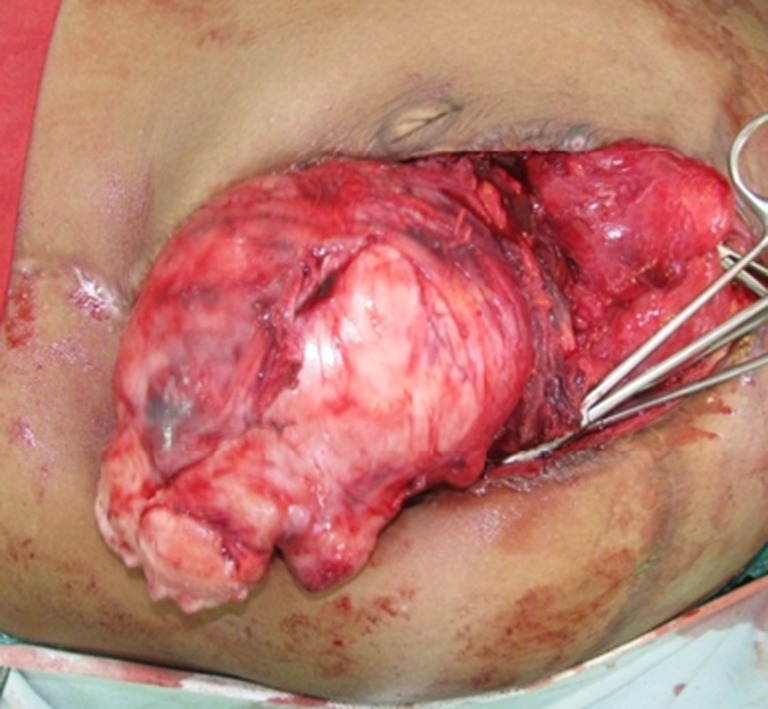
Intraoperative photograph of a 3-kg retroperitoneal tumor mass, measuring 20 × 12 × 10 cm
Fig. 7.
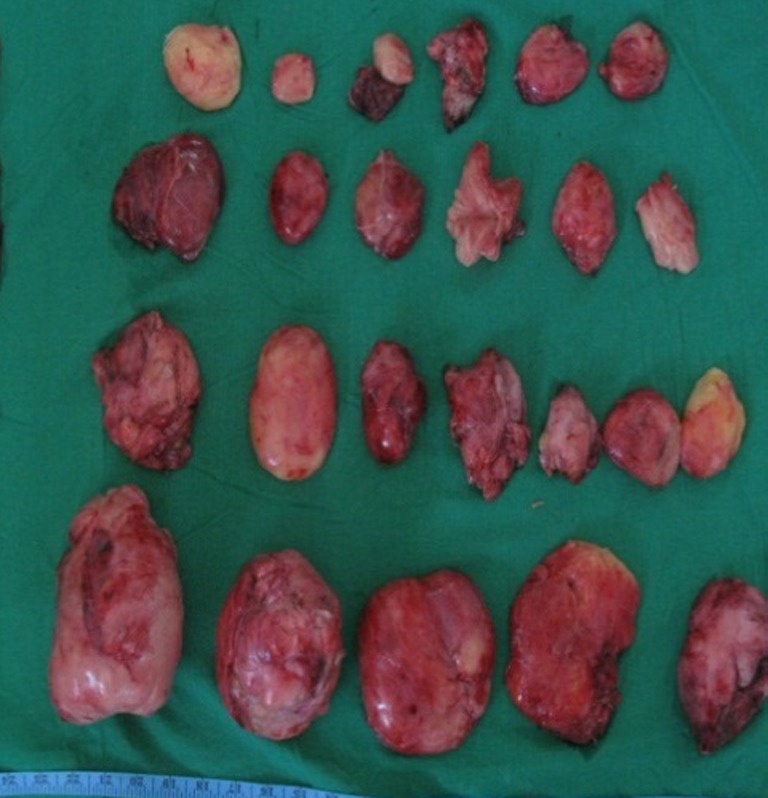
Multiple excised masses of a retroperitoneal liposarcoma collectively weighing about 3.5 kg
Case 4
A 65-year-old male; impression was large mixed density lesion with fat component and calcification representing teratoma. Histopathological examination revealed pleomorphic liposarcoma. The patient had a recurrence 5 years later in 2010. He was reexplored and all the masses were removed en-bloc. Figures 8, 9, 10 and 11.
Fig. 8.

A CT scan of the abdomen (2005) showing large density lesion with fat component and calcification representing teratoma
Fig. 9.

Excised mass of a large retroperitoneal liposarcoma in 2005 (weight 8.2 kg)
Fig. 10.

A CT scan (2010) showing recurrent well-defined, huge, hypodense solid mass measuring 18 × 15 × 15 cm
Fig. 11.

Large recurrent 4.3-kg retroperitoneal sarcoma, measuring 20 × 15 × 15 cm (2010)
Case 5
A 34-year-old male; on examination, he was found to have a large well-circumscribed, firm lump. Figures 12 and 13.
Fig. 12.

A CT scan showing a large predominantly hypodense mass measuring about 20 × 10 × 10 cm arising from retroperitoneum
Fig. 13.
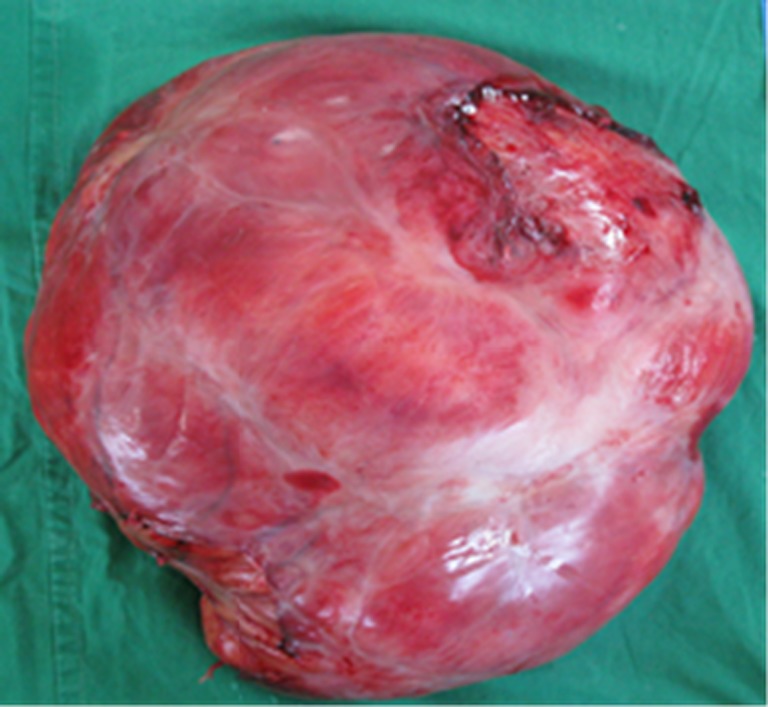
Specimen of a large retroperitoneal mass measuring 20 × 15 × 15 cm (weight 5.1 kg)
Discussion
Retroperitoneal liposarcoma is a malignant tumor of mesenchymal origin. It is one of the most common primary retroperitoneal neoplasms and affects middle-aged patients. The most-common presenting symptom is a palpable abdominal mass, followed by a vague abdominal pain [1]. However, liposarcomas rarely involve the gastrointestinal tract [2–4].
The gross appearance of the tumor depends on the histological type, degree of vascularity, presence of necrosis, and amount of mature fat and fibrous tissue. The tumor appears as a smooth, lobulated, or nodular mass in most instances. Recurrent tumors are not as well encapsulated.
The primary treatment option is resection, if possible [5, 6]. In our series, we followed the approach of the radical resection of the tumor instead of enucleation, assuming that we had to deal with a retroperitoneal tumor of an unknown pathology. However, local recurrence is common and occurs in 66% of patients. This has prompted the investigation of new combined-modality treatment approaches [7]. The most important prognostic factors are free margins, type of resection, age of the patient, and tumor histology.
Radiotherapy (RT) is indicated when the margins are not adequate or there is residual tumor or recurrence. RT is generally used as adjuvant treatment for palliation [8] and may also be applied in higher-grade, locally advanced retroperitoneal liposarcoma. Multi-institutional prospective randomized phase III trial (ACOSOG-Z9031) assessing the value of preoperative RT in patients with primary retroperitoneal soft tissue sarcoma is ongoing. Primary objective of this study is to find out whether preoperative RT will prolong survival without disease relapse. Little data are available for the use of combined RT and chemotherapy (CT). Decisions about adjuvant or neoadjuvant CT or RT are left to clinical judgment [9–11].
A metastatic disease is hematogenous and the extent of metastases is related to the histological grade of the tumor. Local recurrence is the rule with all cell types and invariably with well-differentiated liposarcoma and its variants. Overall, 5-year survival rates are 60–70%. Excision followed by RT (60–70 Gy) results in a more significant reduction in local recurrence than does excision alone [12]. CT has not shown substantial benefits [13]. Myxoid/round cell liposarcoma is highly radio- and chemosensitive. It is selectively responsive to novel drugs, such as trabectedin, a DNA-binding agent. Differentiation between the subtypes of liposarcoma is important to indicate prognosis and, especially, to tailor treatment [14, 15].
Long-term results of two prospective trials showed favorable 5-year local recurrence-free (60%), disease-free (46%), and overall survival rates (61%) among patients who had complete oncological clearance (R0) or incomplete oncological clearance (R1) resection after preoperative RT for intermediate or high-grade retroperitoneal sarcoma [16].
Recent advances have focused on oncogenesis and genomic profiling to identify subsets of liposarcoma, which follow separate molecular pathways. A well-differentiated liposarcoma has 12q rings and giant markers (chromosomal alteration), and the involved genes are HMGIC, CDK4, and MDM2 amplification with a frequency of >90% [17, 18]. The morphology of retroperitoneal liposarcoma has also been studied using optical coherence tomography. These could help in the future to evolve optimal treatment strategies [19–21].
Contributor Information
Rajeev M. Joshi, Email: rajeevjoshi50@gmail.com
Gautum K. Gangurde, Email: gautamgangurde13@gmail.com
Nikhil P. Talathi, Email: nikhiltalathi@yahoo.co.in
Parag P. Telavane, Email: paragt84@yahoo.co.in
Rajinder Singh, Email: drrajinder@gmail.com.
Satish R. Hanamshetti, Email: drsatishrh@gmail.com
Devbrata R. Adhikari, Phone: +91-22-23531401, Email: docdev84@yahoo.com
References
- 1.Brennan NF, Casper ES, Harrison LB (1997) Soft tissue sarcoma. In: De Vita V (ed) Cancer principles and practice of oncology. pp 1738–1788
- 2.Chaudhary A, Arora R, Sharma A, Aggarwal S, Safaya R, Sharma S. Primary colonic liposarcoma causing colo-colic intusussception: a case report and review of literature. J Gastrointest Cancer. 2007;38:160–163. doi: 10.1007/s12029-008-9031-1. [DOI] [PubMed] [Google Scholar]
- 3.Shahidzadeh R, Ponce CR, Lee JR, Chamberlain SM. Liposarcoma in a colonic polyp: case report and review of the literature. Dig Dis Sci. 2007;52:3377–3380. doi: 10.1007/s10620-007-9806-4. [DOI] [PubMed] [Google Scholar]
- 4.Jarboui S, Moussi A, Jarraya H, Ben Mna K, Abdesselem MM, Kourda A, BenJilani S, Guettier C, Zaouche A. Primary dedifferentiated liposarcoma of the colon: a case report. Gastroenterol Clin Biol. 2009;33:1016–1018. doi: 10.1016/j.gcb.2008.11.014. [DOI] [PubMed] [Google Scholar]
- 5.Schwarzbach MH, Hohenberger P. Current concepts in the management of retroperitoneal soft tissue sarcoma. Recent Results Cancer Res. 2009;179:301–319. doi: 10.1007/978-3-540-77960-5_19. [DOI] [PubMed] [Google Scholar]
- 6.Ferrario T, Karakousis CP. Retroperoperitoneal sarcomas. Arch Surg. 2003;138:248–251. doi: 10.1001/archsurg.138.3.248. [DOI] [PubMed] [Google Scholar]
- 7.Raut CP, Pisters PWT. Retroperitoneal Sarcomas: combined-modality treatment approaches. J Surg Oncol. 2006;94:81–87. doi: 10.1002/jso.20543. [DOI] [PubMed] [Google Scholar]
- 8.Tzeng CW, Fiveash JB, Heslin MJ. Radiation therapy for retroperitoneal sarcoma. Expert Rev Anticancer Ther. 2006;6(8):1251–1260. doi: 10.1586/14737140.6.8.1251. [DOI] [PubMed] [Google Scholar]
- 9.Mendenhall WM, Zlotecki RA, Hochwald SN, Hemming AW, Grobmyer SR, Cance WG. Retroperitoneal soft tissue sarcoma. Cancer. 2005;104(4):669–675. doi: 10.1002/cncr.21264. [DOI] [PubMed] [Google Scholar]
- 10.Windham CT, Pisters PWT. Retroperitoneal sarcomas. Cancer Control. 2005;12(1):36–43. doi: 10.1177/107327480501200105. [DOI] [PubMed] [Google Scholar]
- 11.Pawlik TM, Pisters PW, Mikula L, Feig BW, Hunt KK, Cormier JN, et al. Long-term results of two prospective trials of preoperative external beam radiotherapy for localized intermediate- or high-grade retroperitoneal soft tissue sarcoma. Ann Surg Oncol. 2006;13(4):508–517. doi: 10.1245/ASO.2006.05.035. [DOI] [PubMed] [Google Scholar]
- 12.Hohenberger P, Allenberg JR, Schlag PM, Reichardt P. Results of surgery and multimodal therapy for patients with soft tissue sarcoma invading to vascular structures. Cancer. 1999;85(2):396–408. doi: 10.1002/(SICI)1097-0142(19990115)85:2<396::AID-CNCR18>3.0.CO;2-O. [DOI] [PubMed] [Google Scholar]
- 13.Hassan I, Park SZ, Donohue JH, Nagorney DM, Kay PA, Nasciemento AG, et al. Operative management of primary retroperitoneal sarcomas. A reappraisal of an institute experience. Ann Surg. 2004;239:244–250. doi: 10.1097/01.sla.0000108670.31446.54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Jones RL, Fisher C, Al-Muderis O, Judson IR. Differential sensitivity of liposarcoma subtypes to chemotherapy. Eur J Cancer. 2005;41:2853–2860. doi: 10.1016/j.ejca.2005.07.023. [DOI] [PubMed] [Google Scholar]
- 15.Engstrom K, Bergh P, Cederlund CG. Irradiation of myxoid/round cell liposarcoma induces volume reduction and lipoma-like morphology. Acta Oncol. 2007;46:838–845. doi: 10.1080/02841860601080415. [DOI] [PubMed] [Google Scholar]
- 16.Singer S, Corson JM, Demetri GD, Healey EA, Marcus K, Eberlein TJ. Prognostic factors predictive of survival for truncal and retroperitoneal soft-tissue sarcoma. Ann Surg. 1995;221:185–195. doi: 10.1097/00000658-199502000-00009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Heim S, Mandahl N, Dristoffersson U. Marker ring chromosome- a new cytogenetic abnormality characterizing lipogenetic tumors? Cancer Genet Cytogenet. 1987;24(2):319. doi: 10.1016/0165-4608(87)90114-2. [DOI] [PubMed] [Google Scholar]
- 18.Rosai J, Akerman M, dal Cin P. Combined morphologic and karyotypic study of 59 atypical lipomatous tumors. Evaluation of their relationship and differential diagnosis with other adipose tissue tumors. Am J Surg Pathol. 1996;20(10):1182. doi: 10.1097/00000478-199610000-00002. [DOI] [PubMed] [Google Scholar]
- 19.de Vreeze RS, de Jong D, Koops W, Nederlof PM, Ariaens A, Haas RL, van Coevorden F. Oncogenesis and classification of mixed-type liposarcoma: a radiological, histopathological and molecular biological analysis. Int J Cancer. 2011;128(4):778–786. doi: 10.1002/ijc.25390. [DOI] [PubMed] [Google Scholar]
- 20.Rieker RJ, Weitz J, Lehner B, Egerer G, Mueller A, Kasper B, Schirmacher P, Joos S, Mechtersheimer G. Genomic profiling reveals subsets of dedifferentiated liposarcoma to follow separate molecular pathways. Virchows Arch. 2010;456(3):277–285. doi: 10.1007/s00428-009-0869-9. [DOI] [PubMed] [Google Scholar]
- 21.Carbajal EF, Baranov SA, Manne VG, Young ED, Lazar AJ, Lev DC, Pollock RE, Larin KV. Revealing retroperitoneal liposarcoma morphology using optical coherence tomography. J Biomed Opt. 2011;16(2):020502. doi: 10.1117/1.3541789. [DOI] [PubMed] [Google Scholar]