

Abstract
Acute gastric dilatation with infarction, necrosis, and perforation is a rare event. Here, we are presenting the case of a 16-year-old girl who presented to the surgical emergency with vomiting, acute pain in the abdomen, and distension of abdomen. X-ray abdomen showed gas under the diaphragm and massively dilated gastric shadow. Emergency laparotomy was done in which massive dilatation of the stomach with necrosis and perforation was found. Total gastrectomy with esophagojejunostomy was performed and the patient survived.
Keywords: Stomach, Gastric necrosis
Case Report
A 16-year-old girl was admitted to the emergency department with a history of intense pain in the abdomen with severe vomiting and acute abdominal distension for the past 8–10 h. Physical examination showed that the patient was in shock and blood pressure was unrecordable, with a feeble pulse rate of 160/min and a respiratory rate of 30/min. The abdomen was distended and rigid with involuntary guarding. Bowel sounds were absent.
The patient was immediately resuscitated with intravenous fluids and high-flow oxygen and blood investigations were sent. A wide-bore nasogastric tube was inserted, and immediately 4 l of feculent semisolid fluid was aspirated followed by dark brown blood-stained fluid. Laboratory investigations revealed hemoglobin 10.0 g/dl, hematocrit 26.6 %, white blood cell count 10,500/μl, platelet count 2,62,000/μl, BUN 58 mg/dl, and creatinine 2.4 mg/dl. The serum electrolytes were sodium of 128 mg/dl and potassium of 4.8 mg/dl. Blood gases showed that the patient was in metabolic acidosis with a blood pH of 7.12. Correction for metabolic abnormalities was given accordingly. The patient was of average built with no history of eating disorder or psychiatric disorder, neither any history of previous abdominal surgery or any chronic illness. A plain X-ray abdomen in both erect and supine was done. Features consistent with massive gastric dilatation with free air in the peritoneal cavity were identified (Fig. 1).
Fig. 1.
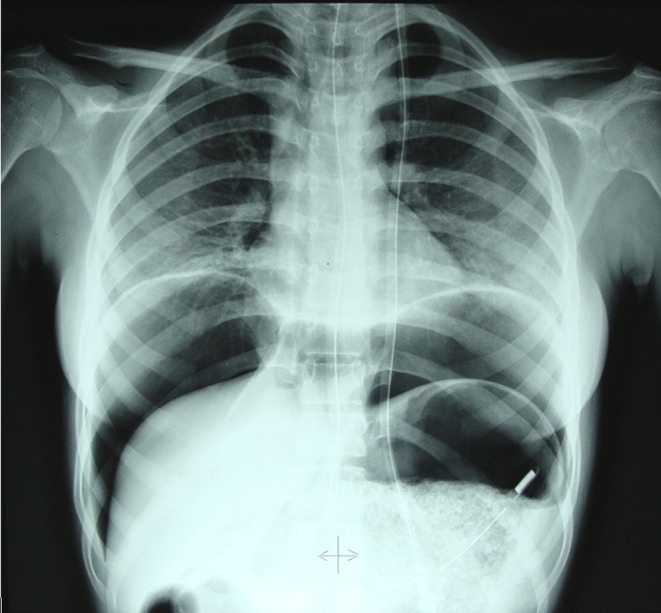
X-Ray abdomen erect film showing pneumoperitoneum in gastric perforation
The patient was taken to the operating room after resuscitation where an emergency total gastrectomy with esophagojejunostomy and feeding jejunostomy were done. The stomach was massively distended extending up to the right iliac fossa, gangrenous along the lesser curvature with a perforation, and patchy areas of necrosis along the fundus and greater curvature. No volvulus or adhesions were seen. Four liters of fluid and undigested food were removed from the peritoneal cavity and stomach. The duodenum and small bowel were normal. The total gastrectomy specimen was massively dilated and gangrenous, measuring approximately 20.6 cm along the lesser curvature and approximately 38.0 cm along the greater curvature. The lesser curvature was gangrenous with a perforation on its anterior aspect (Fig. 2).
Fig. 2.

Specimen of the gangrenous stomach with perforations along the lesser curvature
Histopathological diagnosis showed large areas of mucosal and transmural hemorrhagic infarction with two perforations. The esophageal resected end was viable, while the pyloric resected end was gangrenous. The attached omentum showed congested blood vessels and areas of hemorrhage. Isolated lymph nodes showed caseating granulomatous lymphadenitis suggestive of tuberculosis.
Discussion
Acute gastric dilatation was first described by Duplay in 1833 [1]. The causes of acute gastric dilatation include postoperative conditions, anorexia nervosa and bulimia, psychogenic polyphagia, diabetes mellitus, trauma, electrolyte disturbances, gastric volvulus, spinal conditions, superior mesenteric artery syndrome, medications, infections, debilitating chronic illness, gastric outlet obstruction, aerophagia, and acute pancreatitis [2]. Morris et al. [3] has claimed that anesthesia and debilitation may be predisposing factors. These factors can cause relaxation of the upper esophageal sphincter with aerophagia leading to gastric distention. The atonic theory was introduced in 1859 by Brinton and sustained by others [4]. Revilloid, in 1885, demonstrated that the stomach of cadavers had to be distended with at least 4 l of fluid to result in perforation. In cases of acute massive gastric dilatation, intragastric pressure usually exceeds 30 cm H2O and produces a dramatic decrease of intramural blood flow, with consequent necrosis and perforation [5]. Ischemia initially causes mucosal necrosis followed by full-thickness gastric necrosis which ultimately causes perforation.
Patients with such an acute event require immediate resuscitation due to third-space loss, and immediate laparotomy is usually required.
Contributor Information
Badamutlang Dympep, Phone: +91-989-1440497, Email: badadympep@gmail.com.
Chandra Bhushan Singh, Phone: +91-996-8604382, Email: drcbsingh@sify.com.
Mohd Shakeel, Phone: +91-991-0303136, Email: mdshakeel80@gmail.com.
References
- 1.Saul SH, Dekker A, Watson CG. Acute gastric dilatation with infarction and perforation. Report of fatal outcome in patient with anorexia nervosa. Gut. 1981;22:978–983. doi: 10.1136/gut.22.11.978. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Gul W, Qazi A, Ali SA, Barde C. Acute gastric dilatation in a patient with spinal injury and multiple myeloma. Gastroenterol Hepatol. 2008;4(6):428–434. [PMC free article] [PubMed] [Google Scholar]
- 3.Morris CR, Ivy AC, Maddock WG (1947) Mechanism of acute abdominal distension . Arch Surg 55:101-124 [DOI] [PubMed]
- 4.Abdu RA, Garritano D, Culver O. Acute gastric necrosis in anorexia nervosa and bulimia. Two case reports. Arch Surg. 1987;122(7):830–832. doi: 10.1001/archsurg.1987.01400190096021. [DOI] [PubMed] [Google Scholar]
- 5.Edlich RF, Borner JW, Kuphal J, Wangensteen OH. Gastric blood flow. Its distribution during gastric distention. Am J Surg. 1970;120:35–37. doi: 10.1016/S0002-9610(70)80139-8. [DOI] [PubMed] [Google Scholar]