

Abstract
Objectives.
This study conceptualized loneliness as a mediator in the relation between social engagement and depressive symptoms and explored gender differences in the mediation model. Various indices of social engagement were considered including living arrangement, social network, and activity participation.
Method.
Using data from 674 community-dwelling Korean American older adults, we first examined the mediation effect of loneliness in the relation between each of 3 indices of social engagement (not living alone, social network, and activity participation) and depressive symptoms. Subsequently, gender differences in the mediation model were examined.
Results.
As hypothesized, loneliness was found to mediate the relation between each of the indices of social engagement and depressive symptoms in both men and women. We also observed gender differences in the strength of mediating effects; the effect of living alone was more likely to be mediated by loneliness among men, whereas women showed greater levels of mediation in the models with social network and activity participation.
Discussion.
Our findings suggest that loneliness may explain the mechanism by which deficits in social engagement exerts its effect on depressive symptoms and that gender differences should be considered in interventions targeting social engagement for mental health promotion.
Key Words: Social engagement, Loneliness, Depressive symptoms, Older Korean Americans, Gender differences.
Loneliness is known as one of the “four hardships in old age”  in Asian cultures, along with health constraints, financial difficulties, and boredom. Defined as the subjective evaluation of one’s social condition, loneliness can be distinguished from more objective forms of social isolation such as lack of social contacts, a smaller social network, or lack of social interactions (Cornwell & Waite, 2009). Persistent loneliness is known to be associated with negative outcomes such as poor physical health, impaired sleep, cognitive decline, and psychiatric symptoms including depression (Cacioppo, Hughes, Waite, Hawkley, & Thisted, 2006; Hawkley & Cacioppo, 2010). With as many as 12%–38% of the older population reporting feeling lonely (Theeke, 2009), more information on the role of loneliness in the mechanisms of health and well-being is needed (Hawkley & Cacioppo, 2010).
in Asian cultures, along with health constraints, financial difficulties, and boredom. Defined as the subjective evaluation of one’s social condition, loneliness can be distinguished from more objective forms of social isolation such as lack of social contacts, a smaller social network, or lack of social interactions (Cornwell & Waite, 2009). Persistent loneliness is known to be associated with negative outcomes such as poor physical health, impaired sleep, cognitive decline, and psychiatric symptoms including depression (Cacioppo, Hughes, Waite, Hawkley, & Thisted, 2006; Hawkley & Cacioppo, 2010). With as many as 12%–38% of the older population reporting feeling lonely (Theeke, 2009), more information on the role of loneliness in the mechanisms of health and well-being is needed (Hawkley & Cacioppo, 2010).
Currently ranked as the fifth largest Asian American subgroup, Korean Americans are one of the fastest growing segments of immigrants living in the United States (U.S. Census Bureau, 2011). In the mental health literature, Korean American elders are described as a high-risk group because their rates of probable depression are up to 4 times greater than those of Whites or African Americans (Jang & Chiriboga, 2010; Min, Moon, & Lubben, 2005), and the group reported the highest depressive symptoms among five ethnic groups of Asian Americans in the 2007 California Health Interview Survey (Kim et al., 2010). The direct association of depressive symptoms with limited social activities (Choi, Wilbur, Miller, Szalacha, & McAuley, 2008; Jang & Chiriboga, 2011; Yang et al., 2007) and with loneliness (Kim, 1999) has been reported in previous studies with Korean American elders. However, little is known about the mediating role of loneliness in the relation between social engagement and depressive symptoms, or gender differences.
It is important to study these issues with Korean American older adults not only because they are regarded as being a high-risk group for emotional health problems, but also because they exhibit a higher vulnerability to social isolation due to limited English proficiency (Jang, 2010). Cultural values of each ethnic group strongly influence social resources and adaptation patterns (Casado & Sacco, 2012; Knight & Sayegh, 2010; Sayegh & Knight, 2011); understanding group specific patterns in social engagement, loneliness, and depressive symptoms will provide unique insights. For example, cultural values of familism and interdependence embedded in patriarchy and Confucianism of Korean society may translate into gender-specific social roles such as a caregiving role for women and commitment to work for men (Knight & Sayegh, 2010; Wong, Yoo, & Stewart, 2006). Traditional cultural values are retained in older Korean Americans partly because their social interactions tend to be restricted to local Korean ethnic community settings (Wong, Yoo, & Stewart, 2005). It is expected that Korean American older adults have gendered patterns in social participation and mental health similar to those reported in studies with older adults in Korea (Jang et al., 2009; Jeon, Jang, Rhee, Kawachi, & Cho, 2007; Lee, Jang, Lee, Cho, & Park, 2008).
Although the reported lack of social engagement, feelings of loneliness, and depressive symptoms are related, few studies have attempted to explain the mechanisms through which the three constructs affect one another. Evidence suggests that loneliness is a strong predictor of depressive symptoms (Cacioppo et al., 2006; Cacioppo, Hawkley, & Thisted, 2010; Cornwell & Waite, 2009). Using longitudinal samples, for example, Cacioppo and colleagues (2006, 2010) found that feelings of loneliness led to subsequent depression, but not vice versa. On the other hand, although lower levels of social engagement are associated with depressive symptoms, some people may feel lonely while they are socially engaged, whereas some are content without extensive social interactions. It has been suggested that the subjective perception of loneliness may have more impact on depressive symptoms than does the objective situation of social isolation (Cacioppo et al., 2010; Cornwell & Waite, 2009; Fiori, Antonucci, & Cortina, 2006; Hawkley & Cacioppo, 2010). It is possible, indeed, that loneliness may help explain the mechanism through which lack of social engagement presents risks for depressive moods.
Social engagement, broadly defined as “having connections with people and the community,” has been widely linked with health and well-being of older individuals (Park, 2009). Reported benefits of social engagement include decreased rates of mortality (Agahi & Parker, 2008; Maier & Klumb, 2005), reduced functional disability (Buchman et al., 2009; James, Boyle, Buchman, & Bennett, 2011; Mendes de Leon, Glass, & Berkman, 2003), and decreased risk for cognitive impairment (Barnes, Mendes de Leon, Wilson, Bienias, & Evans, 2004; Seeman et al., 2011; Zunzunegui, Alvarado, Del Ser, & Otero, 2003) and depression (Glass, Mendes de Leon, Bassuk, & Berkman, 2006; Hong, Hasche, & Bowland, 2009; Johnson, 1991). As activity theory has suggested, those who continue to participate in activities and engage in social relations in old age seem to be satisfied with their life and maintain good health (Engestrom, 2008; Lemon, Bengtson, & Peterson, 1972; Longino & Kart, 1982).
However, social engagement may not be a universal remedy for everyone because the structure and function of social engagement can manifest itself differently from one person to the next (Cacioppo et al., 2010; Cumming & Henry, 1961; Maier & Klumb, 2005). The construct includes not only structural components of social relationships such as frequency of contacts and size of social networks, but also the content of social activity. Although limited social engagement such as living alone, smaller networks of family and friends, and lower participation in social activities has generally been linked with poorer mental health outcomes (Hawkley & Cacioppo, 2010; Hawkley, Masi, Berry, & Cacioppo, 2006), specifying the relationship of engagement—or its lack—to loneliness and depressive symptoms could provide insights on the circumstances in which social conditions affect an individual’s depressive symptoms.
Gender differences are of particular interest of this study. Older men and women may differ not only in their levels of social engagement and loneliness, but also in the impact of social engagement on depressive symptoms. For example, older women generally maintain more extensive social ties and a greater participation in social activities compared with older men (Buchman et al., 2009; Hong et al., 2009; James, Wilson, Barnes, & Bennett, 2011; Kendler, Myers, & Prescott, 2005). As much as higher levels of social engagement may be beneficial to older women (Agahi & Parker, 2008), however, there is evidence that older women are more sensitive to the lack of social support than men, and more likely to report loneliness (Aartsen & Jylhä, 2011; Ekwall, Sivberg, & Hallberg, 2005; Kendler et al., 2005; Pinquart & Sorensen, 2001). Although evidence suggests possible gender differences in the role of loneliness in the relation between social engagement and depressive symptoms, to our knowledge, the hypothesis has not been explicitly tested.
Based on previous literature, this study is designed to address three research questions.
(1) Are there gender differences in the levels of social engagement? We hypothesize that older Korean American men will show lower levels of social engagement than older Korean American women on measures of social network and activity participation, but will be less likely to live alone.
(2) Are the impacts of social engagement on depressive symptoms mediated by loneliness in both men and women? We hypothesize that the mediating effects will be observed in both men and women.
(3) Are there gender differences in the magnitudes of mediation effects? Due to the lack of literature on this issue, the final research question is explorative in its nature and no specific hypothesis is specified.
Method
Participants
Upon approval from the university Institutional Review Board, surveys with community-dwelling Korean older adults (aged 60 or older) were conducted from March to August 2008 in Tampa and Orlando, FL. Several sampling methods were combined to recruit immigrant populations. These methods included contacting local Korean churches, other religious groups, senior centers, senior housing, and elder associations. To recruit individuals who were not affiliated with those groups or organizations, referrals from respondents as well as other individuals associated with the primary data collection sites were requested. This convenience sampling procedure was supplemented with a systematic approach using a telephone directory of Korean residents provided by the Florida Korean American Association, which included a total of 2,000 Korean residents in Tampa and Orlando areas, and were called to ask whether there were age-eligible members in their household. Up to five phone calls were made until the individual was considered unreachable. If there was an eligible person in the household, a mail survey packet was sent. This step was designed to improve comprehensiveness of the sample by including individuals who were not recruited by the convenience sampling method and to offset limitations associated with nonrepresentativeness of convenience sampling.
A total of 674 participants were included in the final sample. Detailed information on sampling procedures and validation of the strategy of using multiple methods for recruitment is available elsewhere (Jang, Chiriboga, Allen, Kwak, & Haley, 2010). All respondents were paid US$20 for their participation. The survey questionnaires were in Korean and were developed through back-translation and pilot-testing with 20 older Korean adults who were representative of the anticipated sample. In places where visits were made, surveys were self-administered but trained Korean-speaking interviewers were available for those needing assistance. A copy of the questionnaire and a self-addressed, stamped return envelope were mailed to all individuals with whom onsite contacts were not possible.
Measures
Social engagement.—Three social engagement-related variables were used. The first variable, living arrangement, focuses on the structural component of social engagement. Response to a single question on living arrangement was coded into “living alone” (0) or “living with others” (1). The second variable was social network consisting of family and friends networks, which was adapted from Social Network Scale of Lubben (1988). Three items focused on family, including the number of relatives seen at least once a month (six categories ranging from 0 to 9 or more), frequency of contact (six categories ranging from less than monthly to daily), and the number of relatives the participant felt close to (six categories ranging from 0 to 9 or more). Three identical questions were asked about friends. These six items were summed, with the resulting scale having internal consistency of .79. The third variable focuses on participation in social activities. Individuals were asked how often they participated in six activities: religious meetings, social gatherings (e.g., elder association, alumni association), senior centers, leisure or sporting activities, volunteer activities, and education/learning activities. Each activity was rated on a 4-point scale, ranging from 0 = never to 3 = every day or almost every day. Internal consistency of the scale was .62; somewhat low internal consistency was expected because the listed activities do not necessarily correlate with each other and the summated scale represents overall activity levels rather than a construct. Responses on each item were combined to yield a composite score.
Loneliness.—The frequency of experiencing feeling lonely was measured with a single item “how often have you felt lonely during the past week?” with a 4-point response set (0 = rarely or none of the time; 1 = some or a little of the time; 2 = occasionally or a moderate amount of time; 3 = most or all of the time). In previous studies, this single item measure of loneliness correlates highly with the 20-item original UCLA scale of loneliness (Russell, Peplau, & Ferguson, 1978) and has been shown to be a valid measure of loneliness (Aartsen & Jylhä, 2011; Theeke, 2009).
Depressive symptoms.—The 15-item Geriatric Depression Scale-Short Form (GDS-SF; Sheikh & Yesavage, 1986) was used to measure depressive symptoms. The scale includes 5 positive items (e.g., “Are you satisfied with your life?” and “Do you feel happy?”) and 10 negative items (“Do you feel that your life is empty?” and “Do you feel helpless?”) with a yes/no response format. The total score was calculated by counting the number of endorsed symptoms of depression (scores for positive items were reversed), with the range being from 0 (no depressive symptoms) to 15 (severe depressive symptoms). The GDS-SF has been translated into Korean, and its psychometric properties have been validated (Jang, Small, & Haley, 2001; Mui & Kang, 2006). Internal consistency of the GDS-SF in the present sample was .82.
Background variables.—Demographic information included age (years), gender (0 = men, 1 = women), marital status (0 = married, 1 = not married), and educational attainment (0 = <high school, 1 = ≥high school). Participants were also asked how long they had lived in the United States with responses recoded in years. In addition, participants were asked how they would rate their health, with the response range being poor (1), fair (2), good (3), and excellent (4).
Data Analysis
Descriptive statistics were used to understand sample characteristics, and chi-square or t tests to make comparisons between men and women. The basic mediation model was tested in each gender group (shown in Figure 1) guided by Baron and Kenny’s (1986) criteria: (a) there is a significant association between social engagement and loneliness (path a); (b) there is a significant association between loneliness and depressive symptoms (path b); (c) there is a significant association between a social engagement variable and depressive symptoms (path c); and (d) the association between a social engagement variable and depressive symptoms should become non-significant or weaken when loneliness is controlled for (path c′).
Figure 1.
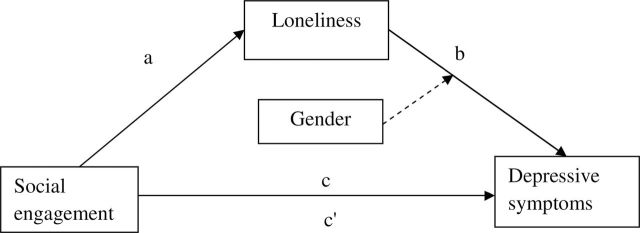
The mediation model of loneliness in the relation between social engagement and depressive symptoms
Note. a = IV to mediator; b = Mediator to DV; c = IV to DV; c′= IV to DV after controlling for the mediating variable.
The final research question on potential gender differences in the magnitude of the mediating effect was tested by following steps for testing the moderated mediation effect or conditional indirect effect (Preacher & Hayes, 2008; Preacher et al., 2007). Of the multiple pathways by which moderated mediation effects can be examined (Preacher et al., 2007), we propose that the moderator (gender) affects paths both from a social engagement variable to loneliness (a in Figure 1) and from loneliness to depressive symptoms (b in Figure 1). The SPSS macros were used for estimating mediation and moderated mediation effects based on a bootstrapping method. The aforementioned method, by repeatedly estimating mediation and moderated mediation effects in each of resampled data sets, approximates the sampling distribution and construct confidence intervals for the mediation and moderated mediation effect (Preacher et al., 2007; Preacher & Hayes, 2008). We computed 95% confidence intervals from 10,000 bootstrap samples. In the mediation models, mediation effects were also confirmed with the Sobel test, a statistical method to assess the significance of any reduction in regression coefficients resulting from mediation (MacKinnon, Lockwood, Hoffman, West, & Sheets, 2002).
Results
Descriptive Information of the Sample
Table 1 presents comparative analysis between men (n = 278) and women (n = 396). The two groups did not differ significantly in length of stay in the United States and loneliness. Men were more likely to be older, have higher levels of education, and rate their health higher compared with women. Regarding social engagement-related variables, men were less likely to live alone and more likely to participate in activities than women. On the other hand, women had larger social networks than men. Finally, women had more depressive symptoms than men. More than 25% of older women fell into the category of probable depression (GDS-SF scores greater than 5), whereas approximately 21% of older men were in the same category (χ2 = 7.56, p < .005). As expected, older Korean women had a larger social network and older Korean men were less likely to be alone; however, contrary to the prediction, men had higher levels of activity participation then women.
Table 1.
Descriptive Characteristics of the Sample (N = 674)
| Variable | M ± SD or % | t/χ2 | |
|---|---|---|---|
| Men (n = 278) | Women (n = 396) | ||
| Socio-demographic | |||
| Age | 71.33±6.36 | 69.37±7.11 | 3.68*** |
| ≥High school | 85.1 | 60.3 | 47.80*** |
| Length of stay in the UnitedStates (years) | 28.98±11.59 | 27.8±11.9 | 1.27 |
| Perceived health | 2.87±0.79 | 2.58±0.84 | 4.66*** |
| Social engagement | |||
| Not living alone | 95.3 | 80.2 | 31.47*** |
| Social network | 21.26±5.96 | 22.77±5.42 | −3.40** |
| Activity participation | 4.98±2.82 | 4.44±2.65 | 2.51* |
| Loneliness | 0.55±0.70 | 0.66±0.74 | −1.91 |
| Depressive symptoms | 3.23±3.25 | 3.87±3.27 | −2.50* |
*p < .05. **p < .01. ***p < .001.
Mediation Analyses
A series of mediation models were tested in each gender group with each of social engagement-related variables, and results are summarized in Table 2. Background variables (age, education, length of stay in the United States, and perceived health) were controlled in all analyses. Similar patterns were observed in separate mediation analyses for men and women. All independent paths among the independent variables (not living alone, social network, and activity participation), the mediator (loneliness), and the dependent variable (depressive symptoms) were significant except the relation between social network and loneliness for men. When loneliness was introduced, the direct significant effects of social engagement-related variables on depressive symptoms became insignificant or significantly reduced. More specifically, all indirect effects were significant for both men and women except for the indirect effect of social network for men. Overall, stronger direct and indirect effects were observed for men with not living alone, and for women with social network and activity participation. The differences of direct and indirect effects between men and women suggest that the mediation model could be moderated by gender, a suggestion that was tested in the subsequent analysis.
Table 2.
Mediation Analyses Between Social Engagement Variables and Depressive Symptoms by Gender
| Not living alone | Social network | Activity participation | ||||
|---|---|---|---|---|---|---|
| Men | Women | Men | Women | Men | Women | |
| IV/loneliness (path a) | ||||||
| B (SE) | −.69 (.20)*** | −.24 (.10)* | −.01 (.01) | −.02 (.01)*** | −.04 (.02)* | −.04 (.01)** |
| Beta | −.21*** | −.12* | −.13 | −.17*** | −.15* | −.14** |
| Loneliness/Depression (path b) | ||||||
| B (SE) | 1.47 (.25)*** | 1.77 (.20)*** | 1.56 (.25)*** | 1.69 (.20)*** | 1.53 (.25)*** | 1.73 (.20)*** |
| Beta | .31*** | .41*** | .33*** | .39*** | .33*** | .40*** |
| IV/Depression (path c) | ||||||
| B (SE) | −3.24 (.86)*** | −1.05 (.40)** | −.08 (.03)* | −.13 (.03)*** | −.16 (.07)* | .23 (.06)*** |
| Beta | −.21*** | −.13** | −.14* | −.22*** | −.14* | −.18*** |
| IV/Depression controlling for loneliness (path c′) | ||||||
| B (SE) | −2.22 (.82)** | −.62 (.36) | −.06 (.03)* | −.09 (.03)** | −.11 (.06) | .16 (.05)** |
| Beta | −.14** | −.08 | −.11* | −.15** | −.10 | −.13** |
| Indirect effect (a × b) with 95% CI | −1.02(−2.27; −.14) | −.43(−.89; −.03) | −.02(−.05;.01) | −.04(−.07; −.02) | −.05(−.10; −.01) | −.07(−.13; −.02) |
| Sobel’s z valuea | −3.10** | −2.46* | −1.59 | −3.18** | −2.18* | −2.70** |
Notes. Notations (a, b, c, and c′) can be found in Figure 1. All analyses were conducted with a control of background variables (age, education, length of stay in the United States, and self-rated health).
Both unstandardized (B) and standardized (Beta) coefficients are presented. It is important to note that unstandardized coefficients are used for testing mediation and moderated mediation models using the bootstrap method and Sobel tests. Because coefficients are standardized within each sample, standardized coefficients may help compare the strengths of effects within sample.
aSobel test was separately conducted to confirm the results from the bootstrapping method.
*p < .05. **p < .01. *p < .001.
The results generally support Hypothesis 2 that loneliness mediated the relationship of social engagement-related variables with depressive symptoms in both men and women.
Gender Differences in Mediation Effects
Since we propose that both paths a and b (Figure 1) are moderated by gender, the quantification of conditional indirect effects includes the components from both paths. In such cases, the moderated mediation can be evaluated based on different conditional indirect effects between groups or moderators (e.g., the magnitude is different between groups; the conditional indirect effect is significant only for one group) using bootstrapping methods (Edwards & Lambert, 2007). The overall mediation effect of loneliness was substantially greater for men (−0.98, p = .006) than for women (−0.44, p = .007) when living alone was the predictor. In contrast, the mediation effects were less for men than women when social network (−0.02, p = .14 vs. −0.04, p = .001) and activity participation (−0.05, p = .037 vs.−0.07, p = .003) were the predictors.
To help interpret overall conditional indirect effects of loneliness on depressive symptoms, Figure 2 illustrates the magnitudes of the mediation relations by gender. The figures show how a one-unit increase in each social engagement variable results in the change in depressive symptoms indirectly through the change in loneliness. For example, the first figure shows that the unit change of living alone (from living alone to not living alone) was associated with a larger decrease in loneliness for men, which indicates that men respond more sensitively than women to the difference in living status in terms of loneliness. The values in depressive symptoms show the changes in depressive symptoms through loneliness affected by the change of the living status. The magnitudes were computed by multiplying the coefficient between the living status and loneliness and the coefficient between loneliness and depression (−0.26 × 1.71 = −0.44 for women; −0.64 × 1.52 = −0.97 for men). As shown, the difference in living alone and not living alone appears to be associated with a larger decrease in depressive symptoms for men than for women. Regarding social network and activity participation in the second and third figures of Figure 2, the scale was magnified by a factor of 20 because the original figure failed to clearly illustrate differences. A one-unit increase in social network or activity participation was associated with a higher decrease of loneliness and a greater decrease of depressive symptoms in women compared with men. As was the case for living alone, the relation between loneliness and depressive symptoms was stronger for women than for men for both cases; the gender difference was negligible for the social network variables.
Figure 2.
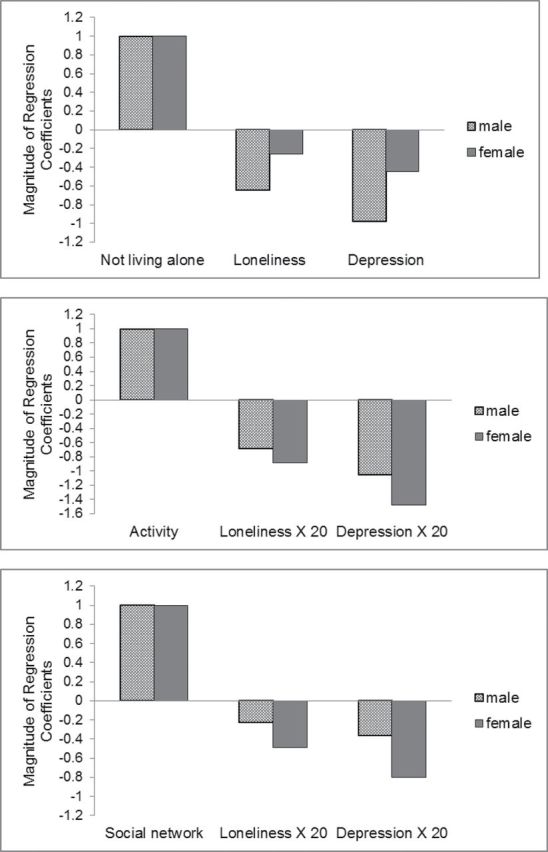
Illustration of the magnitude of mediation by gender
Note. These figures show the change in the magnitude of regression coefficients. The numbers indicate unstandardized regression coefficients. In cases of activity participation and social network, the coefficients were multiplied by 20 for the illustration purpose because the magnitudes of coefficients for loneliness and depressive symptoms were much smaller compared with the magnitudes of coefficients of the independent variables.
Discussion
Our results generally confirmed our hypotheses. As expected, we found that older Korean men were less likely to live alone and have a smaller social network. But contrary to prediction, men engaged in more activities than their female counterparts. As predicted, the relation between each social engagement-related variable and depressive symptoms was mediated by loneliness. We also found interesting gender differences in these mediation effects. The magnitude of mediation effects was different between men and women. For example, loneliness exerted a stronger mediation effect for men in the living alone condition and for women regarding social network and activity participation. This finding implies that different social conditions lead to different influences on older men and women.
The gender differences in mediation relationships are consistent with previous findings, from both overall U.S. and Korean American samples, that social participation is more strongly linked with mental health for older women than for men (Lee et al., 2008). The stronger mediating role of loneliness for women adds to the literature suggesting that limited social engagement has more detrimental effects on women’s mental health (Aartsen & Jylhä, 2011; Ekwall et al., 2005; Kendler et al., 2005; Pinquart & Sorensen, 2001). Similarly, the stronger effect of living alone on mental health for older men has been consistently reported across different cultural groups (Russell, 2009).
On the other hand, the lower level of activity participation among women in our Korean sample is contrary to the greater social participation generally reported among older women (Buchman, 2009; Hong, 2009; Kendler, 2005) and strongly suggests that social role expectations for Korean women deserve greater scrutiny (Chun, Khang, Kim, & Cho, 2008; Jang et al., 2009; Jeon et al., 2007). One factor that may account for the difference is that family plays a central role in Korean culture, and older women assume very high levels of caregiving and family responsibilities in late life, which may limit their opportunities for social participation. Although we have not identified any comparative studies between older Korean and Korean American women with respect to social participation, the cultural values of women’s roles coupled with lack of opportunity for social activities outside of the ethnic enclave may put Korean American older women at a particularly disadvantaged position in social participation.
As suggested earlier, the finding that the mediating effect of loneliness was stronger for men compared with women when living alone is consistent with previous research that living alone exerts more negative effects on men’s mental health than on women’s across different cultural groups (Greenfield & Russell, 2011; Jeon et al., 2007; Russell & Taylor, 2009; Victor et al., 2002). The gender difference might be related to different adaptation patterns in specific social conditions between Korean older men and women. When they live alone, older women tend to compensate their social situation with maintaining more social interactions and social ties with their social networks, whereas older men are less likely to do so (Russell & Taylor, 2009). Yet, the strong association of living alone with heightened depressive symptoms among older Korean American men might be explained by cultural values and social role expectations in Korean society. Korean men are expected to maintain overall responsibility for the well-being of family, yet women provide a caregiving role to their husbands and family (Jeon, 2007). Such emotional dependence on their spouses may lead Korean older men to mental health risks when they are left alone.
It is noteworthy that over half of this sample of older Korean elders reported feeling lonely at least some or a little of the time in the past week. This figure is much higher than the under 20% prevalence of loneliness reported using the same measure of loneliness in a national sample of older populations (Theeke, 2009). Consistent with previous findings (Russell & Taylor, 2009; Shiovitz-Ezra & Leitsch, 2010; Theeke, 2009), perceived poor health was a strong risk factor of loneliness along with living alone, smaller social networks, and lower levels of activity participation. Considering that loneliness has been identified for a risk factor for depressive symptoms (Cacioppo et al., 2006, 2010; Hawkley & Cacioppo, 2010), a special attention should be paid to alleviating loneliness for this population. Interestingly, we found no gender difference in loneliness, but women had more depressive symptoms than men.
Our finding that the effects of social engagement on mental health were not only direct but also indirectly expressed through loneliness, yields important clinical implications. Considering that feeling lonely predicts later depressive symptoms, a simple assessment of one’s feeling of being socially isolated could provide a marker for risk of depressive symptoms. Intervention efforts should target risk groups of individuals such as older men living alone and older women who have smaller social networks and are less likely to participate in activities.
Our study has a number of strengths. This study examined a large sample of older Korean Americans, a group with unique cultural dynamics that might affect social relationships, loneliness, and depression (Jang & Chiriboga, 2011; Jeon et al., 2007). Our project also has some advantages in the measurement of depressive symptoms in research on loneliness. As an item of feeling lonely is embedded in some measures of depressive symptoms such as CES-D (Radloff, 1977), the strong association between loneliness and depressive symptoms reported in past research (r = .40–.65) raises questions about the conceptual distinctions between the two constructs (Cacioppo et al., 2006). Of note, the GDS does not include an item on loneliness, minimizing this concern in our sample. The two constructs are clearly not identical and temporal priority of loneliness over depressive symptoms has been noted in previous studies (Blazer, 2005; Cacioppo et al., 2006, 2010).
The study also had some limitations that should be addressed in future research. First, using a geographically confined sample and including one ethnic sample may limit generalizability of the findings. Yet, the focus on Korean Americans is also strength because our results provide insights relevant to this growing ethnic minority group. Second, this study conceptualizes that loneliness mediates the relationship between social engagement and depressive symptoms. Our cross-sectional findings should be replicated with results from longitudinal studies which could better draw causal inferences. Finally, in this study, social engagement variables focus on structural aspect of social networks and activity participation (e.g., size of and frequency of social contacts). Considering that the quality of social relationships is strongly related with loneliness (Pinquart & Sorensen, 2003), future research should include functional components of social engagement (e.g., actual exchange of social resources between network members or perceived social support) in explaining the mediating role of loneliness in the relation between social engagement and depressive symptoms.
In conclusion, this study describes a potential mechanism through which loneliness mediates the relation between social engagement and depressive symptoms. Although there have been efforts to relate social engagement with depressive symptoms or loneliness with depressive symptoms, little attention has been paid to identify the possibly central role of loneliness in the relationship between social engagement and depressive symptoms. Further, our finding demonstrated that the mediating effect of loneliness was different between men and women. Future research should more closely examine gendered patterns of social engagement, loneliness, and depressive symptoms.
Funding
Data used in this study were collected with support from the National Institute of Mental Health Research Grant Program (R21MH081094; PI—Y. Jang, PhD).
References
- Aartsen M., Jylhä M. (2011). Onset of loneliness in older adults: Results of a 28 year prospective study.. European Journal of Ageing, 8, 31 38. 10.1007/s10433-011-0175-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Agahi N., Parker M. G. (2008). Leisure activities and mortality: Does gender matter? Journal of Aging and Health, 20, 855 871. 10.1177/0898264308324631 [DOI] [PubMed] [Google Scholar]
- Barnes L. L., Mendes de Leon C. F., Wilson R. S., Bienias J. L., Evans D. A. (2004). Social resources and cognitive decline in a population of older African Americans and whites.. Neurology, 63, 2322 2326. 10.1212/01.wnl.0000147473.04043.b3 [DOI] [PubMed] [Google Scholar]
- Baron R. M., Kenny D. A. (1986). The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations.. Journal of personality and social psychology, 51, 1173 1182. 10.1037/0022-3514.51.6.1173 [DOI] [PubMed] [Google Scholar]
- Belsley D. A., Kuh E., Welsch R. E. (1980). Regression diagnostics: Identifying influential data and sources of collinearity New York: John Wiley and Sons, Inc; [Google Scholar]
- Blazer D. G. (2005). Depression and social support in late life: A clear but not obvious relationship.. Aging & Mental Health, 9, 497 499. 10.1080/13607860500294266 [DOI] [PubMed] [Google Scholar]
- Buchman A. S., Boyle P. A., Wilson R. S., Fleischman D. A., Leurgans S., Bennett D. A. (2009). Association between late-life social activity and motor decline in older adults.. Archives of Internal Medicine, 169, 1139 1146. 10.1001/archinternmed.2009.135 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cacioppo J. T., Hawkley L. C., Thisted R. A. (2010). Perceived social isolation makes me sad: 5-year cross-lagged analyses of loneliness and depressive symptomatology in the Chicago Health, Aging, and Social Relations Study.. Psychology and Aging, 25, 453 463. 10.1037/a0017216 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cacioppo J. T., Hughes M. E., Waite L. J., Hawkley L. C., Thisted R. A. (2006). Loneliness as a specific risk factor for depressive symptoms: Cross-sectional and longitudinal analyses.. Psychology and Aging, 21, 140 151. 10.1037/0882-7974.21.1.140 [DOI] [PubMed] [Google Scholar]
- Casado B., Sacco P. (2012). Correlates of caregiver burden among family caregivers of older Korean Americans.. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences, 67, 331 336. 10.1093/geronb/gbr115 [DOI] [PubMed] [Google Scholar]
- Choi J., Wilbur J., Miller A., Szalacha L., McAuley E. (2008). Correlates of leisure-time physical activity in Korean immigrant women.. Western Journal of Nursing Research, 30, 620 638. 10.1177/0193945907310645 [DOI] [PubMed] [Google Scholar]
- Chun H., Khang Y. H., Kim I. H., Cho S. I. (2008). Explaining gender differences in ill-health in South Korea: The roles of socio-structural, psychosocial, and behavioral factors.. Social Science & Medicine (1982), 67, 988 1001. 10.1016/j.socscimed.2008.05.034 [DOI] [PubMed] [Google Scholar]
- Cornwell E. Y., Waite L. J. (2009). Social disconnectedness, perceived isolation, and health among older adults.. Journal of Health and Social Behavior, 50, 31 48. 10.1177/002214650905000103 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cumming E., Henry W. (1961). Growing oldNew York: Basic Books; [Google Scholar]
- Edwards J. R., Lambert L. S. (2007). Methods for integrating moderation and mediation: A general analytical framework using moderated path analysis.. Psychological methods, 12, 1 22. 10.1037/1082-989x.12.1.1 [DOI] [PubMed] [Google Scholar]
- Ekwall A. K., Sivberg B., Hallberg I. R. (2005). Loneliness as a predictor of quality of life among older caregivers.. Journal of Advanced Nursing, 49, 23 32. 10.1111/j.1365-2648.2004.03260.x [DOI] [PubMed] [Google Scholar]
- Engestrom Y. (2008). Discussion: Enriching activity theory without shortcutsInteracting with Computers20(2)256 259. 10.1016/j.intcom.2007.07.003 [Google Scholar]
- Fiori K. L., Antonucci T. C., Cortina K. S. (2006). Social network typologies and mental health among older adults.. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences, 61, P25 P32 [DOI] [PubMed] [Google Scholar]
- Glass T. A., Mendes de Leon C. F., Bassuk S. S., Berkman L. F. (2006). Social engagement and depressive symptoms in late life: Longitudinal findings.. Journal of Aging and Health, 18, 604 628. 10.1177/0898264306291017 [DOI] [PubMed] [Google Scholar]
- Greenfield E. A., Russell D. (2011). Identifying living arrangements that heighten risk for loneliness in later life: Evidence from the U.S. National Social Life, Health, and Aging ProjectJournal of Applied Gerontology30(4)524 534. 10.1177/0733464810364985 [Google Scholar]
- Hawkley L. C., Cacioppo J. T. (2010). Loneliness matters: A theoretical and empirical review of consequences and mechanisms.. Annals of Behavioral Medicine: A Publication of the Society of Behavioral Medicine, 40, 218 227. 10.1007/s12160-010-9210-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hawkley L. C., Masi C. M., Berry J. D., Cacioppo J. T. (2006). Loneliness is a unique predictor of age-related differences in systolic blood pressure.. Psychology and Aging, 21, 152 164. 10.1037/0882-7974.21.1.152 [DOI] [PubMed] [Google Scholar]
- Hong S. I., Hasche L., Bowland S. (2009). Structural relationships between social activities and longitudinal trajectories of depression among older adults.. The Gerontologist, 49, 1 11. 10.1093/geront/gnp006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- James B. D., Boyle P. A., Buchman A. S., Bennett D. A. (2011). Relation of late-life social activity with incident disability among community-dwelling older adults.. The Journals of Gerontology, Series A: Biological Sciences and Medical Sciences, 66, 467 473. 10.1093/gerona/glq231 [DOI] [PMC free article] [PubMed] [Google Scholar]
- James B. D., Wilson R. S., Barnes L. L., Bennett D. A. (2011). Late-life social activity and cognitive decline in old age.. Journal of the International Neuropsychological Society, 17, 998 1005. 10.1017/S1355617711000531 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jang S. N., Kawachi I., Chang J., Boo K., Shin H. G., Lee H., Cho S. I. (2009). Marital status, gender, and depression: Analysis of the baseline survey of the Korean Longitudinal Study of Ageing (KLoSA).. Social science & medicine (1982), 69, 1608 1615. 10.1016/j.socscimed.2009.09.007 [DOI] [PubMed] [Google Scholar]
- Jang Y., Chiriboga D. A. (2010). Living in a different world: Acculturative stress among Korean American elders.. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences, 65B, 14 21. 10.1093/geronb/gbp019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jang Y., Chiriboga D. A. (2011). Social activity and depressive symptoms in Korean American older adults: The conditioning role of acculturation.. Journal of Aging and Health, 23, 767 781. 10.1177/0898264310396214 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jang Y., Chiriboga D. A., Allen J. Y., Kwak J., Haley W. E. (2010). Willingness of older Korean-American adults to use hospice.. Journal of the American Geriatrics Society, 58, 352 356. 10.1111/j.1532-5415.2009.02684.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jang Y., Small B. J., Haley W. E. (2001). Cross-cultural comparability of the Geriatric Depression Scale: Comparison between older Koreans and older Americans.. Aging & Mental Health, 5, 31 37. 10.1080/13607860020020618 [DOI] [PubMed] [Google Scholar]
- Jeon G. S., Jang S. N., Rhee S. J., Kawachi I., Cho S. I. (2007). Gender differences in correlates of mental health among elderly Koreans.. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences, 62, S323 S329 [DOI] [PubMed] [Google Scholar]
- Johnson T. P. (1991). Mental health, social relations, and social selection: A longitudinal analysis.. Journal of Health and Social Behavior, 32, 408 423 [PubMed] [Google Scholar]
- Kendler K. S., Myers J., Prescott C. A. (2005). Sex differences in the relationship between social support and risk for major depression: A longitudinal study of opposite-sex twin pairs.. The American Journal of Psychiatry, 162, 250 256. 10.1176/appi.ajp.162.2.250 [DOI] [PubMed] [Google Scholar]
- Kim G., Chiriboga D. A., Jang Y., Lee S., Huang C. H., Parmelee P. (2010). Health status of older Asian Americans in California.. Journal of the American Geriatrics Society, 58, 2003 2008. 10.1111/j.1532-5415.2010.03034.x [DOI] [PubMed] [Google Scholar]
- Kim O. (1999). Predictors of loneliness in elderly Korean immigrant women living in the United States of America.. Journal of Advanced Nursing, 29, 1082 1088. 10.1046/j.1365-2648.1999.00993.x [DOI] [PubMed] [Google Scholar]
- Knight B. G., Sayegh P. (2010). Cultural values and caregiving: The updated sociocultural stress and coping model.. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences, 65B, 5 13. 10.1093/geronb/gbp096 [DOI] [PubMed] [Google Scholar]
- Lee H. Y., Jang S. N., Lee S., Cho S. I., Park E. O. (2008). The relationship between social participation and self-rated health by sex and age: A cross-sectional survey.. International Journal of Nursing Studies, 45, 1042 1054. 10.1016/j.ijnurstu.2007.05.007 [DOI] [PubMed] [Google Scholar]
- Lemon B. W., Bengtson V. L., Peterson J. A. (1972). An exploration of the activity theory of aging: Activity types and life satisfaction among in-movers to a retirement community.. Journal of Gerontology, 27, 511 523. 10.1093/geronj/27.4.511 [DOI] [PubMed] [Google Scholar]
- Longino C. F., Jr, Kart C. S. (1982). Explicating activity theory: A formal replication.. Journal of Gerontology, 37, 713 722. 10.1093/geronj/37.6.713 [DOI] [PubMed] [Google Scholar]
- Lubben J. E. (1988). Assessing social networks among elderly populationsFamily & Community Health11(3)42 52 [Google Scholar]
- MacKinnon D. P., Lockwood C. M., Hoffman J. M., West S. G., Sheets V. (2002). A comparison of methods to test mediation and other intervening variable effects.. Psychological Methods, 7, 83 104. 10.1037/1082-989X.7.1.83 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maier H., Klumb P. L. (2005). Social participation and survival at older ages: Is the effect driven by activity content or context? European Journal of Ageing, 2(1)31 39. 10.1007/s10433-005-0018-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mendes de Leon C., Glass T. A., Berkman L. F. (2003). Social engagement and disability in a community population of older adultsAmerican Journal of Epidemiology157(7)633 642. 10.1093/aje/kwg028 [DOI] [PubMed] [Google Scholar]
- Min J. W., Moon A., Lubben J. E. (2005). Determinants of psychological distress over time among older Korean immigrants and Non-Hispanic White elders: Evidence from a two-wave panel study.. Aging & Mental Health, 9, 210 222. 10.1080/13607860500090011 [DOI] [PubMed] [Google Scholar]
- Mui A. C., Kang S. Y. (2006). Acculturation stress and depression among Asian immigrant elders.. Social Work, 51, 243 255. 10.1093/sw/51.3.243 [DOI] [PubMed] [Google Scholar]
- Park N. S. (2009). The relationship of social engagement to psychological well-being of residents in assisted living facilitiesJournal of Applied Gerontology28(4)461 481. 10.1177/0733464808328606 [Google Scholar]
- Pinquart M., Sorensen S. (2001). Influences on loneliness in older adults: A meta-analysisBasic and Applied Social Psychology23(4)245 266. 10.1207/s15324834basp2304_2 [Google Scholar]
- Pinquart M., Sorensen S. (2003). Risk factors for loneliness in adulthood and old age: A meta analysis. In Shohov S. (Ed.), Advances in psychology research (Vol. 19, pp. 111 143). Hauppauge, NY: Nova Science Publishers; [Google Scholar]
- Preacher K. J., Hayes A. F. (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models.. Behavior Research Methods, 40, 879 891. 10.3758/BRM.40.3.879 [DOI] [PubMed] [Google Scholar]
- Preacher K. J., Rucker D. D., Hayes A. F. (2007). Addressing moderated mediation hypotheses: Theory, methods, and prescriptionsMultivariate Behavioral Research42(1)185 227. 10.1080/00273170701341316 [DOI] [PubMed] [Google Scholar]
- Radloff L. (1977). The CES-D scale: A self-report depression scale for research in the general populationApplied Psychological Measurement1, 385 401. 10.1177/014662167700100306 [Google Scholar]
- Russell D., Peplau L. A., Ferguson M. L. (1978). Developing a measure of loneliness.. Journal of Personality Assessment, 42, 290 294. 10.1207/s15327752jpa4203_11 [DOI] [PubMed] [Google Scholar]
- Russell D., Taylor J. (2009). Living alone and depressive symptoms: The influence of gender, physical disability, and social support among Hispanic and non-Hispanic older adults.. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences, 64, 95 104. 10.1093/geronb/gbn002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sayegh P., Knight B. G. (2011). The effects of familism and cultural justification on the mental and physical health of family caregivers.. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences, 66, 3 14. 10.1093/geronb/gbq061 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seeman T. E., Miller-Martinez D. M., Stein Merkin S., Lachman M. E., Tun P. A., Karlamangla A. S. (2011). Histories of social engagement and adult cognition: Midlife in the U.S. study.. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences, 66(Suppl. 1)i141 i152. 10.1093/geronb/gbq091 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sheikh J. I., Yesavage J. A. (1986). Geriatric Depression Scale (GDS): Recent evidence and development of a shorter versionClinical Gerontologist5, 165 17310.1300/J018v05n01_09 [Google Scholar]
- Shiovitz-Ezra S., Leitsch S. A. (2010). The Role of social relationships in predicting loneliness: The National Social Life, Health, and Aging ProjectSocial Work Research34(3)157 167. 10.1093/swr/34.3.157 [Google Scholar]
- Theeke L. A. (2009). Predictors of loneliness in U.S. adults over age sixty-five.. Archives of psychiatric nursing, 23, 387 396. 10.1016/j.apnu.2008.11.002 [DOI] [PubMed] [Google Scholar]
- U.S. Census Bureau (2011). 2010 Census American fact finder. Retrieved from http://factfinder.census.gov
- Victor C. R., Scambler S. J., Shah S., Cook D. G., Harris T., Rink E., de Wilde S. (2002). Has loneliness amongst older people increased? An investigation into variations between cohortsAgeing & Society22(5)585 597. 10.1017/S0144686X02008784 [Google Scholar]
- Wong S. T., Yoo G. J., Stewart A. L. (2005). Examining the types of social support and the actual sources of support in older Chinese and Korean immigrants.. International Journal of Aging & Human Development, 61, 105 121 [DOI] [PubMed] [Google Scholar]
- Wong S. T., Yoo G. J., Stewart A. L. (2006). The changing meaning of family support among older Chinese and Korean immigrants.. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences, 61, S4 S9 [DOI] [PubMed] [Google Scholar]
- Yang K., Laffrey S. C., Stuifbergen A., Im E. O., May K., Kouzekanani K. (2007). Leisure-time physical activity among midlife Korean immigrant women in the US.. Journal of Immigrant and Minority Health/Center for Minority Public Health, 9, 291 298. 10.1007/s10903-007-9039-9 [DOI] [PubMed] [Google Scholar]
- Zunzunegui M. V., Alvarado B. E., Del Ser T., Otero A. (2003). Social networks, social integration, and social engagement determine cognitive decline in community-dwelling Spanish older adults.. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences, 58, S93 S100. 10.1093/geronb/58.2.S93 [DOI] [PMC free article] [PubMed] [Google Scholar]