

Abstract
Risk-taking behavior involves making choices with uncertain positive or negative outcomes. Evidence suggests that risk-taking behavior is influenced by emotional state. One such emotional experience is social anxiety, which has been related to both risk-avoidant and risk-seeking decision making. The present study examined a community sample of 34 adolescents grouped into low (Low SA Group) and high (High SA Group) social anxiety (SA). Both groups were compared on changes in performance on a risk taking task (Balloon Analogue Risk Task) between a social threat condition (modified Trier Social Stress Test, High Stress) and a control condition (Low Stress). These conditions were administered on different days, and the order was counterbalanced across subjects. A group x condition interaction revealed that the High SA Group showed greater risk-taking behavior when exposed to the High Stress Condition compared to the Low Stress Condition, while the Low SA Group evidenced no difference between the two conditions. Conceivable interpretations for the increased risk behavior under the condition of social stress for those high in social anxiety are discussed as well as implications for understanding the complex relationship between social anxiety and risk behavior.
Keywords: Risk-taking behavior, social anxiety, adolescent, in-vivo anxiety manipulation
1. Introduction
Risk-taking behavior involves making choices with uncertain positive or negative outcomes, and consists of balancing potential harm or danger to the individual with potential achievement or reward (Byrnes, Miller, and Schafer, 1999; Leigh, 1999). Risk taking is clearly linked to some clinical conditions including substance dependence and abuse as well as borderline and antisocial personality disorders (American Psychiatric Association, 2000). However, the relationship between risk taking and other conditions is less clear, with social anxiety (and the clinical diagnosis of social phobia) exhibiting a particularly complicated picture.
There has been a significant effort aimed at understanding the relationship between social anxiety and risk taking. The literature shows that social anxiety is associated with risk-avoidant decision-making (Barlow, 1988; Butler & Mathews, 1987); including research indicating that individuals high in trait social anxiety make risk-avoidant decisions on a risk-taking behavioral task (Maner et al., 2007). Yet, other work suggests that social anxiety is related to risk-prone activities, including aggression, unsafe sexual practices, and novelty seeking in response to impulsive decision-making (Erwin, Heimberg, Schneier, & Liebowitz, 2003; Kachin, Newman, & Pincus, 2001; Kashdan, Collins, & Elhai, 2006; Kashdan, Elhai, & Breen, 2008; Kashdan & Hofmann, 2008). For example, social anxiety is positively correlated with drinking in situations involving unpleasant emotions and conflict with others (e.g., Buckner Eggleston, & Schmidt, 2006). The seemingly opposing findings related to the association of social anxiety with both risk-avoidant as well as risk-prone decision-making may be related to the context in which the decision-making takes place.
The presence of stress or a highly distressing situation is known to influence the type of decisions that individuals make (e.g., Loewenstein, Weber, Hsee, & Welch, 2001). For example, evidence suggests that risk-taking behavior is influenced by negative affective states such as fear, disgust, or anger (e.g., Lerner & Keltner, 2000; 2001). It is conceivable that social anxiety is associated with risk-avoidance in low emotion contexts, but with risk-seeking in high emotion contexts. Based on limited cognitive resource theories (e.g., Eysenck, Derakshan, Santos, & Calvo, 2007), it may be that under conditions of stress, cognitive resources are recruited for emotion regulation, and diverted away from the inhibitory processes that are necessary to inhibit risky behavior, resulting in more risk taking (e.g., Baumeister, Vohs, & Tice, 2007; Richards, 2004). An alternative mechanism is that engagement in risky behavior serves as a form of negative reinforcement (i.e., Baker, Piper, McCarthy, Majeskie, & Fiore, 2004), such that risk engagement reduces distress associated with the social anxiety.
Few studies have examined the relationship between social anxiety and risk-taking behavior in adolescents; the majority of studies have included college-aged and up participants (see Hardin et al., 2009 and Myers, Aarons, Tomlinson, & Stein, 2003 for exceptions). The issue of enhanced risk-taking in typically developing adolescents, combined with the peak onset of anxiety disorders during this period (Grant, et al., 2005; Johnston, O’Malley, Bachman, & Schulenberg, 2011), highlights the need to study the effects of anxiety on risk-taking in adolescents specifically. Social anxiety is particularly relevant to adolescence because of the dramatic social re-orientation from family to peers (e.g., Nelson et al., 2005) and the exacerbated sensitivity to social expectation and evaluation that take place during this period (Allen, Porter, McFarland, Marsh, & McElhaney, 2005; Guyer, Choate, Pine, & Nelson, 2011). Adolescence is also associated with a dramatic increase in the onset of substance use (e.g., Windle et al., 2008), delinquency (Moffitt, Caspi, Harrington, & Milne, & 2002), and other potentially health-compromising behaviors (DiClemente, Hansen, & Ponton, 1996; Smith-Khuri et al., 2004). Earlier age of risk behavior onset can often predict poorer health and emotional outcomes in adulthood (e.g., Brook, Adams, & Balka, 2004; Colman, Wadsworth, Croudace, Jones, 2007; Sourander et al., 2007). The possibility that socially anxious adolescents, who in neutral situations would tend to be risk-aversive, could become risk-takers in a stressful situation warrants investigation.
Building upon prior research, this study sought to examine the effect of a social stressor on risky decision-making in adolescents with varying degrees of social anxiety. To this aim, we compared low- to high-socially anxious adolescents on their risk-taking behavior using the Balloon Analogue Risk Task (BART) under high and low stress conditions, using a modified Trier Social Stress Test. We hypothesized that high socially anxious (High SA) adolescents would show increased risk-taking when experiencing social stress (compared to a low stress or neutral situation), while low socially anxious (Low SA) adolescents would not exhibit changes in their risk-taking across these two conditions.
2. Method
2.1 Subjects
This study employed data from a sample of adolescents, 15 to 18 years old, recruited from the greater metropolitan Washington D.C. area. These adolescents participated in a larger research project on how adolescents handle stressful situations and had signed a permission to be informed about additional research participant opportunities. To be eligible for the study, participants had to be between the ages of 15 and 18 and be proficient in English. Thirty-nine participants were recruited for the study, three attended only the initial session and two others did not complete the behavioral task at one of their sessions; one participant included did not complete a self-report rating (modified Positive Affect/Negative Affect Scale (PANAS)) and was not included in the analyses including this variable. Of the final 34 participants (67.6% female) included in the analysis, the mean age was 16.07 (SD = 1.01, range = 15–18). The sample was 26.5% Non-Hispanic White, 55.9% Black/African-American, 2.9% Native American, 2.9% Asian American, and 11.8% multiple or other race.
2.2 Measures
We measured stress level by using the four most relevant negative affect items from the Positive Affect/Negative Affect Scale (PANAS; Watson, Clark, & Tellegen, 1988), including “upset,” “angry,” “frustrated”, and “anxious.” For both pre- and post-induction stress assessment, subjects rated the frequency and the intensity of each emotion they were experiencing on a 5-point scale, from 1 (never/not at all) to 5 (always/very much). Participants were instructed: “Your responses should reflect how you feel right now, at this moment.” One subject could not be included in this analysis because of missing pre-stress data.
The Abbreviated Social Phobia and Anxiety Inventory (SPAI-23; Roberson-Nay, Strong, Nay, Beidel, & Turner, 2007) is a 23-item scale derived from the Social Phobia and Anxiety Inventory (SPAI; Turner, Beidel, Dancu, & Stanley, 1989). The SPAI-23 has a 5-point likert-type scale, ranging from 0 (Never) to 4 (Always). The SPAI-23 has been used in both normal and clinical populations, and highly correlates with the SPAI (r = .88), which has been widely used and has excellent psychometric properties with both adults and adolescents.
Lejuez and colleagues (2002) developed a computerized task, the Balloon Analogue Risk Task (BART), to model risk taking in the laboratory. In a number of studies, BART performance has been significantly related to composites of self-reported “real world” risk behaviors (e.g., substance use, delinquency, and safety behaviors; Lejuez et al., 2002; Lejuez, Aklin, Daughters, Zvolensky, & Kahler, 2007). This measure is well validated in older adolescent samples. An independent review by Harrison, Young, Butow, Salkeld, and Soloman (2005) of the state-of the-art strategies to measure risk taking identified the BART has having excellent reliability and validity. This computerized task can be described as follows (see Figure 1). The computer screen shows a small simulated balloon accompanied by three stimuli: a balloon pump, a reset button labeled “Collect”, and a permanent bank. Each click on the pump inflates the balloon one degree. With each pump, 1 cent is accrued in a temporary reserve. When a balloon is pumped past its individual explosion point, a pop sound emanates from the computer. When a balloon explodes, all cents in the temporary bank are lost and the next un-inflated balloon is shown. At any point during each trial, the subject could stop pumping the balloon and click the Collect button. Clicking this button transfers all cents from the temporary bank to the permanent bank (displayed in Total $$$) incrementally cent by cent with a bells sound. After each balloon explosion or collection, the subject’s exposure to that particular balloon ends and a new balloon appears for a total of 20 balloons (i.e., trials) are. All money earned is paid at the end of each session.
Figure 1.

Schematic of the Balloon Analogue Risk Task.
Standardized instructions were given to each participant prior to beginning the task. Participants were instructed: “Throughout the task, you will be presented with a number of balloons, one at a time. For each balloon you will use the mouse to click on the box that will pump up the balloon. Each click on the mouse pumps up the balloon a little more. You will receive 1 (one) cent per pump. But remember, balloons pop if you pump them up too much. A balloon could pop between 1 and 128 pumps and the average balloon will pop at 64 pumps. At any point, you can stop pumping up the balloon and click on the button labeled “Press to Collect $$$.” Clicking this button will start you on the next balloon and will transfer the accumulated money from your temporary bank to your permanent bank labeled “Total Score.” It is your choice to determine how much to pump up the balloon, but be aware that at some point the balloon will explode. The explosion point varies across balloons, ranging from the first pump to enough pumps to make the balloon fill the entire computer screen. If the balloon explodes before you click on “Collect $$$,” then you move on to the next balloon and any money in your temporary bank is lost. Exploded balloons do not affect the money accumulated in your permanent bank.” The primary dependent measures used were the number of balloon explosions and the number of balloon pumps adjusted for the number of balloons that did not explode (i.e., pumps adjusted average; for more detail on this variable see Lejuez et al., 2002). Although the two variables are related, the number of explosions may be viewed as more directly linked to the consequences of risky behavior and therefore of particular relevance to the current study.
2.3 Procedure
Permission to conduct research was obtained from the University of Maryland Institutional Review Board (IRB). Participants signed an informed assent and one parent/guardian signed an informed consent. Participants who were 18 years of age signed a consent form. Participants came for two sessions, separated by 3 to 14 days. Each session corresponded to one of 2 conditions (Low versus High Stress). The order of these conditions was randomized across subjects.
In the High Stress condition (see Figure 2), each participant 1) was given a baseline stress rating to complete (i.e., the modified PANAS), 2) was exposed to the Speech induction (see below for details), 3) was given the stress rating to complete, 4) completed the BART, and 5) gave a speech. In the Low Stress condition each participant 1) was given instruction about a rest period following BART administration, 2) was given a stress rating to complete1, 3) completed the BART, and 4) had a rest period.
Figure 2.
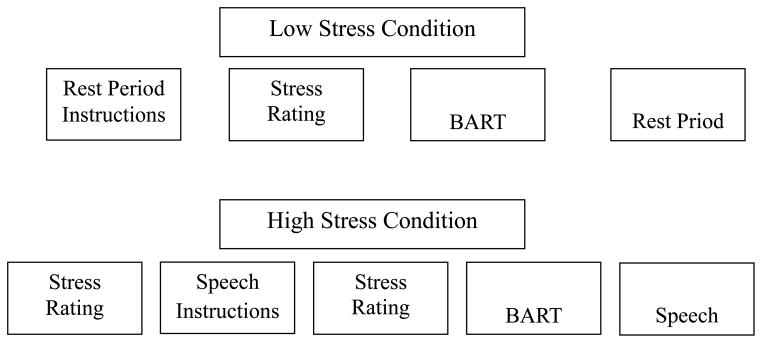
Schematic of events for the High Stress Condition.
The High Stress Condition was adapted from the Trier Social Stress Test (TSST; Kirschbaum, Pirke, & Hellhammer 1993) and video anxiety induction procedures (Tovilović, Novović, Mihić, & Jovanović, 2009). In the High Stress Condition, following the baseline assessment of stress, participants were presented several short videos, each showing a college student presenting a speech in front of an audience of professors. In the videos, while the professors take notes and ask stern questions, the student exhibits increasingly anxious behaviors (e.g., stumbling over words, blushing, sweating). Following the video, participants were told that they will take part in a similar situation at the end of the session in front of a similar audience of judges. For their speech, participants were informed that they would be provided with three speech topics. The same three speech topics were given to all participants. The topics were: 1) should girls be allowed to play on boys’ sports teams? 2) what does Barack Obama’s presidency say about race relations in the United States, and 3) what is one value that’s important to you and how have you consistently lived your life according to it? Participants were informed that one of the topics would be randomly selected by the researcher at the end of the session for them to present an improvised 3 minute speech, and if they did not fulfill the three minute block, the judges would ask them questions, such as “From what source did you gather your information and how do you know it applies to this topic?” until the three minute period was completed. Participants were told that, just as in the video, they would deliver their speech in front of one to five judges. Moreover, participants were provided a list of criteria that included vocabulary, speech fluidity, and enunciation to be used by the judges. Following the speech instructions, the stress rating was completed. Next, the BART was administered. The speech itself was completed after the BART, but it is notable that it was not part of the analysis plan and no data were collected during the speech. The session ended after the speech was completed.
As noted above, the Low Stress Condition involved a rest period of three minutes at the end of the session. Specifically, participants sat in a comfortable chair quietly without distraction. As with the speech, no data were collected during the rest period.
Participants were reimbursed for time and effort at each session including a base payment of $20 plus all earnings on the task which ranged from $0–$13, resulting in a total possible range between $40 and $66.
2.4 Analytic Plan
Preliminary analyses examined the impact of the stress manipulation and explored potential covariates. Primary analyses focused on BART explosions and adjusted average pumps. For these primary analyses, participants were grouped according to low and high scores on the SPAI-23. Participants scoring below and up to the median of 19 were characterized as low socially anxious (Low SA Group; n = 18; 52.9%, SPAI-23 scores ranged from 0–19, M = 9.39, SD = 7.23), while participants scoring above this median score of 19 were characterized as high socially anxious (High SA Group; n = 16; 47.1%, SPAI-23 scores ranged from 20–38, M = 25.75, SD = 4.42). Notably, this median score of 19 is comparable to the mean SPAI-23 score in 4 large studies with older adolescents (means ranging from 16–19) suggesting the appropriateness of the cutoff used here (Schry, Roberson-Nay, & White, 2012). 25.1% of the High SA group fell above the suggested clinical threshold (Schry et al., 2012)
3. Results
3.1 Preliminary Analyses
SA group did not differ on any of the demographic variables (see Table 1). Examination of correlations revealed that no demographic variable was related to the primary dependent variable of change in BART score from the low stress and high stress sessions. In addition, the order in which sessions were completed was not related to the primary dependent variable. As such, these variables were not utilized in the analyses reported below.
Table 1.
Descriptive Statistics and Examination of Differences between Conditions at the Baseline Session
| Variable | Total Sample (n = 34) | Low SA (n = 18) | High SA (n = 16) | t/χ2 | p |
|---|---|---|---|---|---|
| Age (M(SD)) | 16.07 (1.01) | 15.79 (0.81) | 16.38 (1.15) | 1.75 | .09 |
| Gender (% Female) | 67.6 | 72.2 | 62.5 | 0.37 | .55 |
| Race (% Black) | 55.9 | 66.7 | 43.8 | 5.60 | .20 |
| SPAI-23 (M(SD)) | 17.09 (10.23) | 9.39 (7.25) | 25.75 (4.42) | 7.82 | <.001 |
Note. SA = Social Anxiety, SPAI-23 = Abbreviated Social Phobia and Anxiety Inventory.
3.2 Manipulation Check
The effect of the stress manipulation on the stress rating was examined in the high stress condition using a 2-way repeated measures ANOVA with Group (Low versus High SA) as the between-subject factor and Time (pre-induction, post-induction) as the within-subject factor. As depicted in Figure 3, findings indicated a significant interaction for Group x Time (F(1, 31) = 6.52, p = .016, partial eta2 = .17). Follow-up analyses (individual repeated measures ANOVAs for High and Low SA groups) indicated that stress rating was higher in the post-induction period than in the pre-induction period for the High SA Group (M(SD) = 5.27(1.71) for pre versus 7.07(2.52) for post; F(1, 14) = 17.72, p = .001, d = −0.85) but was not different for the Low SA Group (M(SD) = 4.89(1.32) for pre versus 5.17(1.10) for post; F(1, 17) = .46, p = .51, d = −0.23). Approaching the follow-up analyses from a different angle (employing ANOVA to examine difference in means between the two groups, Low versus High SA, at the pre-induction period and the post induction period), the groups did not differ at the pre-induction period (F(1, 31) = .51, p = .48, d = −0.25), but did differ at the post-induction period (F(1, 31) = 8.37, p = .007, d = −0.98).
Figure 3.

Stress ratings as a function of Social Anxiety Group and Pre/Post Induction in the High Stress Condition.
Main effects also were evident indicating higher stress ratings in the post-induction period compared to the pre-induction period across groups (M(SD) = 5.03(.35) for pre; 6.17(.38) for post; F(1, 31) = 12. 2, p = .001, d = 1.07) and in the High SA Group compared to the Low SA Group across conditions (Low SA M(SD) = 5.06(1.50); High SA M(SD) = 6.03(2.08); F(1, 31) = 4.9, p = .035, d = −0.53).
3.3 BART-Y Findings
As previously stated, the BART-Y was analyzed using both the number of explosions and the adjusted average pumps. For explosions (see Figure 4), an interaction of group (Low versus High SA) by condition (Low versus High Stress) was observed (F(1, 32) = 4.28, p = .047, partial eta2 = .12). Additional analyses were conducted to further explore the nature of this group by condition interaction. Simple effects indicated that the two groups did not significantly differ from each other in the control or experimental condition (p’s > .37). However, differences in explosions were found between the two groups across conditions. The High SA Group showed a higher number of explosions in the High Stress Condition compared to the Low Stress Condition (low-stress M(SD) = 7.0 (2.73); high-stress 8.19 (2.71); F(1, 15) = 5.09, p =.04, d = −0.44), but no difference was found for the Low SA Group (low-stress M(SD) = 7.89 (2.93); high-stress 7.61(3.71); F(1, 17) = .34, p = .57, d = 0.08).
Figure 4.
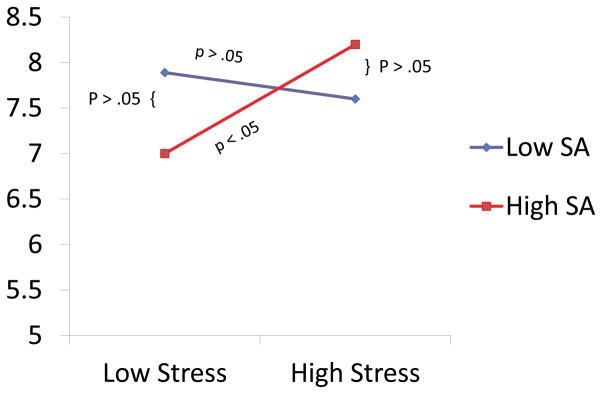
BART explosions as a function of Social Anxiety Group and Stress Condition.
With respect to the pumps adjusted average on BART-Y, the ANOVA revealed no significant interaction or main effects (F(1, 32) = 4.28, p = .27, partial eta2 = .04). Moreover, although the High SA Group showed an increase in adjusted-average pumps from 43.9 to 46.1 pumps across the low and high stress conditions, this difference was not significant. The Low SA Group showed no change in adjusted-average pumps (41.4 in both conditions)2.
Discussion
The present study sought to examine the complex relationship between social anxiety and risk-taking among a sample of healthy adolescents. This study builds upon a complex literature that has found mixed results regarding risk behavior and social anxiety (Hardin et al., 2009; Kashdan, McKnight, Richey, & Hofmann, 2009; Lorian & Grisham, 2010; Maner et al., 2007, Myers et al., 2003). Unlike previous work, this is the first study, to our knowledge, to use a quasi-experimental design to examine this relationship both in and out of the context of a social anxiety induction.
As a first step, our manipulation check showed that the induction was indeed stressful but only to those in the High SA group. With the assurance that our manipulation was working, we also tested the main hypothesis that individuals with higher levels of social anxiety would increase in their risk taking in the context of a social stressor, whereas no such difference would be evident for those with lower levels of social anxiety. Findings were consistent with these hypotheses. Analyses revealed that adolescents in the High SA Group, when acutely socially stressed, increased their risk-taking behavior evidenced by a significant increase in the number of explosions on the BART in the high-stress condition compared to the low-stress condition. Conversely, adolescents in the Low SA group showed no influence of acute social stress on their risk taking on the BART. Of note, although consistent with findings on the explosion variable, findings on the adjusted average pumps were not significant.
The current work represents an initial study establishing the impact of social stress on risk taking of individuals with elevated levels of social anxiety. Although interpretations must be made cautiously, the findings can be understood based on the limited cognitive resource framework (e.g., Dvorak-Bertsch, Curtin, Rubinstein, & Newman, 2007; Green, Rogers, & Elliman, 2000; Pessoa, McKenna, Gutierrez,& Ungerleider, 2002; Tiffany, 1990). Coping with social stress engages cognitive resources to regulate the emotional response to the social stressor, particularly in socially anxious individuals. These cognitive resources, recruited at the service of emotion regulation, would be diverted away from the inhibitory processes that are necessary to inhibit risky behavior. Indeed, evidence shows that emotion regulation is a resource-demanding process, which disrupts simultaneous or subsequent behavioral performance (e.g., Baumeister, Vohs, & Tice, 2007; Richards, 2004). Thus, if an individual needs to regulate their emotional response to stress, then their cognitive resources to inhibit risk-taking become limited.
A related possibility is that engagement in the risk behavior serves as a form of negative reinforcement (i.e., Baker, Piper, McCarthy, Majeskie, & Fiore, 2004) such that risk engagement reduces distress associated with the social anxiety. As such the risk behavior is “negatively reinforced” due to it resulting in the anxiety avoidance/reduction. Self-medication is one specific conceptualization of negative reinforcement that may be particularly relevant here. The most common form of risk behavior noted for those with social anxiety is alcohol and drug use. The use of these substances is thought to regulate mood (Cooper, Frone, Russell, & Mudar, 1995) by ameliorating the impact of acute anxiety (Buckner et al., 2006). Of course increased risk taking on the BART could not result in the type of direct neural effects associated with self-medication as is possible with a substance of abuse, but may still have had some impact in providing the individuals with a strategy for mood regulation or control over behavior in contrast to the stressor where the perception of control may have been violated (Kashdan, Collins, & Elhai, 2006).
Findings should be interpreted in light of the study’s limitations. First, we used a convenience sample, which comprised only a few youths with elevated levels of social anxiety (25.1% of the High SA group, n = 4). Beyond issues associated with generalizability, the limited number of participants with clinically significant symptoms, combined with the overall small sample size, may have undermined our ability to detect less robust effects, such as those measured with the adjusted average pumps variable. Stated differently, perhaps a significant result also could have been found with pumps, as was the case with explosions, with a larger sample size and/or more participants in the clinically relevant range of symptoms. A second limitation concerns the selectivity of the stress procedure that was specific to the social domain. Clearly, the manipulation check validated this social stressor in High SA participants. However, it would be important to know if findings would generalize out of the laboratory setting. Third, future work would benefit from the examination of potential mediators and moderators, such as measures of depressive symptoms or impulsivity or genetic markers, which require the inclusion of a broader range of supporting measures and a larger sample size. One such moderator is outcome expectancies. Kashdan, Collins, and Elhai (2006) demonstrated that socially anxious individuals, expecting positive outcomes in uncertain events, reported strong intentions to engage in risk-taking, whereas socially anxious individuals, expecting negative outcomes, reported weak intentions to engage in risk-taking. In short, the strength of the relationship between social anxiety and risk taking is not only dependent on the social stress per se, but is likely to also be influenced by trait-like cognitive and potentially personality factors. In addition, future research should take into account comorbidities, particularly those defined by problems of inhibitory control (e.g., ADHD), as these comorbidities may lead to even greater risk taking behavior under conditions of stress.
Despite limitations, the findings here are in line with theoretical perspectives on the complex relationship between social anxiety and risk taking. This study significantly extends the literature by moving from examining dispositional levels of anxiety to experimentally manipulated acute social stress. As such, it contributes to the understanding of the functional relationship between social anxiety and risk taking, as well as the contexts that facilitate this relationship. This study sets the stage for future work with more severely impaired clinical samples and ultimately intervention development aimed at inoculating individuals with high social anxiety to identify alternative coping strategies in stressful/risky situations.
Acknowledgments
We would like to thank Stacey B. Daughters for her assistance with participant recruitment and Michael G. Hardin and Katy Korletiz for their support in the design and implementation of the study.
Footnotes
It was our intention in the Low Stress Condition to also provide the stress rating (i.e., modified PANAS) between the baseline and post instructions regarding the rest period following the BART to mirror the High Stress Condition but it was left out of the procedure for about the first 20% of participants. As a result, we chose not to utilize these data here and instead to rely on the difference in the two groups in the High Stress Condition to establish the effect of the manipulation. Further supporting this decision there was no change in the Pre and Post rest period instructions data that were collected for the other 28 participants in Low Stress Condition (p = .91). As such we felt confident that an increase in stress was unique to the High Stress Condition.
Conducting the analyses with SPAI-23 as a median split grouping variable has important benefits in terms of clarity of presentation of the current results. However, we also acknowledge the limitations of a median split approach. To verify that our primary findings were not a specious outcome from a peculiarity in the grouping approach, we also conducted a regression to examine SPAI-23 scores as a continuous variable. Specifically, the predictor variables were SPAI-23 score and Stress condition entered in a first step, followed by the interaction of these two variables in a second step. In doing so, the interactions remained significant for BART explosions (sr2 = .05, p = .046). For adjusted average pumps, the interaction was not significant (sr2 = .03, p = .07). As a result, these additional analyses support the findings provided with the grouping variable as presented above.
Contributor Information
Elizabeth K. Reynolds, Department of Psychiatry and Behavioral Sciences, Division of Child and Adolescent Psychiatry, Johns Hopkins University School of Medicine
Whitney M. Schreiber, Department of Psychology, Center for Addictions, Personality, and Emotions Research, University of Maryland, College Park
Kathy Geisel, Department of Psychology, Center for Addictions, Personality, and Emotions Research, University of Maryland, College Park.
Laura MacPherson, Department of Psychology, Center for Addictions, Personality, and Emotions Research, University of Maryland, College Park.
Monique Ernst, Section on Development and Affective Neuroscience, National Institute of Mental Health;.
C. W. Lejuez, Department of Psychology, Center for Addictions, Personality, and Emotions Research, University of Maryland, College Park
References
- Allen JP, Porter MR, McFarland FC, Marsh P, McElhaney KB. The Two Faces of Adolescents’ Success With Peers: Adolescent Popularity, Social Adaptation, and Deviant Behavior. Child Development. 2005;76(3):747–760. doi: 10.1111/j.1467-8624.2005.00875.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4. Washington, DC: Author; 2000. text rev. [Google Scholar]
- Baker TB, Piper ME, McCarthy DE, Majeskie MR, Fiore MC. Addiction motivation reformulated: An affective processing model of negative reinforcement. Psychological Review. 2004;111:33–51. doi: 10.1037/0033-295X.111.1.33. [DOI] [PubMed] [Google Scholar]
- Barlow DH. Anxiety and its disorders: The nature and treatment of anxiety and panic. New York, NY: Guilford Press; 1988. [Google Scholar]
- Baumeister RF, Vohs KD, Tice DM. The strength model of self-control. Current Directions in Psychological Science. 2007;16(6):351–355. doi: 10.1111/j.1467-8721.2007.00534.x. [DOI] [Google Scholar]
- Brook J, Adams R, Balka E. Illicit drug use and risky sexual behavior among African American and Puerto Rican urban adolescents: The longitudinal links. Journal of Genetic Psychology. 2004;165:203–220. [PubMed] [Google Scholar]
- Buckner JD, Eggleston AM, Schmidt NB. Social Anxiety and Problematic Alcohol Consumption: The Mediating Role of Drinking Motives and Situations. Behavior Therapy. 2006;37(4):381–391. doi: 10.1016/j.beth.2006.02.007. [DOI] [PubMed] [Google Scholar]
- Byrnes JP, Miller DC, Schafer WD. Gender differences in risk taking: A meta-analysis. Psychological Bulletin. 1999;125(3):367–383. doi: 10.1037/0033-2909.125.3.367. [DOI] [Google Scholar]
- Butler G, Mathews A. Anticipatory anxiety and risk perception. Cognitive Therapy and Research. 1987;11(5):551–565. doi: 10.1007/BF01183858. [DOI] [Google Scholar]
- Colman I, Wadsworth ME, Croudace TJ, Jones PB. Forty-year psychiatric outcomes following assessment for internalizing disorder in adolescence. American Journal of Psychiatry. 2007;164:126–133. doi: 10.1176/appi.ajp.164.1.126. [DOI] [PubMed] [Google Scholar]
- Cooper ML, Frone MR, Russell M, Mudar P. Drinking to regulate positive and negative emotions: A motivational model of alcohol use. Journal of Personality and Social Psychology. 1995;69(5):990–1005. doi: 10.1037/0022-3514.69.5.990. [DOI] [PubMed] [Google Scholar]
- DiClemente RJ, Hansen W, Ponton LE. Adolescents at risk: A generation in jeopardy. In: DiClemente R, Hansen W, Ponton L, editors. Handbook of adolescent health risk behavior. New York: Plenum Press; 1996. [Google Scholar]
- Dvorak-Bertsch JD, Curtin JJ, Rubinstein TJ, Newman JP. Anxiety moderates the interplay between cognitive and affective processing. Psychological Science. 2007;18:699–705. doi: 10.1111/j.1467-9280.2007.01963.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Erwin BA, Heimberg RG, Schneier FR, Liebowitz MR. Anger experience and expression in social anxiety disorder: Pretreatment profile and predictors of attrition and response to cognitive-behavioral treatment. Behavior Therapy. 2003;34(3):331–350. doi: 10.1016/S0005-7894(03)80004-7. [DOI] [Google Scholar]
- Eysenck MW, Derakshan N, Santos R, Calvo MG. Anxiety and cognitive performance: attentional control theory. Emotion. 2007;7(2):336–53. doi: 10.1037/1528-3542.7.2.336. [DOI] [PubMed] [Google Scholar]
- Grant BF, Hasin DS, Blanco C, Stinson FS, Chou SP, Goldstein RB, Dawson DA, Smith S, Saha TD, Huang B. The Epidemiology of Social Anxiety Disorder in the United States: Results From the National Epidemiologic Survey on Alcohol and Related Conditions. Journal of Clinical Psychiatry. 2005;66(11):1351–1361. doi: 10.4088/JCP.v66n1102. [DOI] [PubMed] [Google Scholar]
- Green MW, Rogers PJ, Elliman NA. Dietary restraint and addictive behaviors: The generalizability of Tiffany’s cue reactivity model. International Journal of Eating Disorders. 2000;27:419–427. doi: 10.1002/(SICI)1098-108X(200005)27:4<419::AID-EAT6>3.0.CO;2-Z. [DOI] [PubMed] [Google Scholar]
- Guyer AE, Choate VR, Grimm KJ, Pine DS, Keenan K. Emerging depression is associated with face memory deficits in adolescent girls. Journal of the American Academy of Child & Adolescent Psychiatry. 2011;50(2):180–190. doi: 10.1016/j.jaac.2010.11.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hardin MG, Mandell D, Mueller SC, Dahl RE, Pine DS, Ernst M. Inhibitory control in anxious and healthy adolescents is modulated by incentive and incidental affective stimuli. Journal of Child Psychology and Psychiatry. 2009;50(12):1550–1558. doi: 10.1111/j.1469-7610.2009.02121.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Monitoring the Future national results on adolescent drug use: Overview of key findings, 2010. Ann Arbor: Institute for Social Research, The University of Michigan; 2011. p. 77. [Google Scholar]
- Kashdan TB, McKnight PE, Richey JA, Hofmann SG. When social anxiety disorder co-exists with risk-prone, approach behavior: Investigating a neglected, meaningful subset of people in the National Comorbidity Survey-Replication. Behaviour Research and Therapy. 2009;47(7):559–568. doi: 10.1016/j.brat.2009.03.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kachin KE, Newman MG, Pincus AL. An interpersonal problem approach to the division of social phobia subtypes. Behavior Therapy. 2001;32(3):479–501. doi: 10.1016/S0005-7894(01)80032-0. [DOI] [Google Scholar]
- Kashdan TB, Collins RL, Elhai JD. Social Anxiety and Positive Outcome Expectancies on Risk-Taking Behaviors. Cognitive Therapy and Research. 2006;30(6):749–761. doi: 10.1007/s10608-006-9017-x. [DOI] [Google Scholar]
- Kashdan TB, Elhai JD, Breen WE. Social anxiety and disinhibition: An analysis of curiosity and social rank appraisals, approach-avoidance conflicts, and disruptive risk-taking behavior. Journal of Anxiety Disorders. 2008;22(6):925–939. doi: 10.1016/j.janxdis.2007.09.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kashdan TB, Hofmann SG. The high-novelty-seeking, impulsive subtype of generalized social anxiety disorder. Depression and Anxiety. 2008;25(6):535–541. doi: 10.1002/da.20382. [DOI] [PubMed] [Google Scholar]
- Kirschbaum C, Pirke KM, Hellhammer DH. The ‘Trier Social Stress Test’: A tool for investigating psychobiological stress responses in a laboratory setting. Neuropsychobiology. 1993;28(1–2):76–81. doi: 10.1159/000119004. [DOI] [PubMed] [Google Scholar]
- Leigh BC. Peril, chance, adventure: Concepts of risk, alcohol use and risky behavior in young adults. Addiction. 1999;94(3):371–383. doi: 10.1046/j.1360-0443.1999.9433717.x. [DOI] [PubMed] [Google Scholar]
- Lejuez CW, Aklin W, Daughters S, Zvolensky M, Kahler C, Gwadz M. Reliability and Validity of the Youth Version of the Balloon Analogue Risk Task (BART-Y) in the Assessment of Risk-Taking Behavior Among Inner-City Adolescents. Journal of Clinical Child and Adolescent Psychology. 2007;36(1):106–111. doi: 10.1207/s15374424jccp3601_11. [DOI] [PubMed] [Google Scholar]
- Lejuez CW, Read JP, Kahler CW, Richards JB, Ramsey SE, Stuart GL, Strong DR, Brown RA. Evaluation of a behavioral measure of risk taking: The Balloon Analogue Risk Task (BART) Journal of Experimental Psychology: Applied. 2002;8(2):75–84. doi: 10.1037/1076-898X.8.2.75. [DOI] [PubMed] [Google Scholar]
- Lerner JS, Keltner D. Fear, anger, and risk. Journal of Personality and Social Psychology. 2001;81(1):146–159. doi: 10.1037/0022-3514.81.1.146. [DOI] [PubMed] [Google Scholar]
- Lerner JS, Keltner D. Beyond valence: Toward a model of emotion-specific influences on judgement and choice. Cognition and Emotion. 2000;14(4):473–493. doi: 10.1080/026999300402763. [DOI] [Google Scholar]
- Loewenstein GF, Weber EU, Hsee CK, Welch N. Risk as feelings. Psychological Bulletin. 2001;127(2):267–286. doi: 10.1037/0033-2909.127.2.267. [DOI] [PubMed] [Google Scholar]
- Lorian CN, Grisham JR. The safety bias: Risk-avoidance and social anxiety pathology. Behaviour Change. 2010;27(1):29–41. doi: 10.1375/bech.27.1.29. [DOI] [Google Scholar]
- Maner JK, Richey JA, Cromer K, Mallott M, Lejuez CW, Joiner TE, Schmidt NB. Dispositional anxiety and risk-avoidant decision-making. Personality and Individual Differences. 2007;42(4):665–675. doi: 10.1016/j.paid.2006.08.016. [DOI] [Google Scholar]
- Meyers MG, Aarons GA, Tomlinson K, Stein MB. Social anxiety, negative affectivity, and substance use among high school students. Psychology of Addictive Behaviors. 2003;17(4):277–283. doi: 10.1037/0893-164X.17.4.277. [DOI] [PubMed] [Google Scholar]
- Moffit TE, Caspi A, Harrington H, Milne BJ. Males on the life-course-persistent and adolescence-limited antisocial pathways: Follow-up at age 26. Development and Psychopathology. 2002;14:179–206. doi: 10.1017/S0954579402001104. [DOI] [PubMed] [Google Scholar]
- Nelson EE, Leibenluft E, McClure E, Pine DS. The social re-orientation of adolescence: A neuroscience perspective on the process and its relation to psychopathology. Psychological Medicine. 2005;35(2):163–174. doi: 10.1017/S0033291704003915. [DOI] [PubMed] [Google Scholar]
- Pessoa L, McKenna M, Gutierrez E, Ungerleider LG. Neural processing of emotional faces requires attention. Proceedings of the National Academy of Sciences, USA. 2002;98:683–687. doi: 10.1073/pnas.172403899. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Richards JM. The cognitive consequences of concealing feelings. Current Directions in Psychological Science. 2004;13:131–134. doi: 10.1111/j.0963-7214.2004.00291.x. [DOI] [Google Scholar]
- Roberson-Nay R, Strong DR, Nay WT, Beidel DC, Turner SM. Development of an abbreviated Social Phobia and Anxiety Inventory (SPAI) using item response theory: The SPAI-23. Psychological Assessment. 2007;19(1):133–145. doi: 10.1037/1040-3590.19.1.133. [DOI] [PubMed] [Google Scholar]
- Schry AR, Roberson-Nay R, White SW. Measuring Social Anxiety in College Students: A Comprehensive Evaluation of the Psychometric Properties of the SPAI-23. Psychological Assessment. 2012 Feb 27; doi: 10.1037/a0027398. Advance online publication. [DOI] [PubMed] [Google Scholar]
- Smith-Khuri E, Iachan R, Scheidt PC, Overpeck MD, Gabhainn SN, Pickett W, Harrel Y. A cross-national study of violence-related behaviors in adolescents. Archives of Pediatrics & Adolescent Medicine. 2004;158:539–544. doi: 10.1001/archpedi.158.6.539. [DOI] [PubMed] [Google Scholar]
- Sourander A, Jensen P, Davies M, Elonheimo H, Helenius H, Piha J, Kumpulainen K. Who is at greatest risk for adverse long-term outcomes? The Finnish From a Boy to a Man study. Journal of the American Academy of Child & Adolescent Psychiatry. 2007;46:1148–1161. doi: 10.1097/chi.0b013e31809861e9. [DOI] [PubMed] [Google Scholar]
- Tovilović S, Novović Z, Mihić L, Jovanović V. The role of trait anxiety in induction of state anxiety. Psihologija. 2009;42(4):491–504. doi: 10.2298/PSI0904491T. [DOI] [Google Scholar]
- Tiffany ST. A cognitive model of drug urges and drug-use behavior: Role of automatic and nonautomatic processes. Psychological Review. 1990;97:147–168. doi: 10.1037//0033-295X.97.2.147. [DOI] [PubMed] [Google Scholar]
- Turner SM, Beidel DC, Dancu CV, Stanley MA. An empirically derived inventory to measure social fears and anxiety: The Social Phobia and Anxiety Inventory. Psychological Assessment: A Journal of Consulting and Clinical Psychology. 1989;1(1):35–40. doi: 10.1037/1040-3590.1.1.35. [DOI] [Google Scholar]
- Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology. 1988;54(6):1063–1070. doi: 10.1037/0022-3514.54.6.1063. [DOI] [PubMed] [Google Scholar]
- Windle M, Spear LP, Fuligni AJ, Angold A, Brown JD, Pine D, Smith GT, Giedd J, Dahl RE. Transitions into underage and problem drinking: Developmental processes and mechanisms between 10 and 15 years of age. Pediatrics. 2008;121(4):S273–S289. doi: 10.1542/peds.2007-2243C. [DOI] [PMC free article] [PubMed] [Google Scholar]