

Abstract
Both atopy and bronchial hyperresponsiveness (BHR) are characteristic features of asthma. They are also found among non-asthmatic subjects, including allergic rhinitis patients and the general population. Atopy and BHR in asthma are closely related. Atopy induces airway inflammation as an IgE response to a specific allergen, which causes or amplifies BHR. Moreover, significant evidence of the close relationship between atopy and BHR has been found in non-asthmatic subjects. In this article, we discuss the relationship between atopy and BHR in the general population, asthmatic subjects, and those with allergic rhinitis. This should widen our understanding of the pathophysiology of atopy and BHR.
Keywords: Allergic rhinitis, asthma, atopy, bronchial hyperresponsiveness, patients, population
INTRODUCTION
Atopy is defined as an abnormal tendency to produce IgE antibodies in response to common environmental allergens. Although it is not a disease state, it acts as a prerequisite for developing allergic disease, including atopic asthma. Bronchial hyperresponsiveness (BHR) refers to the heightened sensitivity or the excessive reactivity of the airways to a variety of broncho-constricting stimuli. While BHR is one characteristic of asthma, it is also found among non-asthmatic subjects, including subjects with allergic rhinitis (AR) and the general population.
Atopy and BHR in asthma are closely related. Atopy induces airway inflammation as an IgE response to a specific allergen, which induces or amplifies BHR. Moreover, BHR in AR changes according to the exposure to or the avoidance of relevant allergens. Even in the general population, the sensitization rate to common allergens is significantly associated with BHR. In this article, we discuss the relationship between atopy and BHR in the general population, asthmatic subjects, and those with AR, which should widen our understanding of the pathophysiology of atopy and BHR.
ATOPY AND BHR IN THE GENERAL POPULATION
Many studies have reported a close association between atopy and BHR in the general population (Table). BHR is more frequently observed in atopic subjects. The frequency and degree of BHR are associated with the degree of atopy. In a study involving 400 randomly selected college students, the prevalence of BHR was higher in the atopic group than in the non-atopic group, and it increased as the sum of the wheal sizes increased.1 In a large Australian study in which two different dominant allergens (dust mite vs. pollen) were applied to two separate areas, atopic children had a greater risk of BHR at both areas.2 The risk significantly increased when subjects were sensitized to mite and pollen compared to those who were sensitized to either alone. In a study of 527 children aged 7 to 16 years, BHR to histamine showed a good relationship to an atopic index, which was calculated by summing the total wheal sizes from a skin prick test (SPT) to nine common inhalant allergens.3 An independent relationship was reported between the size of the skin test reactions and a bronchial responsiveness index in a multivariate analysis on 662 thirteen-year-old New Zealand children.4 In another study, athletes had a similar relationship between atopy and BHR; atopic athletes had higher BHR than non-atopic athletes, with a tendency for BHR to increase over the number of positive SPTs.5
Table.
Representative studies that show close relationship between atopy and BHR in the general population
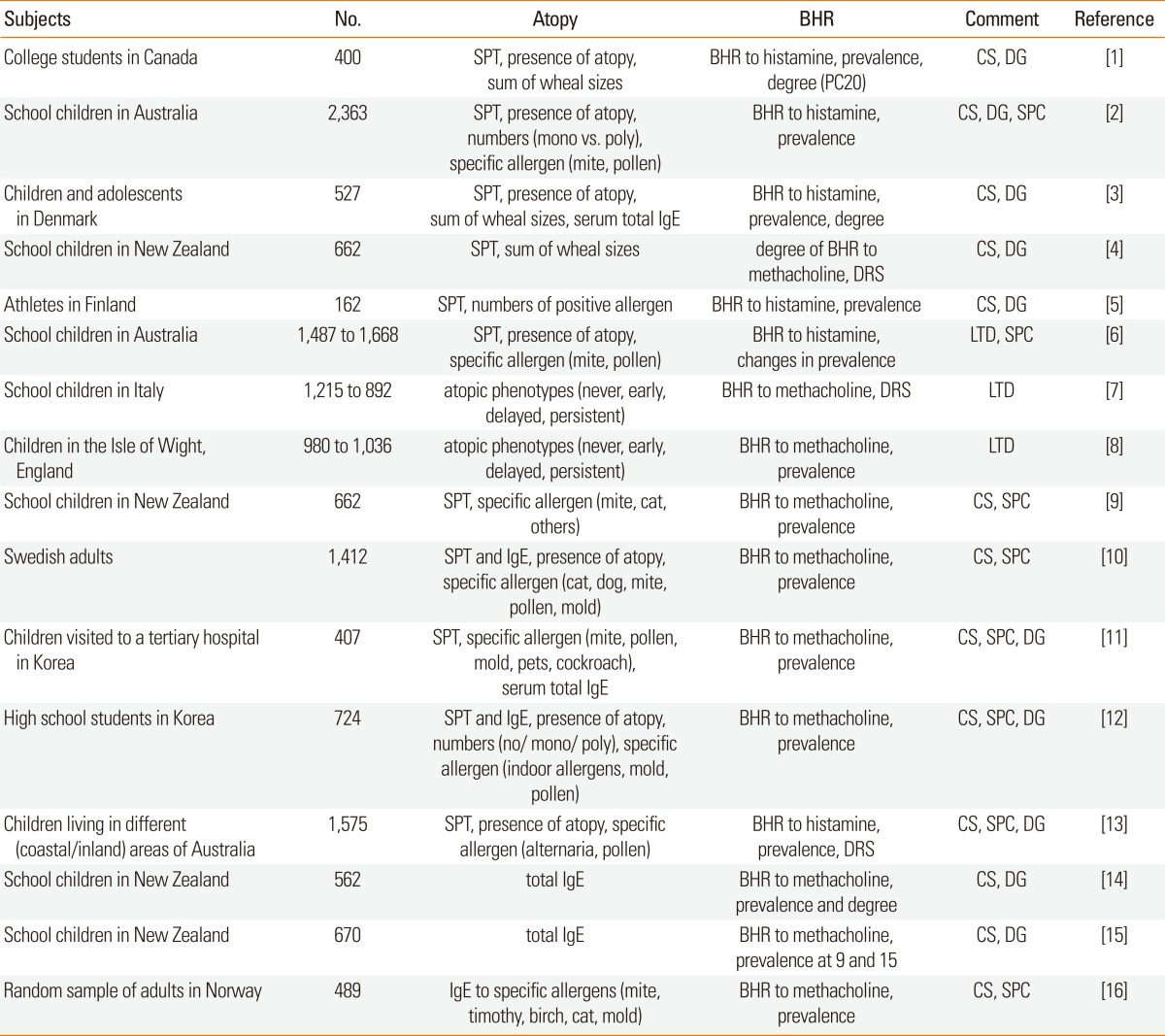
BHR, bronchial hyperresponsiveness; SPT, skin prick test; PC20, provocative concentration that causes 20% fall in forced expiratory volume in 1 second; CS, cross-sectional; DG, degree of atopy; SPC, allergen specificity ; IgE, immunoglobulin E; DRS, dose-response slope; LTD, longitudinal.
Longitudinal studies have also reported a close association between changes in BHR and atopic status. In the aforementioned Australian study, the prevalence of atopy and BHR for 8- to 10-year-old children was assessed in 1982 and 1992; the prevalence of atopy did not change after 10 years, whereas the prevalence of BHR increased 1.5- to 2.2-fold, and was more prominent among the atopic group.6 Therefore, Australian study is a good example that presented atopy as an important risk factor for both current and future BHR. In a study involving 892 seven- to eleven-year-old schoolchildren, atopic status and bronchial responsiveness were assessed twice 3.5 years apart, in 1987 (survey 1) and in 1990-1991 (survey 2).7 The level of BHR (percent decline in forced expiratory volume in 1 second [FEV1] per mg/mL methacholine) was higher in the atopic group than in the non-atopic group, with the highest value in the group of subjects who were persistently atopic during the survey period. Those who were atopic in survey 1 but not in survey 2 had a higher/lower level of BHR in the former/latter survey, which indicates that atopic status is reflected by the level of BHR. A similar tendency in the prevalence of BHR was observed in 10-year-old subjects enrolled in an Isle of Wight cohort, with the highest prevalence in a group of subjects who were persistently atopic from the age of 4 to 10 years followed by a group of subjects who were non-atopic at 4 but atopic at 10, and those who were atopic at 4 but not at 10.8 These results strengthen the relationship between BHR and atopy, with an emphasis on the persistence and the current status of atopy.
The relationship between BHR and atopy is specific to the sensitizing allergen. In the New Zealand study mentioned above, the prevalence of BHR was elevated in subjects sensitized to house dust mite (HDM) and to cat epithelia.9 Moreover, the prevalence was more elevated in those sensitized to both allergens simultaneously, whereas it was not higher than that of non-atopic subjects when children were sensitized to allergens other than HDM or cat epithelia. A study involving 1,412 Swedes reported that BHR prevalence was strongly related to cat epithelia sensitization and weakly to grass pollen sensitization, but not to sensitization to HDM, birch, mugwort, or molds.10 In a Korean study on symptomatic children who visited the allergy clinic of a tertiary hospital,11 HDM and pollen sensitization among five allergen groups (HDM, pollen, mold, pets, and cockroaches) were related to BHR in all subjects but only HDM sensitization was related to BHR when the study was confined to subjects diagnosed as having bronchial asthma. Sensitization to other allergens was not related to BHR. A further study on Korean high school students reported that 12.3% had BHR and 53% were sensitized to at least one allergen (the HDM sensitization rate was up to 40%).12 Atopic subjects were at a higher risk of BHR, especially when they were sensitized to indoor allergens or molds rather than pollens, and to multiple allergens rather than a single allergen. These results indicate that the association between atopy and BHR is allergen-specific but that the specific allergens vary across the studies. In general, sensitization to HDM is strongly correlated with BHR in coastal areas, whereas in dry inland regions sensitization to Alternaria fungi or pollens is more important.2,13
BHR also shows a significant relationship with the degree of atopy when evaluated based on serum levels of total IgE. It has long been reported that BHR to methacholine is correlated with the level of total IgE in the serum, which has been observed not only in subjects with asthma and rhinitis but also in asymptomatic subjects.14 A birth cohort study reported that the level of total IgE at the age of 11 years was separately associated with BHR at the ages of 9 and 15 years.15 In a general population study involving 600 subjects, of five common allergens (HDM, Timothy grass, birch, cat, and mold), subjects sensitized to HDM had a significantly higher prevalence of BHR than those who were not sensitized.16 Although the prevalence of BHR in those sensitized to cat or mold was higher, this was not significant. Furthermore, those sensitized to Timothy grass and birch pollen did not exhibit an increase in the prevalence of BHR. This result indicates the antigen-specificity of the relationship between atopy and BHR in the general population.
VARIATION IN BHR ACCORDING TO ALLERGEN EXPOSURE OR AVOIDANCE
In atopic subjects, BHR increases or decreases according to the level of exposure. Indeed, in subjects who are sensitized to seasonal allergens, BHR increases in the relevant season and returns to its normal level out of season. Moreover, BHR increases after an allergen provocation test, whereby exposure is increased artificially. For a perennial allergen, the level of BHR varies according to the environment or the specific period.
In a study on 13 seasonal asthmatics who were sensitized to ragweed pollen, methacholine PC20 decreased significantly during pollen season but not outside of the season.17 In a study on 10 atopic asthmatics sensitized to grass or Parietaria pollens, methacholine PC20 measured 5 months after the season increased significantly compared to that measured during the relevant season.18 This elevation in BHR in relationship to the increase in exposure to seasonal allergen is not limited to asthmatic patients. In previous studies, subjects with AR who were sensitized to pollen allergens displayed an increase in the frequency and degree of BHR during the pollen season when BHR was assessed using carbachol19 or methacholine.20
The seasonal variation in BHR is not confined to subjects sensitized to seasonal allergens. In a study on nine subjects sensitized to HDM, researchers measured the Der p I concentration in the living room and the bedroom every other week and BHR to histamine every month.21 They found seasonal variation in Der p I concentration and PC20 to histamine, whereby the former was highest in autumn (and lowest in spring) and the latter was lowest in autumn (and highest in spring). In a study on 165 atopic asthmatics, while PC20 was highest in the spring and lowest in the autumn in subjects mono-sensitized to HDM, it was highest in the winter and lowest in the summer in those co-sensitized with pollen allergens.22 In a further study on asthmatic subjects sensitized to HDM, the concentrations of Der p I and Der p II measured at each patient's house were significantly negatively correlated with the cumulative provocative dose of methacholine, inducing a 20% fall in FEV1 (PD20).23 These results indicate a close relationship between variation in BHR and the concentration of HDM allergens.
Allergen provocation tests, which increase the level of exposure to a relevant allergen, increase BHR in atopic patients. In a study in which changes in BHR to histamine or methacholine before and after allergen challenge tests were evaluated in 13 asthmatic patients, all 4 subjects who showed definite late asthmatic responses (LARs) and 3 of 5 subjects who displayed equivocal LARs had increased BHRs, which persisted for up to 7 days.24 In another study, the degree and duration of a decrease in PC20 to histamine were well correlated with the degree of LARs.25 The presence of LARs appears to be a key feature associated with an increase in BHR. In another study, when the methacholine challenge test was performed 24 hours after allergen provocation with relevant allergens in 31 subjects with mild asthma, a significant decrease in PC20 was observed only in the 21 subjects who showed LARs.26 This indicates that the presence of an LAR is an important risk factor for an elevated BHR. The importance of exposure to a relevant allergen in an environment other than the laboratory has also been reported. The Childhood Asthma Management Program (CAMP) reported a significantly lower level of methacholine PC20 in subjects exposed to allergens to which they were sensitized than in those who were not exposed.27
The increase in BHR parallel to the increase in allergen exposure appears to be related to an elevation in the eosinophilic inflammation of the lower airway. In a study on patients with seasonal AR, methacholine PC20 was significantly associated with the level of total IgE in the serum and the number of eosinophils during the relevant season.20 In a study on induced sputum in seasonal AR, an increase in eosinophil counts in the serum and a decrease in the number of apoptotic eosinophils were observed only during the relevant season.28 In a study of 17 seasonal asthmatics sensitized to grass pollen, and on whom bronchial biopsies and bronchoalveolar lavage (BAL) were performed before and after the relevant season, all subjects showed increased airway inflammation during the relevant season as indicated by an increase in the number of T cells, eosinophils, and degranulated mast cells.29 In addition, in a study on 12 asthmatic patients who had methacholine provocation tests and BAL before and after allergen provocation tests, the decrease in methacholine PD20 was correlated with eosinophil numbers in the BAL fluids.30 Finally, a study on 50 asthmatic patients who underwent methacholine provocation tests and sputum inductions before and after the allergen provocation test showed a significant association between changes in methacholine PC20 and the number of eosinophils in their induced sputum.31 These results indicate that the increase in BHR after exposure to a seasonal allergen or after laboratory provocation by the related allergen may occur through an increase in inflammation of the eosinophilic airway.
Elevated BHR can be diminished by avoidance of the associated allergens. The decrease in BHR in patients with pollen allergy after the relevant season is a good example. In one study, when subjects sensitized to HDM moved to a region of the Alps with few to no HDMs, both the level of total IgE and specific IgE decreased as did BHR to histamine,32 which indicates the efficacy of avoiding the relevant perennial allergen. In another study in which 13 asthmatic children sensitized to HDM moved to high-altitude regions of Switzerland, monthly bronchial provocation tests showed that, after moving, BHR to methacholine did not change whereas BHR to adenosine 5'-monophosphate (AMP) or exercise significantly decreased.33 This result suggests that the improvement of BHR after allergen avoidance is more readily revealed by indirect rather than direct stimuli. In addition, in a study in which asthmatic patients sensitized to HDM were kept in a hospital isolation ward, enabling complete avoidance of HDM for more than 2 months, BHR to histamine as well as the asthmatic symptoms decreased.34 Finally, a study in which a low level of HDM was maintained for more than 9 months using a special treatment for furniture reported a fourfold reduction in BHR to histamine in asthmatic patients sensitized to HDM.35
BHR IN SUBJECTS WITH ATOPIC OR NON-ATOPIC ASTHMA
Although atopy is a major risk factor of asthma, a large proportion of asthmatic patients do not have atopy. Non-atopic asthmatics comprise a third of all asthmatics when taking into consideration discrepancies between reports, and share many features with atopic asthmatics in terms of clinical features, risk factors, immunologic mechanisms, and pathophysiology.36 There are currently three hypotheses about the pathophysiology of non-atopic asthma, namely, that one or more of the following processes are involved: allergic reaction to a currently undetermined antigen; localized allergic reaction of the bronchial mucosa to environment allergens, which are undetectable by a blood or skin test; and infection-associated activation of the immune system by a superantigen or by an autoantibody to a denatured tissue protein.37
Several BHR studies that have compared groups of atopic and non-atopic asthmatics have reported conflicting results. In a study on 214 ten-year-old current wheezers (113 atopic, 101 non-atopic), the prevalence of subjects who had a methacholine PC20 of <4 mg/mL was higher in atopic than in non-atopic asthmatics.38 A recent study on 136 school-aged asthmatics also reported a higher prevalence of BHR to methacholine and a lower PC20 in atopic asthmatics than in non-atopic asthmatics.39 In contrast, in one study, the prevalence of BHR to methacholine in adult asthmatics was not different between atopic and non-atopic groups.40 Similarly, in a study on pediatric asthmatics (n=135), methacholine PC20 was not different in the presence or absence of atopy.41 In our recent study on 120 children with asthma, no significant difference in methacholine PC20 was found between children with (n=94) and without (n=26) atopy (2.00 mg/mL vs. 2.95 mg/mL).42 However, a partial difference was found when BHR was assessed using a specialized method. In a study on pediatric asthmatics, although the degree of sensitivity was the same in atopic and non-atopic groups, the degree of reactivity was higher in non-atopic asthmatics.43
These conflicting results are largely not understood, although several reasons have been postulated. First, because of the loose diagnostic criteria of asthma, some of those in the non-asthmatic general population might be misclassified as being asthmatic. Therefore, a significant difference in BHR in the general population might be reflected in studies on asthmatic patients. Indeed, in the aforementioned studies, the frequency of using controller medications was higher in atopic than in non-atopic groups,38 and the prevalence of positive BHR was lower (atopic, 78%; non-atopic, 48.5%).39 In another study, asymptomatic patients thought to be asthmatic also showed a lower prevalence of BHR (atopic, 41/81 vs. non-atopic, 7/37), which suggests that not all of the subjects were in fact asthmatic patients.44 Second, the unequal distribution of other variables that can influence the presence of BHR (i.e., younger age, earlier symptom presentation, parental history of asthma, smoking exposure, a decrease in baseline lung function)41 may influence the difference in BHR between atopic and non-atopic groups. Third, a difference in the degree of BHR might be specifically related to a single specific allergen rather than to atopy itself. In an early study, sensitization to HDM showed a significant relationship with BHR, whereas sensitization to grass did not.45 In a retrospective study on adult asthmatics, a patient group with lower methacholine PC20 had a higher rate of sensitization to HDM than to other antigens.46
The results of comparing BHR between atopic and non-atopic asthmatics differ depending on the type of stimulus used to provoke bronchial constriction. In one study, atopic asthmatics more frequently had BHR to AMP or cold air than non-atopic asthmatics, whereas there was no difference in the prevalence of BHR to methacholine.40 In another, school-aged asthmatics who had BHR to AMP showed a higher frequency of positive SPTs than those who did not.47 Recently, we reported that AMP PC20, other than methacholine PC20, was significantly lower in atopic asthmatics compared to non-atopic asthmatics in a retrospective review of results of BHR to both methacholine and AMP in school-aged asthmatics.42
The fact that BHR to methacholine is similar in atopic and non-atopic asthmatics whereas BHR to AMP is different may indicate that atopic asthmatics have more severe eosinophilic airway inflammation than non-atopic asthmatics, because BHR to AMP is more closely related to eosinophilic airway inflammation.48 In a study that measured exhaled NO, atopic asthmatics had a higher level of fractional exhaled nitric oxide (FeNO) than did normal controls, whereas non-atopic asthmatics showed no difference.49 Moreover, when bronchoscopic biopsies were performed, atopic asthmatics showed airway inflammation involving eosinophils, mast cells, and T cells, whereas in non-atopic asthmatics it was composed of neutrophils and mast cells. In a study in which the patterns of inflammation in induced sputum were compared between atopic asthma, non-atopic asthma, and non-atopic non-asthma groups, the first group had a higher percentage of eosinophils than the second group, which itself had a higher percentage of neutrophils than the last group.50 These results imply that eosinophilic airway inflammation is more prominent in atopic asthma than in non-atopic asthma, which would explain the higher degree of BHR to AMP in atopic asthmatics.
RELATIONSHIP BETWEEN THE DEGREE OF ATOPY AND BHR IN ASTHMATIC PATIENTS
The difference in BHR between atopic and non-atopic asthmatics is not sufficient to delineate the relationship between atopy and BHR: the distinction between atopy and non-atopy is frequently obscure, and the degree of atopy varies greatly among atopic subjects. For this reason, quantifying the degree of atopy appears to be an appropriate alternative to verifying the association between atopy and BHR.
There are various ways to quantify the degree of atopy, however, no consensus criterion has been agreed upon. Total IgE in the serum, specific IgE, the wheal size to the most reactive allergen, the number of positive SPT results, and/or the sum of wheal sizes are used to quantify the degree of atopy. Although total IgE can easily be assessed, normal cut-off points are arbitrary and vary according to age and sex. Moreover, the specific IgE antibody, which mainly contributes to total IgE, varies according to geographic location.51 The specific IgE antibody or the wheal size to the most reactive allergen are easy to interpret, but provide only limited information on the overall atopic status. The number of positive SPT results would serve as a clear criterion, however, it cannot differentiate between major and minor allergens, and may therefore underestimate the atopic status in those who react strongly but exclusively to a few allergens. Summing the total wheal sizes can also provide a good solution, but it can be strongly affected by a few strong allergens. Some researchers have proposed using a "sum of scores" system to determine atopic status.1 Each response is scored from + to ++++ and atopic status is assessed by summing these scores. The resulting score can reflect each strong response when subjects are sensitized to a few allergens and can avoid an excessive response to a few allergens when subjects are sensitized to many allergens.
Studies on the relationship between the degree of atopy and the severity of BHR have shown conflicting results. For example, BHR to methacholine in asthmatic patients has been shown to have a good52 or a poor45,53 association with the degree of atopy. Even in studies confined to atopic asthmatics, the degree of atopy shows conflicting relationships with BHR to methacholine or histamine.1,54,55 A retrospective study reported a higher sensitization rate in those who have BHR to AMP,56 whereas another study reported no association with BHR to AMP.52 The authors of this latter study hypothesized that the association would be more clear when BHR to AMP is pinpointed in atopic patients with asthma. We assessed the degree of atopy from the level of total IgE, the number of positive SPTs, and the sum of the atopic scores in school-aged atopic asthmatics, and found that as the degree of atopy increased, AMP PC20 decreased, whereas methacholine PC20 did not change.42 This implies that, in asthmatic patients, BHR influenced by atopy would be more clearly reflected by AMP than by methacholine. This trend was replicated in our similar study on preschool atopic asthmatics.57 While the methacholine end-point concentration (EPC) displayed no trend in response to the increase in the degree of atopy, AMP EPC decreased when the level of total IgE and the atopic score increased. These results also indicate that in asthmatics the degree of atopy is well correlated with the degree of eosinophilic airway inflammation. Indeed, total IgE in the serum is associated with the FeNO concentration in asthmatic children.58 Moreover, a further study reported that both total IgE and HDM-specific IgE are well correlated with FeNO.59
RELATIONSHIP BETWEEN THE DEGREE OF ATOPY AND BHR IN NON-ASTHMATIC AR PATIENTS
Among rhinitis patients, allergic subjects more frequently have BHR than non-allergic subjects. A study on adult rhinitis patients showed that subjects with BHR (n=161) had a greater prevalence of atopy, larger serum eosinophil counts, and a higher level of serum total IgE than those without BHR (n=249).60 In a larger study, adult patients with AR (n=506) had a higher frequency of BHR than those without AR (n=153) (34.9% vs. 19.9%).61
Because BHR is more frequent in subjects with AR than in those without AR, whether BHR prevalence is different across the level of atopy in AR subjects would be of great concern. We found no difference in the number of positive SPTs, the type of positive allergens, or the level of total IgE in the serum when we compared a group of school-aged AR patients who had BHR (n=42) to those who did not have BHR (n=73).62 Other researchers have reported similar results. In one study that analyzed school-aged AR patients, the number of positive SPTs or blood eosinophils were not different between those with BHR (n=31) and those without BHR (n=20), although the former group had a higher frequency of persistent rhinitis and a higher level of total IgE.63 Another study showed a similar number of positive SPTs and level of total IgE between school-aged AR subjects with BHR (n=13) and those without BHR (n=15).64 In contrast, a further study on AR patients showed a close association, because those who had BHR (n=23) had a greater number of positive SPTs than those who did not have BHR (n=36) (4.04±2.03 vs. 2.63±1.24, P=0.04).65 Furthermore, the number of positive SPTs had a negative correlation with methacholine PC20.
The conflicting results might be derived from the disparity in atopic composition, i.e., the types of sensitized allergens or the ranges of the degree of atopy. In a previous study, a group of AR subjects sensitized to perennial allergens showed a higher frequency of BHR than those sensitized to seasonal allergens, while in subjects with seasonal AR the degree of BHR measured in the relevant season was higher than when measured out of season.66 Although in the study that reported no association, the subjects had on average two positive SPTs,63 the subjects in the study that reported a good correlation had on average four positive SPTs.65 Moreover, in the latter study, most of the subjects who had more than five positive SPTs displayed BHR.
The methods used to measure the degree of atopy may have resulted in the prevalence of BHR to methacholine not being proportional to the number of SPTs in AR subjects. In contrast, the relationship with the degree of atopy may be more sensitive when BHR is measured in relation to AMP rather than to methacholine, as seen for the asthmatic subjects. We measured BHR to both methacholine and AMP for 88 AR subjects and analyzed their relationship to indices of the degree of atopy (total IgE in the serum, number of positive SPTs, and sum of atopic scores based on the wheal sizes).67 We found BHR to methacholine in 22 (25%) subjects and to AMP in 30 (34%) subjects, while those with three atopic indices were not different between the groups with or without BHR to methacholine. Total IgE in the serum and atopic scores were higher in the groups with BHR to AMP than those not sensitive to AMP. Moreover, when we divided each atopic index into three segments and compared the prevalence of BHR to both methacholine and AMP across the segments, the prevalence of BHR to methacholine showed no trend, whereas that to AMP showed an increasing tendency associated with total IgE and the sum of the atopic scores. These results indicate that in AR subjects the frequency of BHR to AMP rather than to methacholine is more associated with atopic parameters, as is found in atopic asthmatic subjects.
CONCLUSION
Although much conflicting evidence is presented here, atopy and BHR are closely associated not only in asthmatic subjects but also in non-asthmatic subjects, including AR subjects and the general population. Moreover, in some specific groups, the degree of atopy is well correlated with the degree of BHR. This association is more prominent when BHR is assessed by AMP than when assessed by methacholine. This evidence indicates that eosinophilic airway inflammation may be involved in the association between atopy and BHR.
Footnotes
There are no financial or other issues that might lead to conflict of interest.
References
- 1.Crockcroft DW, Murdock KY, Berscheid BA. Relationship between atopy and bronchial responsiveness to histamine in a random population. Ann Allergy. 1984;53:26–29. [PubMed] [Google Scholar]
- 2.Peat JK, Britton WJ, Salome CM, Woolcock AJ. Bronchial hyperresponsiveness in two populations of Australian schoolchildren. III. Effect of exposure to environmental allergens. Clin Allergy. 1987;17:291–300. doi: 10.1111/j.1365-2222.1987.tb02017.x. [DOI] [PubMed] [Google Scholar]
- 3.Backer V, Ulrik CS, Hansen KK, Laursen EM, Dirksen A, Bach-Mortensen N. Atopy and bronchial responsiveness in random population sample of 527 children and adolescents. Ann Allergy. 1992;69:116–122. [PubMed] [Google Scholar]
- 4.Burrows B, Sears MR, Flannery EM, Herbison GP, Holdaway MD. Relations of bronchial responsiveness to allergy skin test reactivity, lung function, respiratory symptoms, and diagnoses in thirteen-year-old New Zealand children. J Allergy Clin Immunol. 1995;95:548–556. doi: 10.1016/s0091-6749(95)70317-9. [DOI] [PubMed] [Google Scholar]
- 5.Helenius IJ, Tikkanen HO, Sarna S, Haahtela T. Asthma and increased bronchial responsiveness in elite athletes: atopy and sport event as risk factors. J Allergy Clin Immunol. 1998;101:646–652. doi: 10.1016/S0091-6749(98)70173-3. [DOI] [PubMed] [Google Scholar]
- 6.Peat JK, van den Berg RH, Green WF, Mellis CM, Leeder SR, Woolcock AJ. Changing prevalence of asthma in Australian children. BMJ. 1994;308:1591–1596. doi: 10.1136/bmj.308.6944.1591. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Forastiere F, Corbo GM, Dell'Orco V, Pistelli R, Agabiti N, Kriebel D. A longitudinal evaluation of bronchial responsiveness to methacholine in children: role of baseline lung function, gender, and change in atopic status. Am J Respir Crit Care Med. 1996;153:1098–1104. doi: 10.1164/ajrccm.153.3.8630551. [DOI] [PubMed] [Google Scholar]
- 8.Kurukulaaratchy RJ, Matthews S, Arshad SH. Relationship between childhood atopy and wheeze: what mediates wheezing in atopic phenotypes? Ann Allergy Asthma Immunol. 2006;97:84–91. doi: 10.1016/S1081-1206(10)61375-0. [DOI] [PubMed] [Google Scholar]
- 9.Sears MR, Burrows B, Herbison GP, Holdaway MD, Flannery EM. Atopy in childhood. II. Relationship to airway responsiveness, hay fever and asthma. Clin Exp Allergy. 1993;23:949–956. doi: 10.1111/j.1365-2222.1993.tb00280.x. [DOI] [PubMed] [Google Scholar]
- 10.Plaschke P, Janson C, Norrman E, Björnsson E, Ellbjär S, Järvholm B. Association between atopic sensitization and asthma and bronchial hyperresponsiveness in swedish adults: pets, and not mites, are the most important allergens. J Allergy Clin Immunol. 1999;104:58–65. doi: 10.1016/s0091-6749(99)70114-4. [DOI] [PubMed] [Google Scholar]
- 11.Yu J, Yoo Y, Kang H, Kim DK, Choi SH, Koh YY. The relationship between allergen sensitization and bronchial hyperresponsiveness in children aged 6-8 years. Pediatr Allergy Respir Dis. 2005;15:344–351. [Google Scholar]
- 12.Kim BS, Jin HS, Kim HB, Lee SY, Kim JH, Kwon JW, Kim BJ, Yu J, Yoo S, Hong SJ. Airway hyperresponsiveness is associated with total serum immunoglobulin E and sensitization to aeroallergens in Korean adolescents. Pediatr Pulmonol. 2010;45:1220–1227. doi: 10.1002/ppul.21312. [DOI] [PubMed] [Google Scholar]
- 13.Peat JK, Tovey E, Mellis CM, Leeder SR, Woolcock AJ. Importance of house dust mite and Alternaria allergens in childhood asthma: an epidemiological study in two climatic regions of Australia. Clin Exp Allergy. 1993;23:812–820. doi: 10.1111/j.1365-2222.1993.tb00258.x. [DOI] [PubMed] [Google Scholar]
- 14.Sears MR, Burrows B, Flannery EM, Herbison GP, Hewitt CJ, Holdaway MD. Relation between airway responsiveness and serum IgE in children with asthma and in apparently normal children. N Engl J Med. 1991;325:1067–1071. doi: 10.1056/NEJM199110103251504. [DOI] [PubMed] [Google Scholar]
- 15.Burrows B, Sears MR, Flannery EM, Herbison GP, Holdaway MD, Silva PA. Relation of the course of bronchial responsiveness from age 9 to age 15 to allergy. Am J Respir Crit Care Med. 1995;152:1302–1308. doi: 10.1164/ajrccm.152.4.7551386. [DOI] [PubMed] [Google Scholar]
- 16.Omenaas E, Bakke P, Eide GE, Elsayed S, Gulsvik A. Serum house dust mite antibodies: predictor of increased bronchial responsiveness in adults of a community. Eur Respir J. 1996;9:919–925. doi: 10.1183/09031936.96.09050919. [DOI] [PubMed] [Google Scholar]
- 17.Boulet LP, Cartier A, Thomson NC, Roberts RS, Dolovich J, Hargreave FE. Asthma and increases in nonallergic bronchial responsiveness from seasonal pollen exposure. J Allergy Clin Immunol. 1983;71:399–406. doi: 10.1016/0091-6749(83)90069-6. [DOI] [PubMed] [Google Scholar]
- 18.Prieto L, Bertó JM, Lopez M, Peris A. Modifications of PC20 and maximal degree of airway narrowing to methacholine after pollen season in pollen sensitive asthmatic patients. Clin Exp Allergy. 1993;23:172–178. doi: 10.1111/j.1365-2222.1993.tb00878.x. [DOI] [PubMed] [Google Scholar]
- 19.Madonini E, Briatico-Vangosa G, Pappacoda A, Maccagni G, Cardani A, Saporiti F. Seasonal increase of bronchial reactivity in allergic rhinitis. J Allergy Clin Immunol. 1987;79:358–363. doi: 10.1016/0091-6749(87)90156-4. [DOI] [PubMed] [Google Scholar]
- 20.Di Lorenzo G, Mansueto P, Melluso M, Morici G, Norrito F, Esposito Pellitteri M, Di Salvo A, Colombo A, Candore G, Caruso C. Non-specific airway hyperresponsiveness in mono-sensitive Sicilian patients with allergic rhinitis. Its relationship to total serum IgE levels and blood eosinophils during and out of the pollen season. Clin Exp Allergy. 1997;27:1052–1059. doi: 10.1111/j.1365-2222.1997.tb01257.x. [DOI] [PubMed] [Google Scholar]
- 21.van der Heide S, de Monchy JG, de Vries K, Bruggink TM, Kauffman HF. Seasonal variation in airway hyperresponsiveness and natural exposure to house dust mite allergens in patients with asthma. J Allergy Clin Immunol. 1994;93:470–475. doi: 10.1016/0091-6749(94)90356-5. [DOI] [PubMed] [Google Scholar]
- 22.Riccioni G, Di Stefano F, De Benedictis M, Verna N, Cavallucci E, Paolini F, Di Sciascio MB, Della Vecchia R, Schiavone C, Boscolo P, Conti P, Di Gioacchino M. Seasonal variability of non-specific bronchial responsiveness in asthmatic patients with allergy to house dust mites. Allergy Asthma Proc. 2001;22:5–9. doi: 10.2500/108854101778249221. [DOI] [PubMed] [Google Scholar]
- 23.Custovic A, Taggart SC, Francis HC, Chapman MD, Woodcock A. Exposure to house dust mite allergens and the clinical activity of asthma. J Allergy Clin Immunol. 1996;98:64–72. doi: 10.1016/s0091-6749(96)70227-0. [DOI] [PubMed] [Google Scholar]
- 24.Cockcroft DW, Ruffin RE, Dolovich J, Hargreave FE. Allergen-induced increase in non-allergic bronchial reactivity. Clin Allergy. 1977;7:503–513. doi: 10.1111/j.1365-2222.1977.tb01481.x. [DOI] [PubMed] [Google Scholar]
- 25.Cartier A, Thomson NC, Frith PA, Roberts R, Hargreave FE. Allergen-induced increase in bronchial responsiveness to histamine: relationship to the late asthmatic response and change in airway caliber. J Allergy Clin Immunol. 1982;70:170–177. doi: 10.1016/0091-6749(82)90038-0. [DOI] [PubMed] [Google Scholar]
- 26.Ketchell RI, D'Amato M, Jensen MW, O'Connor BJ. Contrasting effects of allergen challenge on airway responsiveness to cysteinyl leukotriene D(4) and methacholine in mild asthma. Thorax. 2002;57:575–580. doi: 10.1136/thorax.57.7.575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Nelson HS, Szefler SJ, Jacobs J, Huss K, Shapiro G, Sternberg AL. The relationships among environmental allergen sensitization, allergen exposure, pulmonary function, and bronchial hyperresponsiveness in the Childhood Asthma Management Program. J Allergy Clin Immunol. 1999;104:775–785. doi: 10.1016/s0091-6749(99)70287-3. [DOI] [PubMed] [Google Scholar]
- 28.Kurt E, Bavbek S, Aksu O, Erekul S, Misirligil Z. The effect of natural pollen exposure on eosinophil apoptosis and its relationship to bronchial hyperresponsiveness in patients with seasonal allergic rhinitis. Ann Allergy Asthma Immunol. 2005;95:72–78. doi: 10.1016/S1081-1206(10)61191-X. [DOI] [PubMed] [Google Scholar]
- 29.Djukanović R, Feather I, Gratziou C, Walls A, Peroni D, Bradding P, Judd M, Howarth PH, Holgate ST. Effect of natural allergen exposure during the grass pollen season on airways inflammatory cells and asthma symptoms. Thorax. 1996;51:575–581. doi: 10.1136/thx.51.6.575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Oddera S, Silvestri M, Penna R, Galeazzi G, Crimi E, Rossi GA. Airway eosinophilic inflammation and bronchial hyperresponsiveness after allergen inhalation challenge in asthma. Lung. 1998;176:237–247. doi: 10.1007/pl00007606. [DOI] [PubMed] [Google Scholar]
- 31.Imaoka H, Gauvreau GM, Watson RM, Strinich T, Obminksi GL, Howie K, Killian KJ, O'Byrne PM. Sputum inflammatory cells and allergen-induced airway responses in allergic asthmatic subjects. Allergy. 2011;66:1075–1080. doi: 10.1111/j.1398-9995.2011.02588.x. [DOI] [PubMed] [Google Scholar]
- 32.Boner AL, Niero E, Antolini I, Valletta EA, Gaburro D. Pulmonary function and bronchial hyperreactivity in asthmatic children with house dust mite allergy during prolonged stay in the Italian Alps (Misurina, 1756 m) Ann Allergy. 1985;54:42–45. [PubMed] [Google Scholar]
- 33.Benckhuijsen J, van den Bos JW, van Velzen E, de Bruijn R, Aalbers R. Differences in the effect of allergen avoidance on bronchial hyperresponsiveness as measured by methacholine, adenosine 5'-monophosphate, and exercise in asthmatic children. Pediatr Pulmonol. 1996;22:147–153. doi: 10.1002/(SICI)1099-0496(199609)22:3<147::AID-PPUL2>3.0.CO;2-M. [DOI] [PubMed] [Google Scholar]
- 34.Platts-Mills TA, Tovey ER, Mitchell EB, Moszoro H, Nock P, Wilkins SR. Reduction of bronchial hyperreactivity during prolonged allergen avoidance. Lancet. 1982;2:675–678. doi: 10.1016/s0140-6736(82)90709-7. [DOI] [PubMed] [Google Scholar]
- 35.Htut T, Higenbottam TW, Gill GW, Darwin R, Anderson PB, Syed N. Eradication of house dust mite from homes of atopic asthmatic subjects: a double-blind trial. J Allergy Clin Immunol. 2001;107:55–60. doi: 10.1067/mai.2001.111240. [DOI] [PubMed] [Google Scholar]
- 36.Pearce N, Pekkanen J, Beasley R. How much asthma is really attributable to atopy? Thorax. 1999;54:268–272. doi: 10.1136/thx.54.3.268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Corrigan C. Mechanisms of intrinsic asthma. Curr Opin Allergy Clin Immunol. 2004;4:53–56. doi: 10.1097/00130832-200402000-00011. [DOI] [PubMed] [Google Scholar]
- 38.Kurukulaaratchy RJ, Fenn M, Matthews S, Arshad SH. Characterisation of atopic and non-atopic wheeze in 10 year old children. Thorax. 2004;59:563–568. doi: 10.1136/thx.2003.010462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Castro-Rodriguez JA, Navarrete-Contreras P, Holmgren L, Sanchez I, Caussade S. Bronchial hyperreactivity to methacholine in atopic versus nonatopic asthmatic schoolchildren and preschoolers. J Asthma. 2010;47:929–934. doi: 10.3109/02770903.2010.504875. [DOI] [PubMed] [Google Scholar]
- 40.Lúdvíksdóttir D, Janson C, Björnsson E, Stålenheim G, Boman G, Hedenström H, Venge P, Gudbjörnsson B, Valtysdóttir S. Different airway responsiveness profiles in atopic asthma, nonatopic asthma, and Sjogren's syndrome. BHR Study Group. Bronchial hyperresponsiveness. Allergy. 2000;55:259–265. doi: 10.1034/j.1398-9995.2000.00252.x. [DOI] [PubMed] [Google Scholar]
- 41.Harmanci K, Bakirtas A, Turktas I. Factors affecting bronchial hyperreactivity in asthmatic children. J Asthma. 2008;45:730–734. doi: 10.1080/02770900802385992. [DOI] [PubMed] [Google Scholar]
- 42.Suh DI, Lee JK, Kim CK, Koh YY. Methacholine and adenosine 5'-monophosphate (AMP) responsiveness, and the presence and degree of atopy in children with asthma. Pediatr Allergy Immunol. 2011;22:e101–e106. doi: 10.1111/j.1399-3038.2010.01110.x. [DOI] [PubMed] [Google Scholar]
- 43.Mochizuki H, Shigeta M, Tokuyama K, Morikawa A. Difference in airway reactivity in children with atopic vs nonatopic asthma. Chest. 1999;116:619–624. doi: 10.1378/chest.116.3.619. [DOI] [PubMed] [Google Scholar]
- 44.Gruber W, Eber E, Steinbrugger B, Modl M, Weinhandl E, Zach MS. Atopy, lung function and bronchial responsiveness in symptom-free paediatric asthma patients. Eur Respir J. 1997;10:1041–1045. doi: 10.1183/09031936.97.10051041. [DOI] [PubMed] [Google Scholar]
- 45.Ferrante E, Corbo GM, Valente S, Ciappi G. Associations between atopy, asthma history, respiratory function and non-specific bronchial hyperresponsiveness in unselected young asthmatics. Respiration. 1992;59:169–172. doi: 10.1159/000196050. [DOI] [PubMed] [Google Scholar]
- 46.Currie GP, Jackson CM, Lee DK, Lipworth BJ. Determinants of airway hyperresponsiveness in mild asthma. Ann Allergy Asthma Immunol. 2003;90:560–563. doi: 10.1016/S1081-1206(10)61851-0. [DOI] [PubMed] [Google Scholar]
- 47.Bakirtas A, Turktas I. Determinants of airway responsiveness to adenosine 5'-monophosphate in school-age children with asthma. Pediatr Pulmonol. 2006;41:515–521. doi: 10.1002/ppul.20355. [DOI] [PubMed] [Google Scholar]
- 48.van den Berge M, Meijer RJ, Kerstjens HA, de Reus DM, Koeter GH, Kauffman HF, Postma DS. PC(20) adenosine 5'-monophosphate is more closely associated with airway inflammation in asthma than PC(20) methacholine. Am J Respir Crit Care Med. 2001;163:1546–1550. doi: 10.1164/ajrccm.163.7.2010145. [DOI] [PubMed] [Google Scholar]
- 49.Lúdvíksdóttir D, Janson C, Högman M, Hedenström H, Björnsson E, Boman G. Exhaled nitric oxide and its relationship to airway responsiveness and atopy in asthma. BHR-Study Group. Respir Med. 1999;93:552–556. doi: 10.1016/s0954-6111(99)90154-3. [DOI] [PubMed] [Google Scholar]
- 50.Drews AC, Pizzichini MM, Pizzichini E, Pereira MU, Pitrez PM, Jones MH, Sly PD, Stein RT. Neutrophilic airway inflammation is a main feature of induced sputum in nonatopic asthmatic children. Allergy. 2009;64:1597–1601. doi: 10.1111/j.1398-9995.2009.02057.x. [DOI] [PubMed] [Google Scholar]
- 51.Erwin EA, Rönmark E, Wickens K, Perzanowski MS, Barry D, Lundbäck B, Crane J, Platts-Mills TA. Contribution of dust mite and cat specific IgE to total IgE: relevance to asthma prevalence. J Allergy Clin Immunol. 2007;119:359–365. doi: 10.1016/j.jaci.2006.12.648. [DOI] [PubMed] [Google Scholar]
- 52.Fowler SJ, Lipworth BJ. Relationship of skin-prick reactivity to aeroallergens and hyperresponsiveness to challenges with methacholine and adenosine monophosphate. Allergy. 2003;58:46–52. doi: 10.1034/j.1398-9995.2003.23779.x. [DOI] [PubMed] [Google Scholar]
- 53.Takeda K, Shibasaki M, Takita H. Relation between bronchial responsiveness to methacholine and levels of IgE antibody against Dermatophagoides farinae and serum IgE in asthmatic children. Clin Exp Allergy. 1993;23:450–454. doi: 10.1111/j.1365-2222.1993.tb00353.x. [DOI] [PubMed] [Google Scholar]
- 54.Martín-Muñoz F, Moreno-Ancillo A, Pestaña JA, Contreras-Porta J, Díaz-Peña JM, Ojeda JA. Atopy and bronchial hyperresponsiveness in pure extrinsic childhood asthma. J Investig Allergol Clin Immunol. 1997;7:229–233. [PubMed] [Google Scholar]
- 55.Lombardi C, Passalacqua G, Ciprandi G, Scordamaglia A, Canonica GW. Relationship between degree of nonspecific hyperresponsiveness and number of positive skin tests in asthmatics. Monaldi Arch Chest Dis. 2000;55:181–184. [PubMed] [Google Scholar]
- 56.Currie GP, Jackson CM, Lee DK, Lipworth BJ. Allergen sensitization and bronchial hyper-responsiveness to adenosine monophosphate in asthmatic patients. Clin Exp Allergy. 2003;33:1405–1408. doi: 10.1046/j.1365-2222.2003.01772.x. [DOI] [PubMed] [Google Scholar]
- 57.Suh DI, Lee JK, Kim CK, Koh YY. Bronchial hyperresponsiveness to methacholine and adenosine 5'-monophosphate, and the presence and degree of atopy in young children with asthma. Clin Exp Allergy. 2011;41:338–345. doi: 10.1111/j.1365-2222.2010.03664.x. [DOI] [PubMed] [Google Scholar]
- 58.Cardinale F, de Benedictis FM, Muggeo V, Giordano P, Loffredo MS, Iacoviello G, Armenio L. Exhaled nitric oxide, total serum IgE and allergic sensitization in childhood asthma and allergic rhinitis. Pediatr Allergy Immunol. 2005;16:236–242. doi: 10.1111/j.1399-3038.2005.00265.x. [DOI] [PubMed] [Google Scholar]
- 59.Sacco O, Sale R, Silvestri M, Serpero L, Sabatini F, Raynal ME, Biraghi M, Rossi GA. Total and allergen-specific IgE levels in serum reflect blood eosinophilia and fractional exhaled nitric oxide concentrations but not pulmonary functions in allergic asthmatic children sensitized to house dust mites. Pediatr Allergy Immunol. 2003;14:475–481. doi: 10.1046/j.0905-6157.2003.00092.x. [DOI] [PubMed] [Google Scholar]
- 60.Di Lorenzo G, Pacor ML, Mansueto P, Esposito Pellitteri M, Lo Bianco C, Ditta V, Leto-Barone MS, Napoli N, Di Fede G, Rini GB. Determinants of bronchial hyperresponsiveness in subjects with rhinitis. Int J Immunopathol Pharmacol. 2005;18:715–722. doi: 10.1177/039463200501800414. [DOI] [PubMed] [Google Scholar]
- 61.Mølgaard E, Thomsen SF, Lund T, Pedersen L, Nolte H, Backer V. Differences between allergic and nonallergic rhinitis in a large sample of adolescents and adults. Allergy. 2007;62:1033–1037. doi: 10.1111/j.1398-9995.2007.01355.x. [DOI] [PubMed] [Google Scholar]
- 62.Koh YY, Lee MH, Kim CK, Min YG, Kim YK, Min KU, Kim YY. A familial predisposition in bronchial hyperresponsiveness among patients with allergic rhinitis. J Allergy Clin Immunol. 1998;102:921–926. doi: 10.1016/s0091-6749(98)70329-x. [DOI] [PubMed] [Google Scholar]
- 63.Cuttitta G, Cibella F, La Grutta S, Hopps MR, Bucchieri S, Passalacqua G, Bonsignore G. Non-specific bronchial hyper-responsiveness in children with allergic rhinitis: relationship with the atopic status. Pediatr Allergy Immunol. 2003;14:458–463. doi: 10.1046/j.0905-6157.2003.00067.x. [DOI] [PubMed] [Google Scholar]
- 64.Cibella F, Cuttitta G, La Grutta S, Hopps MR, Passalacqua G, Pajno GB, Bonsignore G. Bronchial hyperresponsiveness in children with atopic rhinitis: a 7-year follow-up. Allergy. 2004;59:1074–1079. doi: 10.1111/j.1398-9995.2004.00559.x. [DOI] [PubMed] [Google Scholar]
- 65.Mete N, Sin A, Gulbahar O, Erdinc M, Sebik F, Kokuludag A. The determinants of bronchial hyperresponsiveness in patients with allergic rhinitis. Ann Allergy Asthma Immunol. 2004;93:193–199. doi: 10.1016/S1081-1206(10)61475-5. [DOI] [PubMed] [Google Scholar]
- 66.Verdiani P, Di Carlo S, Baronti A. Different prevalence and degree of nonspecific bronchial hyperreactivity between seasonal and perennial rhinitis. J Allergy Clin Immunol. 1990;86:576–582. doi: 10.1016/s0091-6749(05)80215-5. [DOI] [PubMed] [Google Scholar]
- 67.Kim CK, Choi SJ, Lee JK, Suh DI, Koh YY. Bronchial hyperresponsiveness to methacholine and adenosine monophosphate and the degree of atopy in children with allergic rhinitis. Ann Allergy Asthma Immunol. 2011;106:36–41. doi: 10.1016/j.anai.2010.10.019. [DOI] [PubMed] [Google Scholar]