

Abstract
Background:
Human rights violations among the people with mental illness were not an uncommon occurrence. The present study was aimed to compare persons with psychiatric illness and their caregivers’ perceptions regarding the human rights status of people with mental illness in the community.
Materials and Methods:
A descriptive design was carried out among randomly selected asymptomatic psychiatric patients and their caregivers (N=200) at a tertiary care center. Data was collected through face-to-face interview, using a structured questionnaire. Data was analyzed and interpreted using descriptive and inferential statistics.
Results:
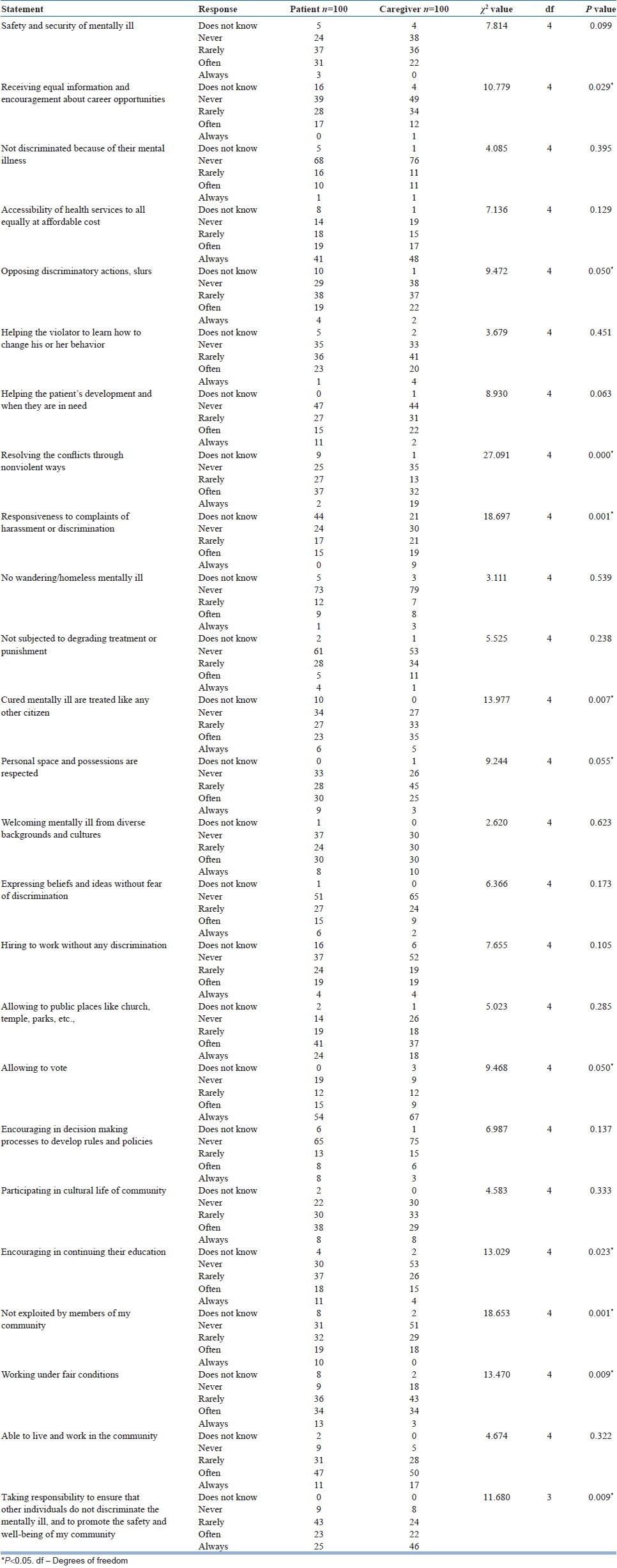
Our findings revealed that the caregivers than psychiatric patients perceived negatively to the statements i.e., ‘Receiving equal information and encouragement about career opportunities’ (χ2=10.779, P<0.029), ‘Opposing discriminatory actions, slurs’ (χ2=9.472, P<0.050) ‘Resolving the conflicts with people with mental illness through nonviolent ways’ (χ2=27.091, P<0.000), ‘Responding to the complaints of harassment or discrimination against the people with mental illness’ (χ2=18.697, P<0.001), ‘Encouraged to continue their education’ (χ2=13.029, P<0.023) ‘Exploitation by the community members’ (χ2=18.653, P<0.001) and working under fair conditions (χ2=13.470, P<0.009).
Conclusion:
The study suggests that there is an urgent need to take necessary steps to protect, promote, and fulfill human rights of people with mental illness through providing care, educating the community, and strengthening the legislations.
Keywords: Caregivers, community, human rights, human rights violations, mentally ill
INTRODUCTION
People with mental illness encountering human rights violations in meeting their basic needs are a reality to be found in every corner of the globe.[1] The Preamble to the Constitution of India assures equal treatment and equality of opportunity and status to all the citizens. Every person with a mental illness has the same basic rights as every other person, specifically including the rights set out in the International Covenant on Civil and Political Rights (ICCPR) and the rights recognized in the Declaration on the Rights of Disabled Persons; that discrimination on the basis of mental illness is not permitted and that people being treated for a mental illness must be accorded the right to recognition as a person before the law.[2] Despite the adequate legislations, we often come across horrendous stories about the way people with mental illness are treated in community and various psychiatric institutions.[3] Further, World Health Organization (WHO) states that we are “facing a global human rights emergency in mental health” as many countries lack the basic legal framework to protect those with a disability.[4] A free India was not an exception, as evident by the National Human Rights Commission report[5] which highlighted the gross inadequacies and subhuman living conditions in mental hospitals. Furthermore, India's dismal record of rights violations of the mentally ill was glaringly exposed with the grotesque death of 25 patients at an “asylum” in Tamil Nadu.[6] The lack of human rights or their violations, as seen in the Erwadi tragedy and similar cases, does not stem from a shortcoming in existing Indian or international law per se; but is the result of social stigma, prejudice, and other social and economic factors linked with mental illness.[7]
Community care has been a paradigm shift for psychiatric treatment worldwide. The success of deinstitutionalization depends on a number of key conditions: The establishment of a comprehensive community support system, an environment that allows the people with mental illness to experience all the rights of citizenship as other individuals do, and tolerance and nondiscrimination in the local community.[8] However, studies have provided evidences of high levels of bullying, harassment, and exploitation experienced by people with mental health problems while living in the community.[9] In addition, they continue to ‘suffer from widespread, systematic discrimination and are consistently denied the rights and services to which they are entitled’.[10] A qualitative study, explored the Taiwanese mentally ill persons’ difficulties living in the community and six themes were identified as follows: Getting a “shameful” illness, unmet needs for community care, being overcome by a distorted world, denying the illness, living with the illness, and adapting to changed level of functioning.[11]
The shift to community-based psychiatric services has formalized the role of the caregiver. The role of family becomes even greater in a developing country like India with more than 1 billion people where there is a paucity of trained personnel, with the number of mental health professionals not exceeding 5,000. For such a huge population, both settings and service providers are grossly inadequate.[12] Further, National Institute of Mental Health and Neuroscience (NIMHANS) in Bangalore estimates that 2 crore Indians need help for serious mental disorders, while a further 5 crore suffer from mental illnesses which are not considered very serious. NIMHANS also estimates that at least 35 lakh Indians need hospitalization on account of mental illnesses. But the country has only 40 institutions that are equipped to treat patients suffering from mental disorders.[13] Thus, a large part of the mental healthcare takes place in the community making the family as the primary care provider. However, the Stigma, residual disability and its intolerance, and more importantly the inability of the mentally ill to protest against exploitation; have all made basic human rights of the mentally ill a major cause of growing concern. Hence, the present study aimed to compare the psychiatric patients’ and their caregivers’ perceptions regarding the human rights status in the community.
MATERIALS AND METHODS
This was a descriptive study conducted on asymptomatic patients with mental illness attending the outpatient department of a tertiary care center between August and November 2010.
Researchers used a random number table to recruit potential subjects who received an initial assessment by a psychiatrist using the Clinical Global Impression-Improvement (CGI-I) Scale.[14] The selected participants were first assessed by a psychiatrist using the Clinical Global Impression-Improvement (CGI-I) Scale. In the present study, asymptomatic (remitted) patients defined as the patients who scored 1(very much improved) or 2 (much improved) on CGI-I scale. Hence, asymptomatic people with mental illness may be the true representative of the target population, because they can ascertain and verbalize their experience of human rights in better way. Among these, asymptomatic patients who met the inclusion criteria were included in the study. The study criteria include; a) asymptomatic psychiatric patients with past history of diagnosis of either schizophrenia or mood disorders based upon the criteria of the International Classification of Disorders Version 10, b) both male and female participants c) within the age group of 18-60 years, d) participants who were willing to participate were interviewed after they gave the written informed consent, and e) availability of a caregiver (caregiver is person who is providing care for the patient at least for past 6 months). Symptomatic, substance abuse, mentally disabled, and cognitively impaired patients were excluded. Subjects meeting these criteria were interviewed after providing a written informed consent. The final sample size was 200.
Data collection tools
The instruments used in this study were:
CGI-I scale: The CGI-I Scale[14] is a standardized instrument to assess illness severity, illness change over time and medication efficacy, taking in to and side effect severity. The instrument uses a 7-point scale, with possible responses for the severity of illness scale ranging from 1 (normal) through 7 (most severely ill)
Sociodemographic schedule: Socio demographic details include; age, gender, educational status, marital status, employment, residence, religion, monthly income, type of family, diagnosis, and duration of illness (in months). In case of caregivers; monthly income, type of family, diagnosis, and duration of illness were excluded
The researchers employed a modified version of “Taking the Human Rights Temperature of Your Community” tool to assess the human rights of the mentally ill in the community.[15] This tool was modified to suit the Indian context with regard to mental illness while retaining the essence of questions. For example, the researchers modified the original statement “My community is a place where residents are safe and secure,” to read “My community is a place where mentally ill patients are safe and secure”.
Item numbers 12, 17, 18, 21, and 22 were completely changed as suggested by the experts. According to the Indian constitution and international covenants (International Covenant on Economic, Social and Cultural Rights-ICESCR and ICCPR); right to vote, right to continuing education, right not to be discriminated were given more importance and exploring these issues were more relevant to the present study. This scale contained 25 items and used a 5-point scale rated from 0 (does not know) to 4 (always). The above mentioned instruments were developed in English language, as the study was undertaken at a tertiary care center where people from different cultures, languages, and traditions come for treatment and represent their communities. Hence, researchers decided to administer the structured questionnaire in a face-to-face interview format.
Instrument validity and reliability
Eleven experts from diverse fields; including nursing, psychiatry, psychiatric social work, psychology, human rights activism, and statistics; validated the tool. A revised version was modified to incorporate the experts’ suggestions. A test-retest method assessed reliability. The researcher administered the instrument on 10 asymptomatic patients with mental illness and their caregivers at a follow-up outpatient department over a 2-week period and found the study feasible with necessary modifications. The reliability coefficient for the final version of the structured questionnaire was 0.96.
Data was collected by the primary author through face-to-face interview, in a private room at the treatment facilities where the participants were recruited and it took approximately 20 min to complete the structured questionnaire. The researchers conducted group education sessions for family members on the human rights of persons with mental illness. Although educating the family members was not a part of the research, after the pilot study it was observed that patients as well as caregivers were not aware of the human rights of persons with mental illness and thus, the researchers felt that educating the family members may help in protecting the human rights of persons with mental illness.
Ethical consideration
The study was approved by the ethics committee (EC) of NIMHANS, India. Participation in the study was voluntary and each participant was informed that their decision to participate or not, would in no way not affect his/her treatment. All responses to the questionnaire remained confidential and a code was used so participants could not be identified from their responses.
The data was analyzed using SPSS version 16 and results were presented in the form of tables. Descriptive (frequency and percentage) and inferential statistics (Chi-square test) was used to interpret the data. Categories with insufficient numbers were combined when performing Chi-square analysis.
RESULTS
Sample characteristics
Among the 200 participants, 50% were asymptomatic psychiatric patients. Mean age for patients was 34.68±10.69 (Mean±Standard Deviation) years and mean age for caregivers was 43.41±12.89 years. Majority of the participants from both groups were men (53% patients and 64% caregivers). The number of caregivers (48%) who had primary education was slightly higher than patients (43%). A significant association was observed between patients and caregivers related to their marital status (χ2=25.432, P<0.000). More number (81%) of the caregivers was married than patients (68%). Similarly, more caregivers (69%) than patients (46%) were employed (χ2=19.391, P<0.001). Most of the sample was Hindus (86% patients and 88% caregivers). The average income of the participants was Rs. 4,919±5,724. Majority (78%) of the participants belonged to above poverty line (monthly family income is above Rs. 1,700). The number of participants from urban (54%) was slightly higher than the participants from rural (46%) [Table 1].
Table 1.
Demographic details comparing patients with caregivers
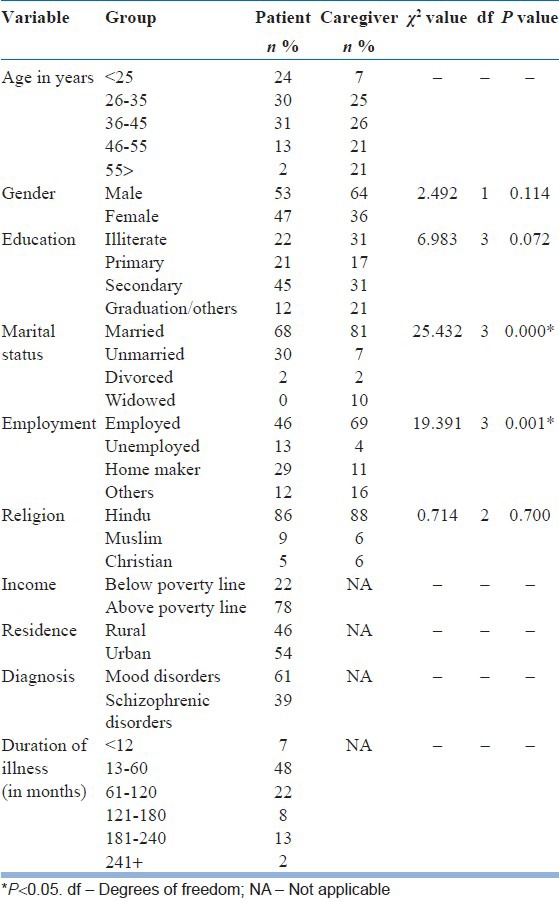
Table 2 shows the responses of participants to the human rights measurement questionnaire. A significant association was identified for the statement ‘Receiving equal information and encouragement about career opportunities’ between patients and caregivers (χ2=10.779, P<0.029). More number of caregivers (83%) than patients (67%) expressed that the people with mental illness ‘never/rarely’ receive equal information and encouragement about their career opportunities. Three-fourth of the caregivers than patients (67%) reported that the community members ‘never/rarely’ oppose discriminatory actions, slurs against people with mental illness (χ2=9.472, P<0.050). Majority of the patients (52%) stated that the community members do not resolve the conflicts with people with mental illness through nonviolent ways (χ2=27.091, P<0.000). The number of caregivers (51%) was slightly higher than patients (41%) who agreed that the community members ‘never/rarely’ responds to the complaints of harassment or discrimination against the people with mental illness (χ2=18.697, P<0.001). Interestingly, 44% of the patients were not aware of complaining procedures. Similarly, more number of the caregivers (40%) than patients (29%), concurred that cured people with mental illness were not treated like other citizens (χ2=13.977, P<0.007). A significant association was found between patients and caregivers to the item ‘personal space and possessions are respected’ (χ2=9.244, P<0.055). Majority of the caregivers (71%) expressed that personal space and possessions of people with mental illness were never/rarely respected. A significant association (χ2=9.468, P<0.050) was identified between patients and caregivers to the statement ‘allowing to vote’. More number of patients (31%) than caregivers (21%) expressed that they were ‘never/rarely’ allowed to vote in their community. However, majority of the patients (69%) as well as caregivers (76%) agreed that people with mental illness were allowed to vote. More than three-fourth of caregivers (79%) than patients (67%) stated that people with mental illness were ‘never/rarely’ encouraged continuing their education (χ2=13.029, P<0.023). Considerably good number (80%) of caregivers and 63% of patients perceived that people with mental illness were exploited by the community members (χ2=18.653, P<0.001). More number of caregivers (61%) than the patients (45%) accepted that people with mental illness ‘never/rarely’ were allowed to work under fair conditions (χ2=13.470, P<0.009). Majority of the caregivers (68%) than patients (48%) accepted that they take responsibility to ensure other individuals in the community do not discriminate mentally ill and promote the safety and well-being of their community (χ2=11.680, P<0.009).
Table 2.
Comparison of perception human rights variables between patients and caregivers
DISCUSSION
The present study compares psychiatric patients’ and their caregivers’ perceptions regarding the human rights status of people with mental illness in their community. The study was unique in nature, as the participated patients were asymptomatic and their caregivers who witnessed human rights violations among people with mental illness in their community. Hence, they may be the true representative of the target population.
As in other studies, present study also provided evidence that the number of men among patients group was marginally higher than women who utilized the mental health services. However, the healthcare services are marked by gender-based inequity of access to hospital care. Findings from a recent study, conducted in two psychiatric facilities in Andhra Pradesh, provided further confirmation of gender differences in accessing to the mental healthcare.[16] In addition, majority of the caregivers (81%) were married than patients. Patients with severe mental disorders such as schizophrenia are more likely to remain single and unmarried than patients in other diagnostic groups. This is particularly true of male patients and can probably be explained by the fact that women tend to be younger than men when first married and are less likely to have experienced an initial psychotic episode. Further, single males appear to be over-represented in schizophrenia samples, including epidemiological studies such as the WHO's 10-country study.[17] On contrary, it is estimated that over 75% Indians (rich or poor) believe that marriage is a cure for mental illnesses like manic depression, bipolar affective disorders, and even schizophrenia.[18] However, in a 10-year follow up study,[19] it was found that ‘marital outcome in Indian patients is good with no significant gender differences’. The high marital rate (about 70% being married before the onset of the illness), presence of children, a shorter duration of illness at inclusion, and the presence of auditory hallucinations at intake were all associated with a good marital outcome.
Access to meaningful, paid work is a basic human right for every citizen, and those who experience serious mental illness should have equal access to the fundamental elements of citizenship which include: Housing, education, income, and work. This means that each individual has the right to be employed in a mainstream job, rather than being labeled as a client in a training program or a sheltered workshop. Perhaps, 46% of the patients were employed. People with mental illness are some of the most disadvantaged in labor market.[20] Further, studies have shown a clear interest in work and employment activities among users of psychiatric services, with up to 90% of users wishing to go into (or back to) work.[21] Work is important, both in maintaining mental health and in promoting the recovery of those who have experienced mental health problems. Enabling people to retain or gain employment has a profound effect on more life domains than almost any other medical or social intervention.[22] Barriers to work are linked to stigma, prejudice, and discrimination. In addition, promoting job opportunities for such people changes both, the public perception and their own perception of themselves. Further, in the current study, 83% of caregivers reported that the people with mental illness were not received information regarding their career opportunities. Community discrimination against people with mental illness was not an uncommon occurrence. Though, there was no significant association observed between the patients and caregivers, majority (84% patients and 87% caregivers) of the participants expressed that people with mental illness were discriminated in the community. These findings were in concurrent with a recent survey conducted in England, in which 85% respondents agreed that people with mental illness experience stigma and discrimination.[23] Contrary to these findings, stigma and discrimination described by the family members and caregivers were different than what was perceived by the patients.[24] Few Indian studies have reported that women with mental disorders face the highest levels of stigma, in addition to that associated with separation or divorce, and were especially disadvantaged since they often received no financial support from their former husbands.[25] However, in India very few studies have focused on the multifaceted stigma of mental illness and its impact on the human rights of the patient.[26,27]
All of us have the right to decent and productive work in conditions of freedom, equity, security, and human dignity. Nevertheless, achieving this right is particularly challenging in case of persons with mental health problems.[28] In a recent survey, 251 (32%) of the mental health service users reported that they had been subjected to hostility or harassment in the community.[29] Present study also concur with these findings, as majority of the caregivers expressed that their community members do not oppose discriminatory actions and slurs (75%) and respond to the complaints of harassment (51%) against the people with mental illness. Further, the patients described that they were called with various names such as ‘mad’, ‘psycho’, ‘idiot’, ‘mental’, ‘retard’, and so forth by the community members. In a developing country like India, many cases such as discrimination and harassment pass unnoticed or unchallenged. According to a report, there are around 400,000 wandering mentally ill people in India. They are the ‘invisible people’, separated from and/or neglected by their families.[30] Yet, in the present study, majority of the participants (73% patients and 79% caregivers) accepted that they have witnessed people with mental illness being homeless, wandering on the streets, around railway stations, bus stands, pilgrim centers, and on street corners. However, homelessness is a crucial issue especially in case of women suffering from mental illness. A study conducted in Delhi with a population of 70 million is found to have nearly 2,500 women with mental illness who have no hope to live and are virtually on the street. If it extrapolates for the whole nation, the country will have nearly 150,000 mentally-ill destitute women.[31] A homeless woman with mental illness is extremely vulnerable for sexual abuse and needs urgent support and care from both governmental and non-governmental organizations (NGOs). Our findings have also shown that cured (asymptomatic) mentally ill were not treated like other people, and their personal space and possessions were not respected. These findings reflect the negative attitude of the community towards people with mental illness. Interestingly, both the group of participants agreed that the right to vote of people with mental illness were protected in the community. A recent study[32] provided evidence that people with serious mental illness are capable of voting. Further, an Italian survey[33] discovered that 68% of caregivers of the mentally ill believed that a person with experience of mental illness should be able to vote. In a democratic society like India, the right to vote is one of the most valued civil rights, because it is considered essential towards protection of other rights.
Education and training are often a precursor to a person gaining employment, increasing opportunities, and realizing potential. In the present study, 79% of the caregivers agreed that people with mental illness were not encouraged for continuing their education. These findings were contrary to a survey conducted in New Zealand, of the 785 respondents, 478 (61%) said they had not been discriminated during education. However, one in five respondents reported that they experienced discrimination in education or training, from other students through to the teachers or tutors.[29] Majority of the caregivers stated that people with mental illness were exploited (80%) and were not working under fair conditions. They reported that people with mental illness were paid less salary, working for long hours, and doing menial job, etc. Majority of the participants (48% patients and 68% caregivers) agreed to take responsibility to ensure that other individuals do not discriminate the people with mental illness and promote the safety and well-being of their community.
The present study has certain limitations such as; the study was restricted to the people with recovered severe mental illness and their caregivers who attended outpatient department at a tertiary care center and smaller sample size may hinder the generalization of the findings. The type I errors may be high due to the item wise Chi-square analysis. Prospective longitudinal research is vital to examine the human rights violations among people with mental illness in the community. Future research should focus on larger sample size and qualitative approach for in depth understanding of human rights issues among these disadvantaged populations. Despite these limitations, our study also has several strengths such as; creating awareness among the patients and their relatives regarding the human rights of people with mental illness. Further, it contains interesting findings from developing countries perspective, which will be of use to both researchers and clinicians.
CONCLUSION
In a nutshell, the findings of the present study highlights that more of the caregivers than psychiatric patients perceived that the human rights of people with mental illness were not protected and influencing their reintegration into the community. The findings of the present study also suggest that it is high time to strengthen the legal frame work to protect the rights of people with mental illness. However, legal sanction may not provide adequate protection; hence mental health professionals, NGOs, professional organizations, and other stakeholders should unify their efforts in educating and changing community attitudes towards mental illness and advocating for human rights of people with mental illness.
ACKNOWLEDGMENT
The researchers would like to thank the participants and their family members for their valuable contributions.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Gostin LO. Human rights of persons with mental disabilities. The European convention of human rights. Int Law Psychiatry. 2000;23:125–59. doi: 10.1016/s0160-2527(99)00039-4. [DOI] [PubMed] [Google Scholar]
- 2.Human Rights Of Mentally Ill Persons. [Last accessed on Dec 7, 2011]. Available www.Legal Service India.com. database on the Internet .
- 3.Gadit AA. Abuse of mentally ill patients: Are we ignoring the human rights principle? J Pak Med Assoc. 2008;58:523–4. [PubMed] [Google Scholar]
- 4.WHO. Mental health, human rights and legislation: A global human rights emergency in mental health. [Last accessed on June 2, 2012]. Available at www.who.int/mental_health/policy/legislation/en/index.html .
- 5.Pratima M, Nagaraja D. Bangalore, India: National Institute of Mental Health and Neuro Sciences (Deemed University), and National Human Rights Commission, New Delhi (2008); [Last accessed on February 20, 2012]. Mental Health; Human Rights. Available online at http://nhrc.nic.in/Publications/Mental_Health_Care_and_Human_Rights.pdf . [Google Scholar]
- 6.IANS. In India, mentally ill are treated as prisoners, not as patients. The New Indian Express. [Last accessed on June 2, 2012]. Available at http://wwwcscsarchiveorg: 8081/MediaArchive/libertynsf/(docid)/17E050063CFFC470E5256B5900184A8E .
- 7.Sharma S. The Indian institutional mental care experience. Curr Opin Psychiatry. 2003;16:547. [Google Scholar]
- 8.Hannigan B. Mental health care in the community: An analysis of contemporary public attitudes towards, and public representations of, mental illness. J Ment Health. 1999;8:431–40. [Google Scholar]
- 9.MIND. “Mind's campaign for equal access to justice for people with mental health problems”. [Last date accessed 2nd December 2011]. Available at http://www.mind.org.uk/anotherassault/
- 10.Burdekin B, Guilfoyle M, Hall D. Australian Government Printing Service; 1993. Human rights and mental illness: Report of the National Inquiry into the Human Rights of People with Mental Illness Canberra. [Google Scholar]
- 11.Lin CL, Kopelowicz A, Chan CH, Hsiung PC. A qualitative inquiry into the Taiwanese mentally ill persons’ difficulties living in the community. Arch Psychiatric Nur. 2008;22:266–76. doi: 10.1016/j.apnu.2007.07.002. [DOI] [PubMed] [Google Scholar]
- 12.Shankar RR. From Burden to Empowerment: The Journey of Family Caregivers in India. In: Sartorius N, Leff J, López-Ibor JJ, Maj M, Okasha A, editors. Families and Mental Disorders: From Burden to Empowerment. Chichester, England: John Wiley and Sons; 2005. pp. 259–90. [Google Scholar]
- 13.Ravindran N. The Silent Epidemic: 2 crore Indians need help for mental disorders. [Last Accessed 2nd June, 2012]. Retrieved from: http://indiatoday.intoday.in/story/2-crore-indians-need-help-for-mental-disorders/1/143355.html .
- 14.Guy W. Clinical Global Impressions: In ECDEU Assessment. Manual for Psychopharmacology. 1976:218–22. [Google Scholar]
- 15.Flowers N, Bernbaum M, Rudelius-Palmer K, Tolman J. The human rights education handbook: Effective practices for learning, action and change. Retreived from http://www.scribd.com/doc/53987765/Human-Rights-Education-Handbook-Effective-Practices-for-Learning-Action-Change-Flowers 2000 .
- 16.Vindhya U. Mental health care: A review of gender differences. Int J Diabetes Dev Ctries. 2001;21:86–95. [Google Scholar]
- 17.Jablensky A, Sartorius N, Ernberg G, Anker M, Korten A, Cooper JE, et al. Schizophrenia: Manifestations, incidence and course in different cultures. A World Health Organization ten-country study. Psychol Med Monogr Suppl. 1992;20:1–97. doi: 10.1017/s0264180100000904. [DOI] [PubMed] [Google Scholar]
- 18.Barat T. Marriage and Mental Illness. [Last accessed on 2010 Nov 30]. Avaialable at http://www.boloji.com/index.cfm?md=Content and sd=Articles and ArticleID=6443 .
- 19.Thara R, Srinivasan TN. Outcome of marriage in schizophrenia. Soc Psychiatry Psychiatr Epidemio. 1997;32:416–20. doi: 10.1007/BF00788182. [DOI] [PubMed] [Google Scholar]
- 20.Improving Services to People with Mental Health Difficulties. Coventry: LSC; 2006. Learning and Skills Coucil. [Google Scholar]
- 21.Grove B. Mental health and employment. Shaping a new agenda. J Ment Health. 1999;8:131–40. [Google Scholar]
- 22.Boardman J, Bob G, Rachel P, Geoff S. Work and employment for people with psychiatric disabilities. Br J Psychiatry. 2003;182:467–8. doi: 10.1192/bjp.182.6.467. [DOI] [PubMed] [Google Scholar]
- 23.The NHS Information Centre. Attitudes to Mental Illness -2011 survey report 2011, England The Health and Social Care Information Centre. [Last accessed on 2011 Nov 16]. Available from: www.ic.nhs.uk/pubs/attitudestomi11 .
- 24.Schulze B, Angermeyer MC. Subjective experiences of stigma: A focus group study of schizophrenic patients, their relatives and mental health professionals. Soc Sci Med. 2002;56:299–312. doi: 10.1016/s0277-9536(02)00028-x. [DOI] [PubMed] [Google Scholar]
- 25.Saxena S, Thornicroft G, Knapp M, Whiteford H. Resources for mental health: Scarcity, inequity, and inefficiency. Lancet. 2007;370:878–89. doi: 10.1016/S0140-6736(07)61239-2. [DOI] [PubMed] [Google Scholar]
- 26.Thara R, Srinivasan TN. How stigmatizing is schizophrenia in India? Int J Soc Psychiatry. 2000;46:135–41. doi: 10.1177/002076400004600206. [DOI] [PubMed] [Google Scholar]
- 27.Weiss M, Jadhav S, Raguram R, Vounatsou P, Littlewood R. Psychiatric stigma across cultures: Local validation in Bangalore and London. Anthropol Med. 2001;8:71. [Google Scholar]
- 28.Gaston H, Phyllis G. Geneva: World Health Organization; 2000. Mental health: Impact, issues and good practices. [Google Scholar]
- 29.Peterson D, Lynne P, Nancy S, Gael S. New Zealand, Auckland: Mental Health Foundation of New Zealand; 2004. Respect Costs Nothing: A survey of discrimination faced by people with experience of mental illness in Aotearoa; p. 62. [Google Scholar]
- 30.Sridhar L. NIMHANS recommends the Banyan model for mental healthcare. [Last accessed on 2003 Nov 16]. Available at http://www.infochangeindia.org/public-health/features/nimhans-recommends-the-banyan-model-for-mental-healthcare. html .
- 31.NationalSeminar, “MENTALLY ILL WOMEN- IS DESTITUTION THE ONLY ANSWER.?”. New Delhi. [Last accessed on 2011 Nov 12]. Available www.ncw.nic.in/./Mental_health .
- 32.Raad R, Karlawish J, Appelbaum PS. The Capacity to Vote of Persons With Serious Mental Illness. Psychiatr Serv. 2009;60:624. doi: 10.1176/ps.2009.60.5.624. [DOI] [PubMed] [Google Scholar]
- 33.Magliano LM, Guarneri EA. “A multicenter Italian study of patients’ relatives’ beliefs about schizophrenia”. Psychiatr Serv. 2001;52:1528–30. doi: 10.1176/appi.ps.52.11.1528. [DOI] [PubMed] [Google Scholar]