

Sir,
Chlorpromazine equivalence (CPZE) has been taught to psychiatrists over generations. The concept of anti-psychotic equivalence, CPZE in particular, has been used for long time to compare the dose and efficacy of the anti-psychotics. The application of this was much prevalent during the era of typical anti-psychotics, which slowly started fading away with widespread use of atypical anti-psychotics.[1] The reason being that the receptor profile of these group being different - typical only predominantly on D2 receptors (mostly) and atypical on serotonergic, histaminergic, cholinergic and adrenergic receptors over the dopaminergic receptors.[2] Nonetheless, the needs for a measure to compare the anti-psychotics on a common platform have been long felt and attempts have been made for the same. One such attempt is the concept of defined daily dose (DDD). In this critique, we comment about the concepts of CPZE and the DDD and present the chlorpromazine equivalents of the available anti-psychotic medications.
The standardized method to compare different anti-psychotics helps in determining the efficacy of the drug and in determining the target dose while changing from one medicine to another. Further, it helps in monitoring the side effect profile and assessing the costs of treatment. The chlorpromazine equivalent is one such measure, which has been used from the earlier days. Later the concept of DDD was introduced.
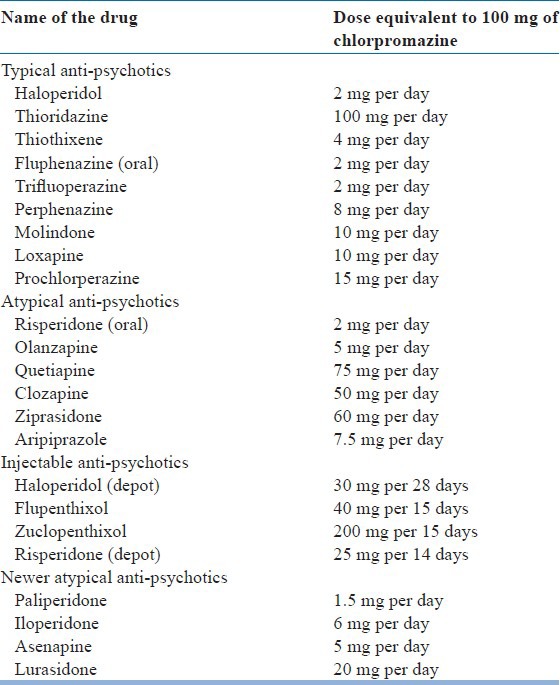
CPZE is defined as the dose of a drug, which is equivalent to 100 mg of oral dose of chlorpromazine. The drug equivalent to 200-300 mg of chlorpromazine is considered the minimum effective dose[3] and more than 1000 mg of chlorpromazine is considered high.[4] The literature gives the equivalence of anti-psychotics of first generation with much more clarity than the second generation drugs. The main reason for this being the action of later on serotonergic, histaminergic, cholinergic and adrenergic receptors over the dopaminergic receptors compared to the former.[2] However, even as the debate regarding the relevance of the equivalents for second generation drugs go on, Woods[5] in his review based on the reported minimum effective dose has arrived at the chlorpromazine equivalents of the atypical anti-psychotics. The equivalence of all the anti-psychotics, typicals, and atypicals, has been synthesized into Table 1 based on the data from the available review literature.
Table 1.
Chloropromazine equivalents of different anti-psychotics
The other critique on this concept is that the equivalence is based on the assumption that the relationship between the dose and the potency is linear, which may not be true for all the anti-psychotics, for example, the relative anti-psychotic potency of haloperidol significantly decreases as the dosage increases.[1] Although, the receptor profile seems to be the concept, the data are derived from clinical and anecdotal resources. This affects the observation as the sedative and anxiolytic effects of drugs would make drugs such as haloperidol seem less potent in comparison with chlorpromazine.[6]
The other available platform to compare anti-psychotics is based on their DDD. The DDD is defined as the assumed average maintenance dose per day for a drug used in its main indication in adults. This international unit was approved by World Health Organization (WHO) in 2003 and the values are determined by WHO collaborating center for drug statistics methodology. The advantage of DDD over the CPZE is that the DDD is calculated based on the review of published systematic studies.[7]
Studies have looked into the reliability and the agreement between the doses across the drugs. These studies have differing results. The studies by Rijcken et al.[8] and Barr et al.[9] reported significant difference for comparability between the DDD and the CPZE. The later reported that, CPZE is a reliable platform to compare the anti-psychotics owing to their affinity for dopamine receptor occupancy. However, a study by Nose et al.[7] had a result favoring the coherence between the two systems and noted that DDD is a reliable tool for comparison, as it is beyond the influence of price of the drug and maximum recommended values as per the individual national formularies.
Chlorpromazine equivalent and DDD are two widely used platforms to compare the doses of anti-psychotics. While CPZEs are easy to remember and use in day-to-day clinical practice, given the wide ranging differences in the pharmacodynamic profile of various anti-psychotics (ranging from apples to oranges), this yard stick seems to be limited in terms of its clinical utility. DDD seems to be a better option in the research settings, as it allows comparison across population. Further studies are warranted to standardize the methods to compare the anti-psychotics in terms of their efficacy and potency, based on their actions at the receptor levels.
ACKNOWLEDGMENT
Dr. Vijay Danivas is supported by the Welcome Trust/DBT India Alliance Senior Fellowship Grant to Dr. G. Venkatasubramanian.
REFERENCES
- 1.Atkins M, Burgess A, Bottomley C, Riccio M. Chlorpromazine equivalents: A consensus of opinion for both clinical and research applications. Psychiatr Bull. 1997;21:224–6. [Google Scholar]
- 2.Stahl SM, editor. 3rd ed. Cambridge University Press; 2008. Stahl's Essential Psychopharmacology: Neuroscientific Basis and Practical Applications; pp. 327–453. [Google Scholar]
- 3.Taylor D, Paton C, Kapur S, editors. London: Informa Healthcare; 2009. The Maudsley Prescribing Guidelines; p. 12. [Google Scholar]
- 4.Hung G. A comparison of two methods of calculating total antipsychotic dose. Hong Kong J Psychiatr. 2007;17:87–90. [Google Scholar]
- 5.Woods SW. Chlorpromazine equivalent doses for the newer atypical antipsychotics. J Clin Psychiatry. 2003;64:663–7. doi: 10.4088/jcp.v64n0607. [DOI] [PubMed] [Google Scholar]
- 6.Mullen R, Coon AW, Smith S. Perception of equivalent doses of neuroleptlc drugs. Psychiatr Bull. 1994;18:334–5. [Google Scholar]
- 7.Nosè M, Tansella M, Thornicroft G, Schene A, Becker T, Veronese A, et al. Is the Defined Daily Dose system a reliable tool for standardizing antipsychotic dosages? Int Clin Psychopharmacol. 2008;23:287–90. doi: 10.1097/YIC.0b013e328303ac75. [DOI] [PubMed] [Google Scholar]
- 8.Rijcken CA, Monster TB, Brouwers JR, de Jong-van den Berg LT. Chlorpromazine equivalents versus defined daily doses: How to compare antipsychotic drug doses? J Clin Psychopharmacol. 2003;23:657–9. doi: 10.1097/01.jcp.0000096247.29231.3a. [DOI] [PubMed] [Google Scholar]
- 9.Barr AM, Honer WG, Johnson JL, Wu TK, Procyshyn RM. A comparison of antipsychotic drug-defined daily doses versus chlorpromazine equivalent doses in patients with or without extrapyramidal motor symptoms. J Clin Psychopharmacol. 2010;30:741–3. doi: 10.1097/JCP.0b013e3181fab7ca. [DOI] [PubMed] [Google Scholar]