

Abstract
In many interventions that are based on an exercise program intended to induce weight loss, the mean weight loss observed is modest and sometimes far less than the individual expected. The individual responses are also widely variable, with some individuals losing a substantial amount of weight, others maintaining weight, and a few actually gaining weight. The media have focused on the sub-population that loses little weight, contributing to a public perception that exercise has limited utility to cause weight loss. The purpose of the symposium was to present recent, novel data that help explain how compensatory behaviors contribute to a wide discrepancy in exercise-induced weight loss. The presentations provide evidence that some individuals adopt compensatory behaviors, i.e. increased energy intake and/or reduced activity, that offset the exercise energy expenditure and limit weight loss. The challenge for both scientists and clinicians is to develop effective tools to identify which individuals are susceptible to such behaviors, and to develop strategies to minimize their impact.
Keywords: Energy expenditure, physical activity, non-exercise activity thermogenesis, energy intake
INTRODUCTION
The recent focus on exercise as medicine is predicated on a fundamental dose-response relationship; the application of exercise will confer benefits to health. On average, when previously sedentary individuals add exercise to their lifestyle, they become more physically fit, are at lower risk for many chronic disease and are better able to manage an appropriate body weight. This forms the basis for physical activity guidelines to enhance the health of the general public. The average response obscures considerable variability and the individual responses to habitual exercise deviate widely (Figure 1). In addition to the fortunate sub-group who lose body weight/fat, there are the unfortunate people who do not, despite completing a similar volume of exercise. It is clear that not only is there a large inter-individual variability in exercise-induced weight loss, but in general, people also tend to lose less weight than theoretically expected. For example, Ross and Janssen (58) reported that in studies lasting 25 weeks or longer, average weight loss is only 30% of predicted values. Although the phenomenon of individual variability in weight change in response to exercise or diet is not new (6, 53), it has yet to be exploited and used effectively to design better weight loss strategies.
Figure 1.
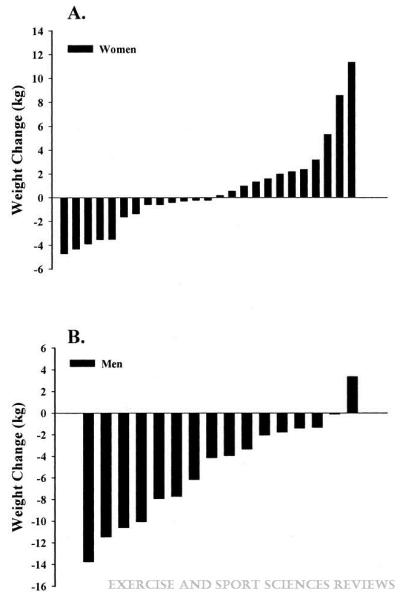
Individual 16-month weight change in exercise groups by gender. (A) Women. (B) Men. Adopted from (15) with permission.
Individuals who are weight stable are assumed to be in energy balance, i.e. energy intake (EI) = energy expenditure (EE); to induce an energy deficit and therefore weight loss, EE must exceed EI. Thus, the addition of structured exercise should theoretically result in energy deficit and weight loss. Of course, not completing the prescribed amount of exercise will also contribute to a lower than theoretically expected weight loss. However, the observation that observed weight loss is modest or less than expected persists in studies where exercise is closely supervised and continuously adjusted over the course of the intervention (13).
Therefore, people who lose little or no weight in response to adding structured exercise must be compensating for the increased EE of exercise by reducing their non-exercise physical activity and/or increasing their EI (Figure 2). Either compensatory response will attenuate or even reverse the energy deficit generated by adding structured exercise. However, data that support or refute the relative importance of less non-exercise activity or more EI in blunting the expected benefits of exercise on energy balance and body weight are equivocal. Contributing factors to this ambiguity include not monitoring of the exercise intervention, as well as accuracy and validity issues related to the measurement of EI and EE. The methodological issues are compounded by the fact that it is difficult to clamp EE during an exercise intervention because it is a behavioral adaptive response (i.e. non-exercise physical activity) that is also a dependent variable of interest.
Figure 2.

Components of total daily energy expenditure.
The purpose of this review is to summarize the presentations of participants in a symposium entitled “Behavioral Compensation to Exercise: Do We Eat More and Do Less?”, presented at the National American College of Sports Medicine Meeting in San Francisco, CA, in 2012. The purpose of the symposium was to present recent, novel data related to the effects of exercise, specifically prescribed for weight loss, on compensatory eating and physical activity behaviors. The strategy was to feature speakers who could present data from each side of the energy balance equation. Drs. Melanson and Kozey Keadle discussed the impact of exercise on non-exercise physical activity and EE, and Drs. King and Donnelly discussed the effect of exercise on energy and macronutrient intake. The objectives of this review are to present the state of knowledge regarding the magnitude and direction of activity and diet compensation, identify areas where more research is needed, provide guidance to improve exercise/diet recommendations, which in turn will improve the effectiveness of weight loss strategies.
EFECTS OF EXERCISE ON NON-EXERCISE PHYSICAL ACTIVITY
Total daily energy expenditure (TDEE) is the sum of resting metabolic rate, thermic effect of food (TEF), and physical activity energy expenditure (AEE) (Figure 2). AEE can be further divided into exercise (i.e., planned, structured physical activity, EXEE) or non-exercise physical thermogenesis (NEAT). In human studies, if the outcome measure is physical activity assessed via accelerometry, than the appropriate term to describe this is non-exercise physical activity (non-Ex PA). However, if the outcome is non-exercise EE measured using DLW or estimated from accelerometry or other methods (see next paragraph), then the appropriate term to use is NEAT. We have used this terminology to properly distinguish these two outcomes throughout the manuscript. In some studies, particularly animal studies, the term “spontaneous physical activity (SPA)” is often used to indicate NEAT. Thus, in some instances we have used the same terminology that was used by the authors. Garland et al. (23) recently addressed some challenges defining and measuring NEAT. For the purpose of this review, we are interested in determining whether individuals “do less” when they start exercise training. Therefore, we will broadly define non-Ex PA as including all activities of daily living which includes fidgeting, maintaining posture, and ambulation, and NEAT is the term that defines the EE associated with these activities (23, 37). In humans, NEAT is highly variable (37, 56, 75), is a strong positive predictor of TDEE (56, 72), and is likely influenced by environmental (18) and biological factors (29, 75). Studies in rodents suggest that multiple neuroregulators (e.g. dopamine, orexin A, leptin, ghrelin, agouti-related protein) play a role in regulating SPA/NEAT (23, 35).
Determining if behavioral compensation occurs in response to exercise training requires accurate measurement of all components of TDEE. However, obtaining accurate measures of TDEE in free-living EE in humans is challenging. The two most common approaches are the doubly labeled water (DLW) method (24, 49, 69) or the use activity monitors (12, 27, 41). A complete review of the various methods to measure physical activity have been published elsewhere (69). DLW is the gold standard method for measuring TDEE (69). When DLW is used in exercise training trials, NEAT is typically estimated using the measured or estimated resting metabolic rate and EXEE. Few studies actually measure the thermic effect of food; most assume it is 10% of TDEE and that it does not change during the intervention period. NEAT is thus estimated as the difference between TDEE and the sum of RMR and exercise EE (e.g., TDEE of 2500 kcal − (RMR of 1600 kcal + EXEE of 400kcal) = 500 kcal NEAT). The major limitation of this method is the cost, so sample sizes are typically small or contain only a sub-set of participants. In addition, DLW provides one value of EE over a period of days; thus, unless total EXEE is accounted for, it is difficult to detect changes in NEAT. DLW water does not provide information on the type of non-Ex PA that is taking place (e.g., sitting, ambulatory movement) or the patterns of physical activity. This is an important issue, as sedentary behavior has been shown to be predictive of health outcomes independent of total physical activity (47). These limitations can somewhat be overcome using activity monitors, but estimates of EE from accelerometry are less accurate than those from DLW (69).
Does NEAT contribute to body weight regulation?
The strongest evidence that NEAT plays a role in regulating body weight comes from studies in animals. For example, Teske et al. (65) demonstrated that obesity resistant rats had higher levels of SPA throughout their lifespan. Obviously, performing such a detailed longitudinal study in humans would not be feasible, and consequently, the evidence from human studies is not as convincing. The best evidence in humans comes from prospective studies performed in Pima Indians which demonstrated that SPA measured in a respiration chamber was inversely correlated with fat mass change in males (75). Interestingly, there was no association between SPA and fat mass change in females. This study also demonstrated that family membership accounted for 57% of the variation in SPA, suggesting that NEAT may be genetically programmed. Additional evidence that NEAT contributes to body weight regulations comes from two long-term overfeeding studies. The seminal studies of Bouchard (5) demonstrated that gains in fat mass were primarily determined by genetic factors (~50%), but given that physical activity levels were tightly controlled in this study, it is possible that differences in NEAT contributed to the unexplained variance in weight gain. The second study, by Levine and colleagues, demonstrated that changes in NEAT was the only component of EE that predicted fat gain (38). However, this was a small study (N=16), and as reviewed by Westerterp et al. (70) this is the only study in humans that demonstrated an increase in physical activity in response to overfeeding (38). Additionally, how NEAT may regulate body weight during experimental overfeeding may be different from what is experienced in free-living individuals. For example, data from a recent large (N=321) prospective study of free-living women demonstrated that AEE, determined using DLW, was not a predictor of weight change over three years of follow up (40). Even at modest levels of AEE (i.e., <4 MJ/d), some women lost weight, some remained weight stable, and others actually gained weight. Consistent with this latter study, two recent cross-sectional studies of ~120 individuals demonstrated that “incidental PA”, determined using accelerometry, is positively associated with cardiorespiratory fitness, but shows no association with abdominal fat mass (46, 47). Thus, definitive studies demonstrating a clear link between NEAT and body weight regulation in humans are still lacking.
Does initiation and adoption of exercise cause changes in NEAT?
A number of studies have been done to determine if NEAT changes during the initiation and adoption of regular exercise (Table 1). The acute effect of exercise (i.e. initiation) on non-Ex PA and NEAT has been studied in several studies. In a series of elegant studies, Stubbs et al. (61-63) studied the acute effects of different doses of exercise on EI, EE (measured using HR monitor), and energy balance over periods of 7-10 days. In two of these studies, TDEE tended to decrease over time when medium (1.6 MJ/d) and high (3.2-4.0 MJ/d) levels of exercise were performed (61, 62), suggesting that NEAT decreased. However, in the latter study, dietary fat intake was also increased, so it is possible that the compensation was partly due to the dietary manipulation. More recently, Alahamdi et al. (1) compared the effects of single session of exercise performed at two different intensities on non-Ex PA in overweight and obese men. Non-Ex PA remained unchanged for the first two days, but increased three days following the moderate- (16%, not significant) and high-intensity (25%) sessions. The reasons for this delayed increase are not clear, but similar results were previously observed in obese boys (36). In contrast, NEAT (estimated from HR and physical activity diaries) remained unchanged in a group of lean males and females participating in every other day moderate-intensity exercise training for eight days (48). Although a strength of these short-term studies is the within-subject design, they are limited by the short-term nature of the intervention. Longer term studies aimed at understanding the effects of exercise adaptation on NEAT, have also yielded equivocal results. Studies have shown reductions in non-Ex PA (12, 41, 49) and NEAT (13, 24, 49, 51) whereas other studies have reported no changes in NEAT during the training period (27, 71). It is difficult to reconcile these discrepant findings, but it is likely that differences in intensity and mode of exercise, the measurement tool used, and the age and sex of study participants were contributing factors. For example, it appears that older adults are more likely to exhibit compensatory changes in NEAT (24, 51) and non-Ex PA (50), although none of these studies compared younger to older adults. Moreover, since a variety of exercise intensities were employed, it is not possible to determine the independent effects of age and exercise intensity. A recent study in overweight adults suggested that reductions in NEAT were dose-dependent, with reductions occurring only in the group performing a high dose of exercise (600 kcal/d) but not in the group performing a moderate dose of exercise (300 kcal/d) (57). In contrast, no dose-response effect was observed in a secondary analysis in two large cohort studies that compared the effects of different doses of exercise on cardiovascular fitness and cardiovascular risk factors (10, 27). However, these studies were not specifically designed to determine if there is dose-response effect of exercise on NEAT.
Table 1.
Summary of experimental studies that directly measured total daily energy expenditure in responses to exercise
| Reference | N | Subjects | Duration | Days/ wk |
Intensity/duration | Measurement | Results |
|---|---|---|---|---|---|---|---|
| Goran and Poehler, 1992 [24] |
11 | NW/OW older men (56-78 y) |
8 weeks | 3 | 85% VO2 max, 300kcal/session |
DLW | Evidence for compensation, NEAT decreased by 62% (from 571 ± 386 to 340 ± 342 kcal/day) |
| Meijer et al., 1999 [48] |
22 | NW/OW older men and women (mean 58y) |
12 weeks | 2 | 60 and 90min, weight training and aerobic |
AM | Non-exercise activity significantly lower on training compared to non-training days |
| Donnelly et al., 2003 [13] |
74 | OW/OB men and women (17- 35y) |
16 months | 5 | 45 min, 75% HRR | DLW | Weight loss ~50% of predicted, suggests compensation |
| Manthou et al., 2010 [41] |
34 | OW/OB men and women (mean 31 y) |
8 weeks | 2 or 5 | 150 min/wk, 90-95% LT |
HR | Predicted fat loss 0.8 +/− 0.2 kg actual fat loss 0.0 +/− 0.2 kg, half of subjects compensated |
| Di Blasio et al. [12] |
34 | NW-OB post- menopausal women (mean 56 y) |
13 weeks | 4 | 40min, moderate walking |
AM | Half of sample compensated, on average no change in TDEE |
| Hollowell et al., 2009 [27] |
50 | OW/OB men and women (mean 53.2 yr) |
8 months | 3 to 5 times |
Low 5035Kj/wk at 65-80% or 40-55% VO2 peak; high 8372 KJ/wk 65-80% VO2 peak |
AM | Both groups significantly increased TDEE, no change in non-exercise activity |
| Morio et al, 1998 [50] |
13 | NW/OW men and women (63 ± 2 yrs) |
14 weeks | 3 | 40 min total, 20 min moderate, 20 min interval training |
Self-report diary | No change in TDEE, time walking decreased, energy expended during free living activities significantly decreased by 7.7% |
| Author | N | Subjects | Duration | Days/ wk |
Intensity/duration | Measurement | Results |
|---|---|---|---|---|---|---|---|
| Alahmadi et. al. 2011 [1] |
16 | OW/OB males (mean 26.5 y) |
4 days | 1 | 60 min; mod | AM | No evidence for compensation, increase in TDEE |
| McLaughlin et al. [47] |
16 | NW men and women (20-25y) |
8 days | 4 | 2092 kJ; 59% VO2 max in females and 48% VO2 max in males |
HR | No evidence for compensation, increase in TDEE and non- exercise activity |
| Stubbs et.al [60] |
8 | NW men (18- 40y) |
7 days | 7 | 3, 40-min exercise sessions per day at 65% VO2 max |
HR | Evidence for compensation 0.32 MJ/day (or 2.2 MJ/wk) |
| Stubbs et al., 2002 [62] |
6 | NW women (18- 40y) |
7 days | 6 | Mod-two 40 min exercise sessions per day; high- 3, 40 40- min exercise sessions per day |
HR | No evidence for compensation, increase in TDEE and non- exercise activity |
| Stubbs et al., 2002 [61] |
6 | NM men (18- 40y) |
7 days | 6 | Mod: two 40 min exercise sessions per day; high: three 40 min exercise sessions per day |
HR | Evidence of modest compensation 0.3-0.6Mj/day |
| Westerterp et al., 1992 [70] |
32 | NW men and women, 28-41 y |
10 months | 4 | Half-marathon training, vigorous intensity, progressive increase to 90 min/day |
DLW | No evidence for compensation, increase in TDEE |
Note: NW is normal weight, OW is overweight, OB is obese. DLW is double labeled water, HR is heart rate, HRR is heart rate reserve, AM is activity monitor, NEAT is Non-exercise activity thermogenesis. TDEE is total daily energy expenditure, Values are mean ± SD unless otherwise indicated.
The majority of the early studies in this area have based their conclusions on mean data. As discussed above, there is large individual variability in the magnitude and even the direction of weight lost as a result of exercise training. Recent evidence suggests there are individual differences in compensatory responses that may have important implications for weight loss and other important disease risk factors. Manthou et al. (42) measured NEAT using HR and diaries in overweight and obese women who completed an 8-week exercise intervention. On average, the group increased TDEE by 0.62 MJ/day. However, there were large individual differences in weight loss. They classified 11 individuals as ‘responders’ (those who lost as much weight as predicted) and 23 individuals as ‘non-responders’ (those who lost less weight than predicted). NEAT was the only variable that was significantly different between groups.
Previous studies have reported individual variability in weight loss but this was the first to demonstrate that changes in NEAT are associated with changes in body weight. Furthermore, change in NEAT was a significant predictor in fat mass in the group as a whole. Similarly, Di Blasio et al. (12) reported that half of the post-menopausal women who started training were compensators, decreasing NEAT by an average 233 kcal/day. In this study, those who decreased NEAT did not have improvements in blood lipids, suggesting behavioral compensation may have implications for changes in health outcomes as well as weight loss. These two recent studies illustrate an important shift from a group-based approach to an individual-level analysis. By considering individual difference in compensation, intervention strategies to reduce compensation and maximize weight loss strategies can be developed. Nonetheless, the results of these studies both demonstrate that on a group level, the trend was for non-EX PA to decrease.
Do changes in NEAT offset exercise EE during weight loss?
There is evidence that caloric restriction, without exercise, induces compensatory changes in non-EX PA and NEAT that can offset intended weight loss. The best evidence comes from a study in monkeys (64). In that study, when EI was decreased by 30% in the first month, the decrease in SPA was substantial enough that no significant decrease in body weight occurred. In the second month, when EI was decreased by 60%, significant weight loss occurred (−6.4 ± 1.7%), but further suppression of SPA was also observed. A similar effect has been observed in humans in the CALERIE study (43); NEAT, decreased in the caloric restriction groups. However, because there were no changes in physical activity measured with accelerometry, the authors concluded that the decreases in AEE were due to increased muscle efficiency or decreased “fidgeting”.
The evidence that exercise, without caloric restriction, induces compensatory changes in NEAT, is not as strong. Evidence can only be obtained from studies where either EI was controlled, or measured intake did not change. The strongest evidence can be found in studies conducted by Donnelly et al. (13, 16). In the first Midwest Exercise Trial (MET-1), the intervention produced weight loss in men (−5.2±4.7 kg), but not women (13). There were no changes in measured EI during the intervention. At 16 months, EXEE was 668±116 kcal/d in men and 438.9±88 kcal/d in women, but TDEE (DLW) increased only by 371±646 and 209±555 kcal/day in men and women, respectively. TDEE increased by approximately 55% of EXEE in men and 48% of EXEE in women. In the 2nd Midwest Exercise Trial (MET-2) conducted by the same group, EXEE was matched between men and women, and there were no differences in the change in TDEE (16). Thus, it does not appear that there were important sex differences in the degree of compensation. Additional evidence of the effects of exercise without caloric restriction on NEAT comes from the study of Tremblay et al. (67). Subjects were resident for a 12 week exercise intervention, and EI was held constant, at baseline levels. Change in body energy stores during the 2nd half of the intervention was only 65% of the energy deficit. However, it is not possible to conclude that decreases in NEAT occurred, because TDEE was not measured, but also because a reduction in RMR was also observed. Conversely, analysis of the carefully controlled studies performed by Ross et al. (28, 59) demonstrated that the estimated energy imbalance induced by exercise was not significantly different from the prescribed EXEE, suggesting that NEAT was preserved (66). However, there are several limitations to this approach. First, it cannot be determined to what degree changes in both EE and EI contributed to the estimated energy imbalance. Second, errors in body composition are incorporated in this calculation, and the changes in NEAT may be within the bounds of error and thus beyond detection, but still of great enough magnitude to have a meaningful effect on body weight (26). These examples illustrate the pitfalls of attempting to assess the degree of exercise compensation without accurate measurement of the individual components of EE.
When the magnitude of observed weight loss is less than the expected weight loss, this is often interpreted as evidence of compensation in non-Ex PA and NEAT (13). It is worth noting that in every study we reviewed, the expected weight loss was calculated using the “3500 kcal/lb body weight rule”, i.e. an energy deficit of 3500 kcals will induce a weight loss of 1 lb of body weight, which is based on the calculated energy content of body composition (70:30 FM:FFM) (74). However, a limitation to this static approach is that it erroneously predicts a linear change in body weight over time. Moreover, this model was derived from data obtained in short-term, low calorie diets, and thus, is not directly applicable to changes in energy stores induced by exercise. As elegantly illustrated by Hall (25), the rate of weight change over time will slow over time due to compensatory changes in EE, and that it assumes that all people lose weight at a fixed ratio of 70:30 FM:FFM. Thus, the expected weight loss based on the “3500 kcal” rule is likely an overestimate of the true theoretical weight loss.
From the above discussion, it is clear that more sophisticated studies are required to more completely understand the effects of exercise, prescribed for weight loss, on non-exercise physical activity. Such studies should encompass the simultaneous measurement of EI and EE, including all components of EE, objective measurement of physical activity, and accurate measurement of changes in body energy stores. There several outstanding questions related to how exercise modifies non-exercise physical activity. To our knowledge, studies examining the effects of type (endurance versus resistance), mode (swimming, cycling, or running) or intensity of exercise on non-Ex PA and NEAT (or EI) have not been performed. As discussed above, the effects of age, sex, and obesity have not been well-studied. Finally, given the equivocal findings from both acute and chronic studies, it is not possible to draw conclusions about differences in compensation that may occur during the initiation and adaption to exercise. Thus, more studies are needed to determine the effects of these potentially important factors on non-EX PA and NEAT.
EFECTS OF EXERCISE ON ENERGY AND MACRONUTRIENT INTAKE
Compensatory increases in EI are thought to be at least partially responsible for the small magnitude of mean weight loss induced by aerobic exercise training without energy restriction (66). For example, King et al. (31, 32) have demonstrated significant increases in EI among participants who did not reduce weight or fat mass in response to aerobic exercise training (12 wks., 5 d/wk., 500 kcal/session, 70% max HR). However, evidence for an effect of exercise on EI or macronutrient composition is not compelling. Acute exercise has been shown to have no effect (33, 34, 39, 45) or result in only partial compensatory increases in EI following a bout of acute exercise (54, 61, 73). The majority of studies in this area have shown no change in EI or macronutrient intake in response to aerobic exercise training (2, 8, 11, 13, 14, 16, 44, 55, 60). However, the literature on change in EI and macronutrient intake in response to exercise training should be interpreted cautiously. EI typically has been assessed by self-reported 3 or 7-day food records which have been demonstrated to underestimate EI when compared with energy expenditure assessed by DLW (2). For example, Donnelly et al. (16) compared EI measured by DLW and diet records, and found under-reporting for diet records of 20 to 30%. Advanced technology can reduce this error considerably. For example, In MET 2 (described below) EI and macronutrient content was assessed across 10 months during 1 week periods at 4 time points with ad libitum eating at the University of Kansas Cafeteria (16). Digital photographs were obtained before and after consumption and the type and quantity of foods and beverages were quantified by trained research staff. Food and beverages consumed outside the cafeteria were assessed using multiple pass 24-hour recall procedures using food models and standardized, neutral probing questions. These procedures reduced error of EI compared to DLW to ~ 3%.
Data from the MET-2 afforded a unique opportunity not only to examine the effect of exercise training but also examine if a dose effect existed at 2 levels of EE and if there were gender differences for energy and macronutrient intake in a sample of previously sedentary, overweight/obese young adults. Moreover, data for individual variation for weight loss and energy intake were available. A detailed description of the design and methods for MET-2 has been previously published (16). Briefly, MET-2 randomized 141 young adults age 18-30 years, BMI 25-40 kg/m2 to a 10 month, 5 day/week supervised exercise intervention at 2 levels of EXEE (400 or 600 kcal/session) or a non-exercise control group. All participants continued their typical patterns of daily physical activity and dietary intake over the duration of the 10 month intervention.
Exercise consisted primarily of walking/jogging on motor-driven treadmills, and was supervised by trained research staff in a dedicated exercise facility. The exercise protocol gradually increased EXEE from baseline to the end of month 3 and then remained at 400 or 600 kcal/session for the remainder of the study, as previously described (16).
Compliance to the exercise protocol, an essential element of an efficacy study, was defined as successfully completing > 90% of scheduled exercise sessions defined as maintaining the target exercise HR±4 beats/minute for the prescribed duration of the exercise session. Participants who were non-compliant during any 3 month interval (months 0-3, 3-6, 6-9) or during the final month (month 10) were dismissed from the study. Participants assigned to the non-exercise control group were instructed to continue their typical patterns for physical activity and dietary intake over the duration of the 10 month study. With the exception of assessment of EXEE, the same outcome assessments were completed with both the exercise and control groups.
Ninety-two of the 141 participants randomized at baseline (65.2%) complied with the study protocol and completed all outcome assessments. There were no significant between group differences in EI (kcal/d) at baseline. During the exercise intervention EI was 121 kcal/day (4.5%) and 285 kcal/day (10.7%) higher in the 400 and 600 kcal/session compared with control; however these differences were not significant. Across the duration of the intervention, there were no significant changes for macronutrients for the 400 or 600 kcal/session groups. The control group had significant decreases in percentage and grams of fat. When EI and macronutrients were analyzed by gender, no significant differences were found for men between groups and no significant changes were found across the duration of the intervention. Significant differences for were found in women for EI during the intervention. Control women decreased EI by an average of 352 kcal/d compared to women in the 600 kcal/session group who decreased by an average of 45 kcal/d (p<0.05). Control women had a significant increase in percentage of carbohydrate (4.0%) and significant decrease in percentage of fat (4.2%) across the duration of the study.
Despite the supervision of exercise and tight control of EXEE, wide variation was shown for weight loss (Figure 1) suggesting compensation in components of energy balance. EI may be the largest source for compensation and the individual differences for change across the intervention were considerable. The individual variation for EI may diminish weight loss and thus the impact of exercise alone as a primary weight loss strategy. These individuals may be considered “non-responders” with respect to exercise for weight loss and if identified early during a weight loss program may represent and opportunity for more targeted interventions using diet counseling or energy restriction.
What are the causes of variability?
There are a range of behavioral (increased food intake, decreased activity, non-compliance with the exercise) and metabolic (decrease in resting metabolic rate) adaptations that could occur in response to increased EXEE. However, there is strong evidence to suggest that over-eating is a pernicious and potent contributor to weight gain and obesity (4). Therefore, increases in EI are likely a strong contributing factor to the modest weight loss often observed in exercise interventions. The processes underpinning any compensation in EI need to be better understood.
What are the drivers of exercise-induced compensatory eating?
With respect to biological needs and energy balance regulation, homeostatic processes of appetite control are associated with changes in the orexigenic drive to eat (e.g. hunger), whereas hedonic processes are associated with reward and the pleasure of eating. Individuals who are more susceptible to exercise-induced compensation could be characterized by an enhanced hunger (homeostatic processes) or hyper-responsivity to the pleasurable components of food (hedonic processes), or both.
Homeostatic Processes
It is important to determine how the homeostatic processes of satiation and satiety are adjusted in response to increased EXEE. Blundell and colleagues at the University of Leeds in the UK have demonstrated that exercise can be used as a tool to better understand appetite regulation. The researchers used a 12-week supervised exercise intervention model to characterize the drivers of compensatory eating (9, 30, 31). The exercise intervention consisted of 5 moderately-high-intensity (70% VO2max) exercise sessions per week, with fixed intensity and duration for all individuals. The EE of each exercise session was approximately 2 MJ. An assay of appetite measures was used to objectively monitor EI and appetite sensations in the research unit. On each test day, following a fixed breakfast, participants were provided with ad libitum lunch and dinner test meals and an evening snack box, each separated by 4 hours. This methodological platform and approach is based on a number of conceptual principles and is designed to provide a comprehensive and flexible model for the study of EE and EI. Key features of the approach are that the exercise is supervised, and the measurements of EI and appetite are conducted under carefully controlled conditions. Blundell’s 12-week exercise intervention serves as an ideal model of resistance to weight loss, and provides an opportunity to help explain why exercise doesn’t work for everyone.
The series of studies by Blundell et al. revealed that 12 weeks of exercise exerted different effects on fasting and postprandial appetite sensations. Compensators (i.e. non-responders) were defined as losing less weight after the exercise intervention than non-compensators (i.e., responders). Compared to their own baseline, compensators experienced marked and significant increases in EI and fasting hunger in response to the exercise intervention (Figure 3). However, both compensators and non-compensators experienced an increase in satiety immediately after the fixed breakfast meal (Figure 4). This dual response effect demonstrates that while some people might experience an orexigenic response to supervised exercise, exercise also has the capacity to improve satiety.
Figure 3.
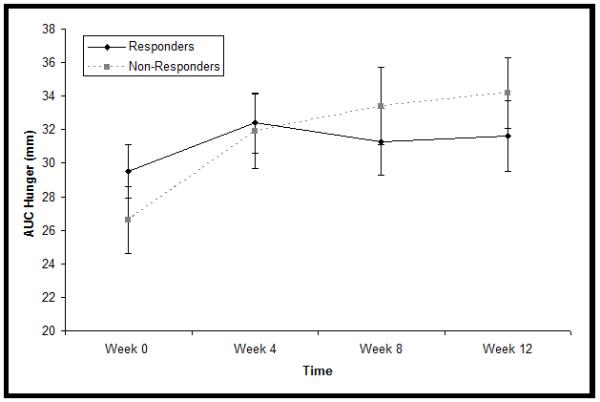
Area Under the Curve (AUC) Hunger for Responders (non-compensator) and non-responders (compensators). Adopted from (30).
Figure 4.
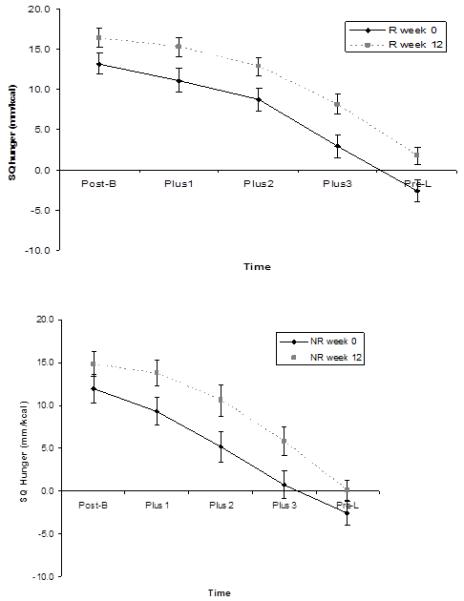
Satiety Quotient (SQ) responses during the post-prandial period for (a) Responders R, non-compensators) and (b) Non-Responders (NR, compensators) at baseline (Week 0) and at 12 weeks of exercise (12 week). Adopted from (30).
Hedonic Processes
The hedonic aspects of food (e.g. the pleasure of eating) also influences appetite control (3). Reward plays an important role in the initiation, maintenance and cessation of eating. Therefore it is plausible that changes in food and macronutrient preferences might contribute to compensatory increases in EI (17).
Finlayson has worked extensively on the theoretical and methodological understanding of behavior related to ‘liking’ and ‘wanting’ food in humans to develop a novel methodology to detect changes or differences in ‘liking’ and ‘wanting’ hedonic responses (21, 22). This procedure was used to demonstrate that individuals identified as compensators because they exhibit an acute compensatory increase in food intake after a single bout of exercise, also experience a significant exercise-induced increase in hedonic preference for a range of foods (19). The Liking and Wanting procedure was also used in the 12-week exercise intervention to assess changes in taste and nutrient preferences under more chronic energy balance conditions. Those who experienced an immediate post-exercise increase in liking for food in general, and an increased wanting for high-fat sweet foods also experienced less weight loss (20). Interestingly, this response to acute exercise was not influenced by chronic exercise. Therefore it is possible that some people are more vulnerable to the acute effects of exercise on reward. An enhanced motivational drive or wanting for food after exercise may help to explain why some people over-compensate when given access to food after exercise.
What are the potential homeostatic and non-homeostatic mechanisms underpinning compensation?
Obvious homeostatics candidates include the peptides strongly associated with appetite regulation. For example, orexigenic peptides such as Ghrelin and anorectic peptides such as GLP-1 could partly explain some of the homeostatic and hedonic responses to exercise-induced EE (45). There is evidence that non-homeostatic factors are associated with changes in food intake responses to exercise (7) such that individuals with a high level of disinhibition are more susceptible to overcompensate for the EXEE (68). Individuals who are identified as compensators - hence experience lower weight loss compared to non-compensators - could be characterized by a portfolio of homeostatic and/or non-homeostatic characteristics that partially explain the resistance.
IMPLICATIONS: HOW CAN THE EVIDENCE BE USED TO IMPROVE THE EFFECTIVENESS OF WEIGHT MANAGEMENT STRATEGIES?
Unless there is a better understanding of why some people fail to lose weight with exercise, the increase in the prevalence of obesity and the associated co-morbidities will be unmanageable and unsustainable. Although we acknowledge that people aspire to unrealistically high rates of weight loss, it is futile to continue prescribing exercise and/or dietary interventions using a one-size-fits-all approach, and expect people to be content when their efforts produce little or no weight loss. The evidence is suggestive, but not conclusive, that when initiating an exercise program with the intent of losing weight, some individuals compensate by decreasing their non-Ex PA and NEAT. This is likely mediated by subject factors (e.g. age, sex, body weight) as well as factors related to the exercise program itself (mode, duration, intensity, frequency), but how each of these factors contribute to the overall effect has not been well-studied. Surprisingly, some data suggest that there are individuals who respond to an exercise program by increasing their non-Ex PA and NEAT. Understanding how exercise impacts non-Ex PA has health implications far-beyond regulating energy balance, as evidence suggests that limiting sedentary behavior has positive effects on many health outcomes, independent of exercise (52). Moreover, it is not clear from the existent literature, when compensation occurs, whether this is intentional (i.e. “I exercised today, so I will take the elevator”) or not. Clearly, there is much more to be learned in this area.
The evidence also suggests that a compensatory increase in EI could also account for variability and offset the expected weight loss. Preliminary evidence suggests that some people experience an orexigenic response to exercise, making them more resistant to exercise-induced weight loss. The potential underlying mechanisms underpinning this compensatory response include appetite peptide response and non-homeostatic eating behavior traits. Collectively, the evidence indicates that compensatory adaptive responses in EI and NEAT offset the effects of exercise and result in some individuals achieving little or no weight loss. However, to our knowledge, compensatory changes in non-EX PA and EI have not been comprehensively examined within the same study, and this is a high priority for future research. The model of resistance to exercise-induced weight loss needs to be used strategically in future studies. Identifying the resistance to weight loss, and characterizing the adaptive compensatory responses will produce better strategies on how to individually tailor weight management programs. Indeed, energy restriction studies can also benefit from this approach.
Although a compensatory increase in food intake is disappointing to the people directly affected, it serves as an ideal model of resistance to weight loss, and provides an opportunity to help explain why exercise doesn’t work for everyone. It could also be used to inform strategies to help obese individuals who may avoid exercise based on their experience of disappointing weight loss. We propose that it is possible to pool the current evidence and use it strategically in the form of evidence-based screening procedures to identify resistance to weight loss due to a compensatory increase in food intake. This approach is novel because it targets resistance to weight loss and individuals susceptible to compensation during exercise interventions. Identification and characterization of behavioral and physiological characteristics will provide evidence-based screening information that will facilitate the identification of individuals vulnerable to compensation and resistant to weight loss. Early identification of weight loss resistance will eventually permit tailoring of obesity prevention and treatment strategies to suit individuals who are more susceptible to compensatory eating. We also need to better educate people that weight loss is not the only health benefit of exercising. Indeed, there is strong evidence that people experience other health benefits (e.g., reduced blood pressure and waist circumference) despite not attaining the expected, or any, weight loss (32). Our concern is that efforts to increase physical activity amongst the general population have been undercut by negative media reports portraying exercise as ineffective for weight loss, which may be interpreted by some as therefore ineffective for improving health. We all have a responsibility to eradicate this ‘bad spin’, and to educate the public that weight loss is not the sole benefit of exercising; indeed, people can experience health benefits in the absence of weight loss (32).
Acknowledgements
The authors wish to acknowledge the contributions of their respective laboratory members and colleagues who made the presentation of these data and ideas possible, including The Biopsychology Group, University of Leeds, UK. In addition, the authors wish to thank Audrey Bergouignan for her thoughtful comments during the preparation of this manuscript. The authors also wish to acknowledge all of the outstanding work in this area that could not be included due to space limitations.
Work related to this symposium was supported by the following grants: NIH DK07708 and UL1 RR025780 (Dr. Melanson); NIH RC1HL099557 (Drs. Kozey Keadle and Dr. Barry Braun), and NIH DK49191 (Dr. Donnelly).
Footnotes
Conflicts of interest: The authors have not conflicts of interest to declare.
The work presented in this manuscript don not constitute and endorsement by ACSM.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
REFERENCES
- 1.Alahmadi MA, Hills AP, King NA, Byrne NM. Exercise intensity influences nonexercise activity thermogenesis in overweight and obese adults. Medicine and science in sports and exercise. 2011;43(4):624–31. doi: 10.1249/MSS.0b013e3181f7a0cb. [DOI] [PubMed] [Google Scholar]
- 2.Ambler C, Eliakim A, Brasel JA, Lee WN, Burke G, Cooper DM. Fitness and the effect of exercise training on the dietary intake of healthy adolescents. Int J Obes Relat Metab Disord. 1998;22(4):354–62. doi: 10.1038/sj.ijo.0800595. [DOI] [PubMed] [Google Scholar]
- 3.Berthoud HR. Neural control of appetite: cross-talk between homeostatic and non-homeostatic systems. Appetite. 2004;43(3):315–7. doi: 10.1016/j.appet.2004.04.009. [DOI] [PubMed] [Google Scholar]
- 4.Blundell JE. Exercuse makes you fat - what’s going on? Nutrition Bulletin. 2009;34:380–2. [Google Scholar]
- 5.Bouchard C, Tremblay A, Despres JP, Nadeau A, Lupien PJ, Theriault G, et al. The response to long-term overfeeding in identical twins. N Engl J Med. 1990;322(21):1477–82. doi: 10.1056/NEJM199005243222101. [DOI] [PubMed] [Google Scholar]
- 6.Bouchard C, Tremblay A, Despres JP, Theriault G, Nadeau A, Lupien PJ, et al. The response to exercise with constant energy intake in identical twins. Obesity research. 1994;2(5):400–10. doi: 10.1002/j.1550-8528.1994.tb00087.x. [DOI] [PubMed] [Google Scholar]
- 7.Bryant EJ, King NA, Blundell JE. Disinhibition: its effects on appetite and weight regulation. Obesity reviews : an official journal of the International Association for the Study of Obesity. 2008;9(5):409–19. doi: 10.1111/j.1467-789X.2007.00426.x. [DOI] [PubMed] [Google Scholar]
- 8.Bryner RW, Toffle RC, Ullrich IH, Yeater RA. The effects of exercise intensity on body composition, weight loss, and dietary composition in women. Journal of the American College of Nutrition. 1997;16(1):68–73. doi: 10.1080/07315724.1997.10718651. [DOI] [PubMed] [Google Scholar]
- 9.Caudwell P, Hopkins M, King NA, Stubbs RJ, Blundell JE. Exercise alone is not enough: weight loss also needs a healthy (Mediterranean) diet? Public health nutrition. 2009;12(9A):1663–6. doi: 10.1017/S1368980009990528. [DOI] [PubMed] [Google Scholar]
- 10.Church TS, Martin CK, Thompson AM, Earnest CP, Mikus CR, Blair SN. Changes in weight, waist circumference and compensatory responses with different doses of exercise among sedentary, overweight postmenopausal women. PLoS One. 2009;4(2):e4515. doi: 10.1371/journal.pone.0004515. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Cox KL, Gorely TJ, Puddey IB, Burke V, Beilin LJ. Exercise behaviour change in 40 to 65-year-old women: The SWEAT Study (Sedentary Women Exercise Adherence Trial) British journal of health psychology. 2003;8(Pt 4):477–95. doi: 10.1348/135910703770238329. [DOI] [PubMed] [Google Scholar]
- 12.Di Blasio A, Ripari P, Bucci I, Di Donato F, Izzicupo P, D’Angelo E, et al. Walking training in postmenopause: effects on both spontaneous physical activity and training-induced body adaptations. Menopause. 2012;19(1):23–32. doi: 10.1097/gme.0b013e318223e6b3. [DOI] [PubMed] [Google Scholar]
- 13.Donnelly JE, Hill JO, Jacobsen DJ, Potteiger J, Sullivan DK, Johnson SL, et al. Effects of a 16-month randomized controlled exercise trial on body weight and composition in young, overweight men and women: the Midwest Exercise Trial. Arch Intern Med. 2003;163(11):1343–50. doi: 10.1001/archinte.163.11.1343. [DOI] [PubMed] [Google Scholar]
- 14.Donnelly JE, Jacobsen DJ, Heelan KS, Seip R, Smith S. The effects of 18 months of intermittent vs. continuous exercise on aerobic capacity, body weight and composition, and metabolic fitness in previously sedentary, moderately obese females. Int J Obes Relat Metab Disord. 2000;24(5):566–72. doi: 10.1038/sj.ijo.0801198. [DOI] [PubMed] [Google Scholar]
- 15.Donnelly JE, Smith BK. Is exercise effective for weight loss with ad libitum diet? Energy balance, compensation, and gender differences. Exercise and sport sciences reviews. 2005;33(4):169–74. doi: 10.1097/00003677-200510000-00004. [DOI] [PubMed] [Google Scholar]
- 16.Donnelly JE, Washburn RA, Smith BK, Sullivan DK, Gibson C, Honas JJ, et al. A randomized, controlled, supervised, exercise trial in young overweight men and women: the Midwest Exercise Trial II (MET2) Contemporary clinical trials. 2012;33(4):804–10. doi: 10.1016/j.cct.2012.03.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Elder SJ, Roberts SB. The effects of exercise on food intake and body fatness: a summary of published studies. Nutrition reviews. 2007;65(1):1–19. doi: 10.1111/j.1753-4887.2007.tb00263.x. [DOI] [PubMed] [Google Scholar]
- 18.Esparza J, Fox C, Harper IT, Bennett PH, Schulz LO, Valencia ME, et al. Daily energy expenditure in Mexican and USA Pima indians: low physical activity as a possible cause of obesity. Int J Obes Relat Metab Disord. 2000;24(1):55–9. doi: 10.1038/sj.ijo.0801085. [DOI] [PubMed] [Google Scholar]
- 19.Finlayson G, Bryant E, Blundell JE, King NA. Acute compensatory eating following exercise is associated with implicit hedonic wanting for food. Physiology & behavior. 2009;97(1):62–7. doi: 10.1016/j.physbeh.2009.02.002. [DOI] [PubMed] [Google Scholar]
- 20.Finlayson G, Caudwell P, Gibbons C, Hopkins M, King N, Blundell J. Low fat loss response after medium-term supervised exercise in obese is associated with exercise-induced increase in food reward. Journal of obesity. 2011 doi: 10.1155/2011/615624. 2011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Finlayson G, King N, Blundell J. The role of implicit wanting in relation to explicit liking and wanting for food: implications for appetite control. Appetite. 2008;50(1):120–7. doi: 10.1016/j.appet.2007.06.007. [DOI] [PubMed] [Google Scholar]
- 22.Finlayson G, King N, Blundell JE. Is it possible to dissociate ‘liking’ and ‘wanting’ for foods in humans? A novel experimental procedure. Physiology & behavior. 2007;90(1):36–42. doi: 10.1016/j.physbeh.2006.08.020. [DOI] [PubMed] [Google Scholar]
- 23.Garland T, Jr., Schutz H, Chappell MA, Keeney BK, Meek TH, Copes LE, et al. The biological control of voluntary exercise, spontaneous physical activity and daily energy expenditure in relation to obesity: human and rodent perspectives. The Journal of experimental biology. 2011;214(Pt 2):206–29. doi: 10.1242/jeb.048397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Goran MI, Poehlman ET. Endurance training does not enhance total energy expenditure in healthy elderly persons. The American journal of physiology. 1992;263(5 Pt 1):E950–7. doi: 10.1152/ajpendo.1992.263.5.E950. [DOI] [PubMed] [Google Scholar]
- 25.Hall KD, Sacks G, Chandramohan D, Chow CC, Wang YC, Gortmaker SL, et al. Quantification of the effect of energy imbalance on bodyweight. Lancet. 2011;378(9793):826–37. doi: 10.1016/S0140-6736(11)60812-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Hill JO, Wyatt HR, Reed GW, Peters JC. Obesity and the environment: where do we go from here? Science. 2003;299(5608):853–5. doi: 10.1126/science.1079857. [DOI] [PubMed] [Google Scholar]
- 27.Hollowell RP, Willis LH, Slentz CA, Topping JD, Bhakpar M, Kraus WE. Effects of exercise training amount on physical activity energy expenditure. Medicine and science in sports and exercise. 2009;41(8):1640–4. doi: 10.1249/MSS.0b013e31819c71a4. [DOI] [PubMed] [Google Scholar]
- 28.Janssen I, Fortier A, Hudson R, Ross R. Effects of an energy-restrictive diet with or without exercise on abdominal fat, intermuscular fat, and metabolic risk factors in obese women. Diabetes Care. 2002;25(3):431–8. doi: 10.2337/diacare.25.3.431. [DOI] [PubMed] [Google Scholar]
- 29.Joosen AM, Gielen M, Vlietinck R, Westerterp KR. Genetic analysis of physical activity in twins. The American journal of clinical nutrition. 2005;82(6):1253–9. doi: 10.1093/ajcn/82.6.1253. [DOI] [PubMed] [Google Scholar]
- 30.King NA, Caudwell PP, Hopkins M, Stubbs JR, Naslund E, Blundell JE. Dual-process action of exercise on appetite control: increase in orexigenic drive but improvement in meal-induced satiety. The American journal of clinical nutrition. 2009;90(4):921–7. doi: 10.3945/ajcn.2009.27706. [DOI] [PubMed] [Google Scholar]
- 31.King NA, Hopkins M, Caudwell P, Stubbs RJ, Blundell JE. Individual variability following 12 weeks of supervised exercise: identification and characterization of compensation for exercise-induced weight loss. Int J Obes (Lond) 2008;32(1):177–84. doi: 10.1038/sj.ijo.0803712. [DOI] [PubMed] [Google Scholar]
- 32.King NA, Hopkins M, Caudwell P, Stubbs RJ, Blundell JE. Beneficial effects of exercise: shifting the focus from body weight to other markers of health. British journal of sports medicine. 2009;43(12):924–7. doi: 10.1136/bjsm.2009.065557. [DOI] [PubMed] [Google Scholar]
- 33.King NA, Horner K, Hills AP, Byrne NM, Wood RE, Bryant E, et al. Exercise, appetite and weight management: understanding the compensatory responses in eating behaviour and how they contribute to variability in exercise-induced weight loss. British journal of sports medicine. 2012;46(5):315–22. doi: 10.1136/bjsm.2010.082495. [DOI] [PubMed] [Google Scholar]
- 34.King NA, Tremblay A, Blundell JE. Effects of exercise on appetite control: implications for energy balance. Medicine and science in sports and exercise. 1997;29(8):1076–89. doi: 10.1097/00005768-199708000-00014. [DOI] [PubMed] [Google Scholar]
- 35.Kotz CM, Levine JA. Role of nonexercise activity thermogenesis (NEAT) in obesity. Minnesota medicine. 2005;88(9):54–7. [PubMed] [Google Scholar]
- 36.Kriemler S, Hebestreit H, Mikami S, Bar-Or T, Ayub BV, Bar-Or O. Impact of a single exercise bout on energy expenditure and spontaneous physical activity of obese boys. Pediatric research. 1999;46(1):40–4. doi: 10.1203/00006450-199907000-00007. [DOI] [PubMed] [Google Scholar]
- 37.Levine JA. Non-exercise activity thermogenesis. The Proceedings of the Nutrition Society. 2003;62(3):667–79. doi: 10.1079/PNS2003281. [DOI] [PubMed] [Google Scholar]
- 38.Levine JA, Eberhardt NL, Jensen MD. Role of nonexercise activity thermogenesis in resistance to fat gain in humans. Science. 1999;283(5399):212–4. doi: 10.1126/science.283.5399.212. [DOI] [PubMed] [Google Scholar]
- 39.Lluch A, King NA, Blundell JE. No energy compensation at the meal following exercise in dietary restrained and unrestrained women. Br J Nutr. 2000;84(2):219–25. [PubMed] [Google Scholar]
- 40.Luke A, Dugas LR, Ebersole K, Durazo-Arvizu RA, Cao G, Schoeller DA, et al. Energy expenditure does not predict weight change in either Nigerian or African American women. The American journal of clinical nutrition. 2009;89(1):169–76. doi: 10.3945/ajcn.2008.26630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Manthou E, Gill JM, Wright A, Malkova D. Behavioral compensatory adjustments to exercise training in overweight women. Medicine and science in sports and exercise. 2009;42(6):1121–8. doi: 10.1249/MSS.0b013e3181c524b7. [DOI] [PubMed] [Google Scholar]
- 42.Manthou E, Gill JM, Wright A, Malkova D. Behavioral compensatory adjustments to exercise training in overweight women. Med Sci Sports Exerc. 2010;42(6):1121–8. doi: 10.1249/MSS.0b013e3181c524b7. [DOI] [PubMed] [Google Scholar]
- 43.Martin CK, Das SK, Lindblad L, Racette SB, McCrory MA, Weiss EP, et al. Effect of calorie restriction on the free-living physical activity levels of nonobese humans: results of three randomized trials. J Appl Physiol. 2011;110(4):956–63. doi: 10.1152/japplphysiol.00846.2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Martins C, Kulseng B, King NA, Holst JJ, Blundell JE. The effects of exercise-induced weight loss on appetite-related peptides and motivation to eat. The Journal of clinical endocrinology and metabolism. 2010;95(4):1609–16. doi: 10.1210/jc.2009-2082. [DOI] [PubMed] [Google Scholar]
- 45.Martins C, Morgan LM, Bloom SR, Robertson MD. Effects of exercise on gut peptides, energy intake and appetite. The Journal of endocrinology. 2007;193(2):251–8. doi: 10.1677/JOE-06-0030. [DOI] [PubMed] [Google Scholar]
- 46.McGuire KA, Ross R. Incidental physical activity is positively associated with cardiorespiratory fitness. Medicine and science in sports and exercise. 2011;43(11):2189–94. doi: 10.1249/MSS.0b013e31821e4ff2. [DOI] [PubMed] [Google Scholar]
- 47.McGuire KA, Ross R. Incidental physical activity and sedentary behavior are not associated with abdominal adipose tissue in inactive adults. Obesity (Silver Spring) 2012;20(3):576–82. doi: 10.1038/oby.2011.278. [DOI] [PubMed] [Google Scholar]
- 48.McLaughlin R, Malkova D, Nimmo MA. Spontaneous activity responses to exercise in males and females. European journal of clinical nutrition. 2006;60(9):1055–61. doi: 10.1038/sj.ejcn.1602417. [DOI] [PubMed] [Google Scholar]
- 49.Meijer EP, Westerterp KR, Verstappen FT. Effect of exercise training on total daily physical activity in elderly humans. Eur J Appl Physiol Occup Physiol. 1999;80(1):16–21. doi: 10.1007/s004210050552. [DOI] [PubMed] [Google Scholar]
- 50.Meijer GA, Janssen GM, Westerterp KR, Verhoeven F, Saris WH, ten Hoor F. The effect of a 5-month endurance-training programme on physical activity: evidence for a sex-difference in the metabolic response to exercise. Eur J Appl Physiol Occup Physiol. 1991;62(1):11–7. doi: 10.1007/BF00635626. [DOI] [PubMed] [Google Scholar]
- 51.Morio B, Montaurier C, Pickering G, Ritz P, Fellmann N, Coudert J, et al. Effects of 14 weeks of progressive endurance training on energy expenditure in elderly people. Br J Nutr. 1998;80(6):511–9. doi: 10.1017/s0007114598001603. [DOI] [PubMed] [Google Scholar]
- 52.Owen N, Healy GN, Matthews CE, Dunstan DW. Too much sitting: the population health science of sedentary behavior. Exercise and sport sciences reviews. 2010;38(3):105–13. doi: 10.1097/JES.0b013e3181e373a2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Poehlman ET, Tremblay A, Despres JP, Fontaine E, Perusse L, Theriault G, et al. Genotype-controlled changes in body composition and fat morphology following overfeeding in twins. The American journal of clinical nutrition. 1986;43(5):723–31. doi: 10.1093/ajcn/43.5.723. [DOI] [PubMed] [Google Scholar]
- 54.Pomerleau M, Imbeault P, Parker T, Doucet E. Effects of exercise intensity on food intake and appetite in women. The American journal of clinical nutrition. 2004;80(5):1230–6. doi: 10.1093/ajcn/80.5.1230. [DOI] [PubMed] [Google Scholar]
- 55.Pritchard JE, Nowson CA, Wark JD. A worksite program for overweight middle-aged men achieves lesser weight loss with exercise than with dietary change. Journal of the American Dietetic Association. 1997;97(1):37–42. doi: 10.1016/S0002-8223(97)00015-1. [DOI] [PubMed] [Google Scholar]
- 56.Ravussin E, Lillioja S, Anderson TE, Christin L, Bogardus C. Determinants of 24-hour energy expenditure in man. Methods and results using a respiratory chamber. The Journal of clinical investigation. 1986;78(6):1568–78. doi: 10.1172/JCI112749. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Rosenkilde M, Auerbach PL, Reichkendler MH, Ploug T, Stallknecht BM, Sjodin A. Body fat loss and compensatory mechanisms in response to different doses of aerobic exercise - a randomized controlled trial in overweight sedentary males. Am J Physiol Regul Integr Comp Physiol. 2012 doi: 10.1152/ajpregu.00141.2012. [DOI] [PubMed] [Google Scholar]
- 58.Ross R, Janssen I. Physical activity, total and regional obesity: dose-response considerations. Medicine and science in sports and exercise. 2001;33(6 Suppl):S521–7. doi: 10.1097/00005768-200106001-00023. discussion S8-9. [DOI] [PubMed] [Google Scholar]
- 59.Ross R, Janssen I, Dawson J, Kungl AM, Kuk JL, Wong SL, et al. Exercise-induced reduction in obesity and insulin resistance in women: a randomized controlled trial. Obesity research. 2004;12(5):789–98. doi: 10.1038/oby.2004.95. [DOI] [PubMed] [Google Scholar]
- 60.Snyder KA, Donnelly JE, Jabobsen DJ, Hertner G, Jakicic JM. The effects of long-term, moderate intensity, intermittent exercise on aerobic capacity, body composition, blood lipids, insulin and glucose in overweight females. Int J Obes Relat Metab Disord. 1997;21(12):1180–9. doi: 10.1038/sj.ijo.0800533. [DOI] [PubMed] [Google Scholar]
- 61.Stubbs RJ, Hughes DA, Johnstone AM, Whybrow S, Horgan GW, King N, et al. Rate and extent of compensatory changes in energy intake and expenditure in response to altered exercise and diet composition in humans. Am J Physiol Regul Integr Comp Physiol. 2004;286(2):R350–8. doi: 10.1152/ajpregu.00196.2003. [DOI] [PubMed] [Google Scholar]
- 62.Stubbs RJ, Sepp A, Hughes DA, Johnstone AM, Horgan GW, King N, et al. The effect of graded levels of exercise on energy intake and balance in free-living men, consuming their normal diet. European journal of clinical nutrition. 2002;56(2):129–40. doi: 10.1038/sj.ejcn.1601295. [DOI] [PubMed] [Google Scholar]
- 63.Stubbs RJ, Sepp A, Hughes DA, Johnstone AM, King N, Horgan G, et al. The effect of graded levels of exercise on energy intake and balance in free-living women. Int J Obes Relat Metab Disord. 2002;26(6):866–9. doi: 10.1038/sj.ijo.0801874. [DOI] [PubMed] [Google Scholar]
- 64.Sullivan EL, Cameron JL. A rapidly occurring compensatory decrease in physical activity counteracts diet-induced weight loss in female monkeys. Am J Physiol Regul Integr Comp Physiol. 2010;298(4):R1068–74. doi: 10.1152/ajpregu.00617.2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Teske JA, Billington CJ, Kuskowski MA, Kotz CM. Spontaneous physical activity protects against fat mass gain. Int J Obes (Lond) 2012;36(4):603–13. doi: 10.1038/ijo.2011.108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Thomas DM, Bouchard C, Church T, Slentz C, Kraus WE, Redman LM, et al. Why do individuals not lose more weight from an exercise intervention at a defined dose? An energy balance analysis. Obesity reviews : an official journal of the International Association for the Study of Obesity. 2012;13(10):835–47. doi: 10.1111/j.1467-789X.2012.01012.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Tremblay A, Poehlman ET, Despres JP, Theriault G, Danforth E, Bouchard C. Endurance training with constant energy intake in identical twins: changes over time in energy expenditure and related hormones. Metabolism: clinical and experimental. 1997;46(5):499–503. doi: 10.1016/s0026-0495(97)90184-0. [DOI] [PubMed] [Google Scholar]
- 68.Visona C, George VA. Impact of dieting status and dietary restraint on postexercise energy intake in overweight women. Obesity research. 2002;10(12):1251–8. doi: 10.1038/oby.2002.170. [DOI] [PubMed] [Google Scholar]
- 69.Westerterp KR. Assessment of physical activity: a critical appraisal. European journal of applied physiology. 2009;105(6):823–8. doi: 10.1007/s00421-009-1000-2. [DOI] [PubMed] [Google Scholar]
- 70.Westerterp KR. Physical activity, food intake, and body weight regulation: insights from doubly labeled water studies. Nutrition reviews. 2010;68(3):148–54. doi: 10.1111/j.1753-4887.2010.00270.x. [DOI] [PubMed] [Google Scholar]
- 71.Westerterp KR, Meijer GA, Janssen EM, Saris WH, Ten Hoor F. Long-term effect of physical activity on energy balance and body composition. Br J Nutr. 1992;68(1):21–30. doi: 10.1079/bjn19920063. [DOI] [PubMed] [Google Scholar]
- 72.Westerterp KR, Plasqui G. Physical activity and human energy expenditure. Current opinion in clinical nutrition and metabolic care. 2004;7(6):607–13. doi: 10.1097/00075197-200411000-00004. [DOI] [PubMed] [Google Scholar]
- 73.Whybrow S, Hughes DA, Ritz P, Johnstone AM, Horgan GW, King N, et al. The effect of an incremental increase in exercise on appetite, eating behaviour and energy balance in lean men and women feeding ad libitum. Br J Nutr. 2008;100(5):1109–15. doi: 10.1017/S0007114508968240. [DOI] [PubMed] [Google Scholar]
- 74.Wishnofsky M. Caloric equivalents of gained or lost weight. The American journal of clinical nutrition. 1958;6(5):542–6. doi: 10.1093/ajcn/6.5.542. [DOI] [PubMed] [Google Scholar]
- 75.Zurlo F, Ferraro RT, Fontvielle AM, Rising R, Bogardus C, Ravussin E. Spontaneous physical activity and obesity: cross-sectional and longitudinal studies in Pima Indians. The American journal of physiology. 1992;263(2 Pt 1):E296–300. doi: 10.1152/ajpendo.1992.263.2.E296. [DOI] [PubMed] [Google Scholar]