

Abstract
Corticosteroid can induce osteonecrosis in children with leukemia. Few studies have been designed to assess the influence of a wide range of cumulative steroid dose on this side effect. Prevalence, risk factors of symptomatic osteonecrosis and its impact on adults’ Quality of Life were assessed in 943 patients enrolled in the French “Leucémies de l'Enfant et de l'Adolescent“ (LEA) cohort of childhood leukemia survivors. During each medical visit, data on previous osteonecrosis diagnosis were retrospectively collected. Patients without a history but with suggestive symptoms were investigated with magnetic resonance imaging. The total steroid dose in equivalent of prednisone was calculated for each patient and its effect on osteonecrosis occurrence was studied in multivariate models. Cumulative incidence was 1.4% after chemotherapy alone versus 6.8% after transplantation (P<0.001). A higher cumulative steroid dose, age over ten years at diagnosis, and treatment with transplantation significantly increased the risk of osteonecrosis. A higher post-transplant steroid dose and age over ten years at time of transplantation were significant factors in the transplanted group. With patients grouped according to steroid dose quartile, cumulative incidence of osteonecrosis reached 3.8% in the chemotherapy group for a dose beyond 5835 mg/m2 and 23.8% after transplantation for a post-transplant dose higher than 2055 mg/m2. Mean physical composite score of Quality of Life was 44.3 in patients with osteonecrosis versus 54.8% in patients without (P<0.001). We conclude that total and post-transplant cumulative steroid dose may predict the risk of osteonecrosis, a rare late effect with a strong negative impact on physical domains of Quality of Life.
Introduction
Approximately 80% of children with acute lymphoblastic leukemia (ALL) and 60% of those with acute myeloblastic leukemia (AML) can be cured of their disease.1 Along with the improved cure rate, awareness of treatment-related late effects has become increasingly important.2 Osteonecrosis (ON) has long been recognized as a complication of leukemia treatment.3–5 The Childhood Cancer Survivor Study has compared the rate of self-reported ON in cancer survivors with the rate observed in a sibling comparison group. The rate ratio was 6.5 in non-transplanted ALL, 11.2 in non-transplanted AML, and 59.2 for allogeneic hematopoietic stem cell transplantation (HSCT) recipients.6 ON can result in severe pain, loss of function, and joint collapse requiring surgical intervention.7,8 The initial imaging technique is often a plain radiograph but now magnetic resonance imaging (MRI) has been established as the most sensitive method in the early diagnosis of ON.9
Prevalence and risk factors for ON effect have varied widely in previously published papers. This might reflect differences in the definition and detection methods of ON but also disparities in the studied cohorts such as size and type of the cohort, inclusion criteria (notably the percentage of adolescents) and the treatments received (mainly the cumulative steroid dose). Corticosteroids are essential for the treatment of pediatric ALL10–12 and have been identified as the main cause of ON in this context. However, few studies were designed to understand the effect of the cumulative steroid dose as a quantitative variable on the risk of ON and, to our knowledge, none of them have tried to identify a steroid dose threshold. On the other hand, many published studies are based on a chemotherapeutic protocol and patients who received hematopoietic stem cell transplantation (HSCT) as part of their anti-leukemic treatment are often excluded. In the present study, data were extracted from a large cohort of childhood leukemia survivors, the French LEA cohort, which is not based on a specific therapeutic protocol but was designed to include all children treated for leukemia after 1980 in several participating centers. This allowed us to assess the influence of a wide range of cumulative steroid dose and to compare children treated with chemotherapy only to those treated by chemotherapy and HSCT. In addition, we also evaluate the impact of ON on Quality of Life of patients who reached adulthood.
Design and Methods
Patient selection
This study was designed to describe the prevalence of symptomatic ON, to identify risk factors, and to evaluate its impact on Quality of Life. We analyzed all patients included during the years 2004–2009 in the French LEA cohort, a multicenter program initiated in 2003 to evaluate prospectively long-term health status of childhood leukemia survivors who had been treated after 1980. Details of the whole program have been previously described.13 Briefly, data are collected during specific medical visits at pre-defined dates beginning one year after completion of chemotherapy or one year after HSCT, then repeatedly every two years until the patient reaches 20 years of age and has more than ten years follow-up duration from diagnosis, and every four years thereafter. The study was approved by the French National Program for Clinical Research, the French National Cancer Institute (InCA), and an ethics committee.
Study end point
ON was one of the late side effects that were systematically evaluated in the LEA program. During the medical visits, each patient with a previous diagnosis of symptomatic ON was identified. Date of diagnosis, joints involved and treatments were detailed. Patients were clinically evaluated during the medical visit and MRI of the symptomatic joints was proposed if ON was clinically suspected.
Steroid therapy
Cumulative steroid doses differed according to the protocol used for leukemia treatment. For each patient, we collected the cumulative dose of prednisone and dexamethasone received as part of conventional therapy and during the post-transplantation period. The total steroid dose in equivalent of prednisone received was calculated using the formula: total steroid dose in mg/m2 = dose of prednisone + (dose of dexamethasone x 6.67).14–16
Quality of Life
The Quality of Life (QoL) of adult patients was assessed using the SF-36 questionnaire,17 a reliable instrument to assess self-perceived health status in adult survivors of childhood cancer.18 The SF-36 is comprised of 36 items describing 8 dimensions and two summary composite scores: the physical composite score (PCS) and the mental composite score (MCS). The PCS and MCS scores are norm-based, using a linear T-score transformation with a mean of 50.
Statistical methods
Prevalence rates of ON were expressed as percentage of affected patients in a given population. Cumulative incidences of ON over time were estimated using the Kaplan-Meier method, displayed with their 95% confidence interval (CI) and compared with the log rank test. Multivariate logistical regression analyses were used to construct models of association between prevalence rates of ON and potential risk factors. Multiple linear regression models were constructed to explore the potential link between occurrence of ON and the patient’s long-term QoL scores. To help interpret the clinical significance of differences in means scores of QoL dimensions, effect sizes were calculated by dividing the difference between the mean score of patients with ON and the mean score of patients without ON by the standard deviation of the non-ON group. We considered an effect size of 0.2–0.49 as ‘small’, 0.5–0.79 as ‘medium’ and 0.8 or higher as ‘large’.19
Results
Characteristics of studied cohort
Among the 1115 childhood leukemia survivors fulfilling criteria for LEA inclusion in the five participant centers, 943 patients agreed to participate and were enrolled in the LEA program during the years 2004–2009 (response rate 84.6%). There was no significant difference in gender, type of leukemia, age at diagnosis, history of relapse, and treatment or not with HSCT between the responder group and the non-responder group.
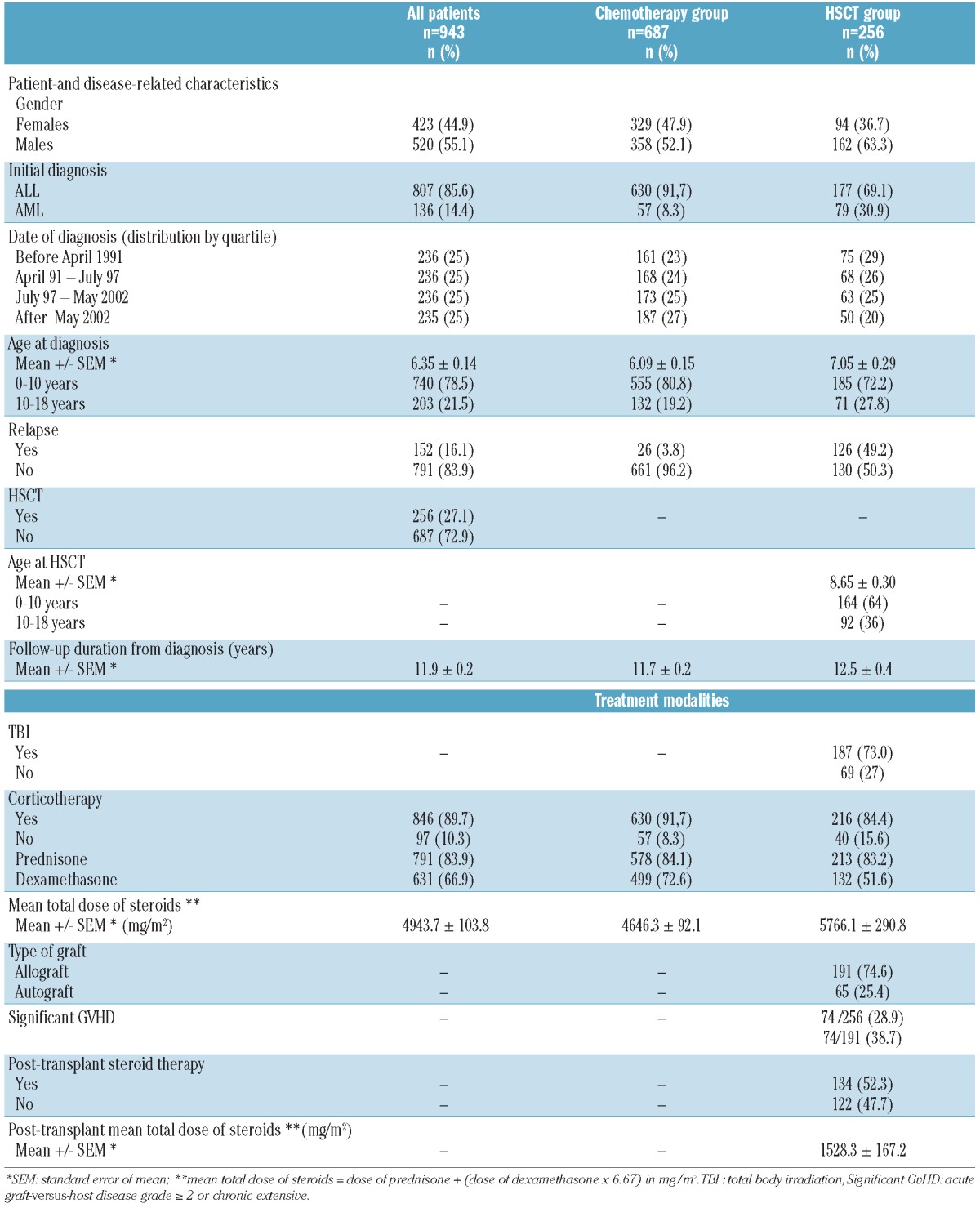
All these 943 patients had ON assessment during each of their specific LEA medical visits: data on previous osteonecrosis diagnosis were retrospectively collected whereas patients without such a history were clinically evaluated and proposed to have MRI examination of the symptomatic joints. Details of patient- and disease-related characteristics, as well as treatment modalities, are shown in Table 1. All patients had been treated after 1980 for acute lymphoblastic (ALL, n=807) or acute myeloid leukemia (AML, n=136), with the various treatment protocols that were used in France during this time period. Mean follow-up duration from diagnosis to last LEA evaluation was 11.9 years. Two hundred and three patients were over ten years of age at time of diagnosis. Six hundred and eighty-seven were treated by chemotherapy with or without CNS irradiation, whereas the 256 other patients also received HSCT (65 autografts and 191 allografts from sibling, unrelated donor or cord blood). All patients with ALL received corticosteroids. Among 136 AML patients, 97 never received steroids and 39 who were treated with allogeneic HSCT received post-transplant steroid therapy. Mean total steroid dose was 4943.7 mg/m2 for the whole cohort. In the HSCT group, total dose was 5766.1 mg/m2, including 1528.3 mg/m2 during the post-transplant period, whereas total dose was 4646.3 mg/m2 in the chemotherapy group.
Table 1.
Patients’ and treatment characterictics.
Features and risk factors of osteonecrosis
Among the 943 patients, 24 (2.5%) developed symptomatic ON within a median of 1.8 years (interquartile range, IQR, 1.2–3.5 years) after the diagnosis of acute leukemia. Median time was 2.4 years (IQR, 0.9–3.3) after diagnosis in the chemotherapy group and 0.9 years (IQR, 0.6–1.5) after the first transplant in the HSCT group. The cumulative incidence of ON over time was 2.8±0.6% for the whole cohort (Figure 1). This incidence was 6.8±1.8% in the HSCT group and 1.4±0.5% in the chemotherapy group (P<0.001). In the HSCT group, all symptomatic ON occurred after transplantation and none during the previous chemotherapeutic phase. The most frequent locations were knee (15 patients) and hip (11 patients). Multiple joints involvement was not rare (7 of 24 cases, 29.2%). Four patients required surgical joint replacement.
Figure 1.

Cumulative incidence of osteonecrosis (A) All patients (B) Chemotherapy group versus HSCT group (C). All patients grouped according to cumulative steroid dose quartiles. (D) Chemotherapy patients grouped according to cumulative steroid dose quartiles. (E) HSCT patients grouped according to the post-transplant cumulative steroid dose quartiles. Almost all patients in the quartile 1 and 2 did not receive any post-transplant steroid therapy. Consequently the first category includes all patients with a cumulative dose equal to 0.
Univariate analysis of risk factors was carried out in the whole cohort and then separately in the ‘chemotherapy’ and the ‘HSCT’ subgroups (Table 2). Age over ten years at time of diagnosis and a higher cumulative steroid dose increased the risk for ON in the whole cohort as well as in both subgroups. Date of diagnosis, distributed by quartile was also a significant risk factor, the highest risk being observed during the most recent time periods. This reflected changes in steroid cumulative steroid dose according to the treatment protocols over the time periods (Table 3). In the HSCT group, 4 additional significant factors were detected: age over ten years at time of transplant, the type of HSCT (the risk being higher after allogeneic than after autologous transplantation), the occurrence of graft-versus-host disease (GvHD) and a higher post-transplant steroid dose. Gender did not appear to interfere significantly with the development of ON. ALL patients treated with chemotherapy only had a 1.4% prevalence of symptomatic ON whereas all patients with AML and osteonecrosis were in the HSCT group. AML patients who received HSCT had a 5% prevalence (4 of 79) who reached 6.6% (4 of 61) when only allogeneic HSCT were considered. All significant risk factors in the univariate analysis were entered in the multivariate logistical regression models with the exception of type of graft and GvHD that were clearly in a cause and effect relationship with the post-transplant steroid dose. Results of the multivariate models are shown in Table 4. In the whole cohort, age at diagnosis, HSCT and higher total steroid dose were significant prognostic factors. Considering the 2 therapeutic subgroups, significant factors were age at diagnosis and steroid dose in the chemotherapy group, and age at transplantation and post-transplant steroid dose in the HSCT group.
Table 2.
Risk factors for osteonecrosis patients: univariate analysis.
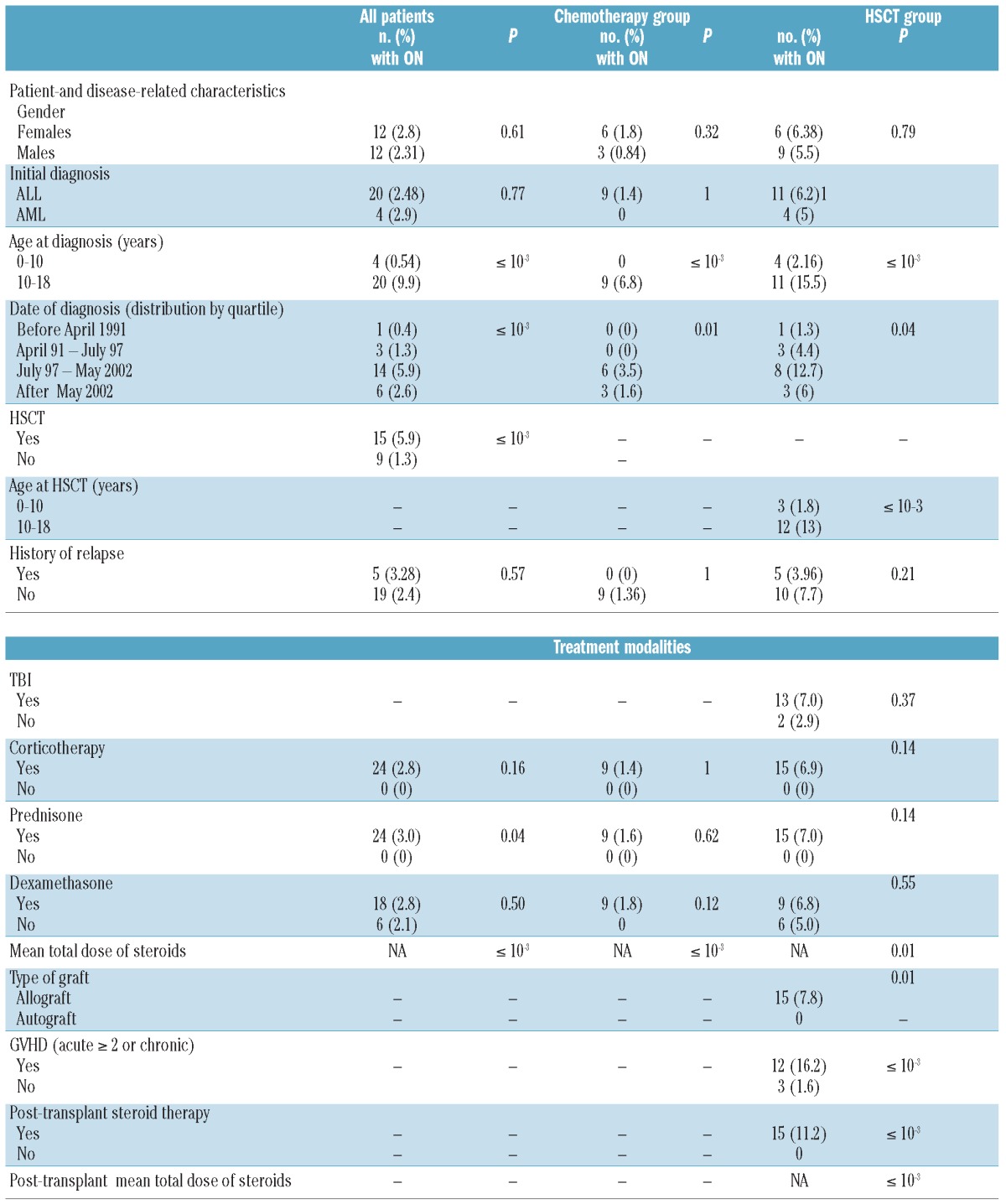
Table 3.
Cumulative dose of steroids according to date of diagnosis.
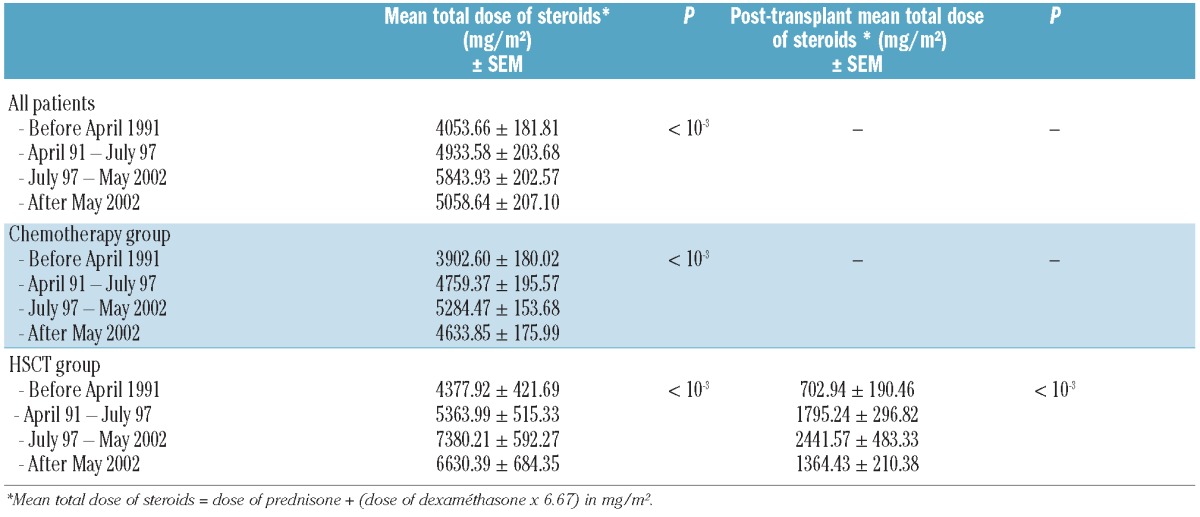
Table 4.
Risk factors for osteonecrosis: multivariate analysis.
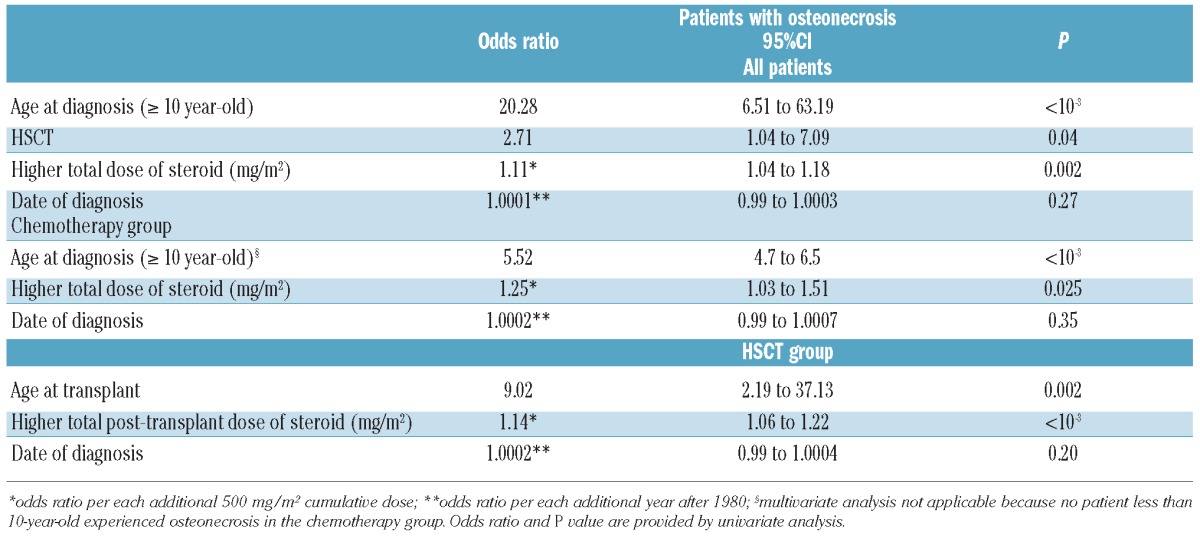
Figure 1 shows the cumulative incidence of ON depending on steroid dose with patients grouped according to dose quartiles. In the whole cohort, as well as in both therapeutic subgroups, the threshold was apparently at the higher dose category. More precisely, cumulative incidence of ON reached 8.6% (95%CI: 5.2–14.5) in the whole cohort for a steroid dose over 6150 mg/m2. This incidence was 3.8% (1.7–8.5) in the chemotherapy group over 5835 mg/m2 and 23.8% (12.8–44.4) for children who received HSCT and a post-transplant steroid dose exceeding 2055 mg/m2.
QoL in osteonecrosis patients
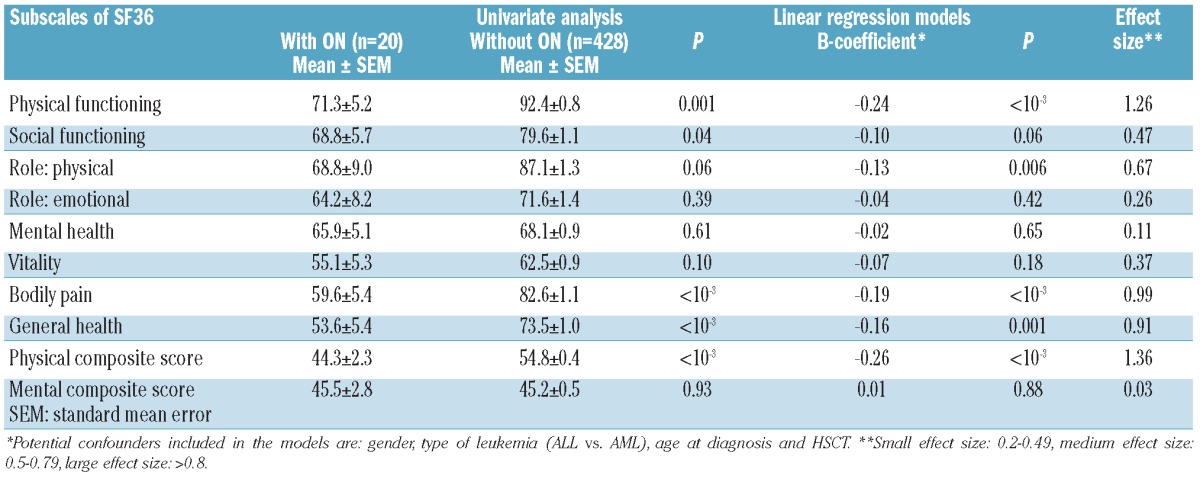
Among 493 patients who had reached adulthood at time of evaluation, 448 completed the SF36 questionnaire. Twenty of them had ON. As reported in table 5, ON had a strong negative impact on physical domains of quality of life. In the multivariate analysis (including gender, type of leukemia, age at diagnosis and HSCT as potential confounders), ON significantly deteriored the physical composite score (PSC) and the subscales “physical functioning”, “role limitations due to physical health problems”, “bodily pain” and “general health”. The effect sizes were larger than 0.80 (range, 0.91 to 1.36) in the PCS, “physical functioning”, “bodily pain” and “general health”. On the other hand, no significant difference was found in the mental composite score.
Table 5.
Effect of osteonecrosis (ON) on Quality of Life among adults survivors (SF36).
Discussion
This study was designed to evaluate symptomatic ON in a large cohort of long-term childhood leukemia survivors, with a separate analysis of patients treated by chemotherapy alone or by chemotherapy and HSCT. The cumulative incidence estimation was 2.8% for all patients, 6.8% after HSCT and 1.4% in the chemotherapy group.
In previous publications, the incidence estimation has been variable, probably reflecting differences in the definition (symptomatic or asymptomatic) and detection methods of ON, anti-leukemic treatments and cohort sizes.20 Our estimation is similar to those reported after several chemotherapeutic protocols such as the BFM 95 with 1.8% in 1951 patients,21 the UKALL XII with 4% in 1053 patients,22 and in a study from Greece that found a cumulative incidence of 2.5% in 276 patients.23 In some other cohorts, reported incidences have been higher, ranging from 7.1 to 14%.15,24–27 The time of occurrence we describe here is also comparable with many existing studies who reported a 14–27 month median time interval from leukemia diagnosis to ON occurrence.15,20–25 After allogeneic transplantation for childhood leukemia, Faraci et al. found a 3.9% prevalence of clinically and radiologically documented ON.28 Another study revealed a prevalence of ON in almost 30% of the children who had systematic serial MRI of hips and knees (even if they had no clinical symptom) during the three years after their allogeneic HSCT, but in several patients, osteonecrotic lesions resolved spontaneously.29 Patients with early, asymptomatic and regressive ON were not identified in the LEA late effect program because only symptomatic patients were investigated. This difference in study design may in part explain some discrepancy in prevalence rates. In addition, unlike reports from clinical trials, our analysis is based on a study of survivors and did not include non-survivors with ON.
Most previous studies have underlined that the main risk factor for ON after leukemia treatment is age over ten years at diagnosis or at time of HSCT. This unique susceptibility of adolescents is not easily explainable. Even if the physiopathology of ON remains largely unknown and probably multifactorial, a vascular role is clearly implicated.30,31 One hypothesis is that steroid therapy can induce proliferation of marrow lipocytes. In adolescents with epiphyseal closure, this marrow fat-cell hypertrophy results in elevated intraosseous pressure followed by reduced intramedullary blood flow, marrow ischemia and, ultimately, necrosis. In contrast, immature bone may buffer increased pressure at the epiphyseal plate.30 The fact that adolescents are prone to develop ON may also be explained by age-related differences in steroid-induced changes in the coagulation system during leukemia treatment.26 Finally, a PAI-1 gene polymorphism predicts ON in children aged ten years and over with ALL, suggesting that this inhibitor of fibrinolysis plays a role in the pathophysiology.32
For HSCT patients, GVHD is a risk factor for ON, probably due to intensive use of steroid and immunosuppression.5,28 Our study confirms this relationship and suggests that the risk may be extremely high when the post-transplantation steroid dose is over 2055 mg/m2. Total body irradiation has also been implicated,28 but this was not significant in our study.
Steroids, such as prednisone (PDN) and dexamethasone (DXM) are an essential component of acute lymphoblastic leukemia treatment but have a well-established role in ON occurrence. In our study, 97 patients out of 943 did not receive corticosteroids because they had AML, and none of them experienced symptomatic ON. Furthermore, we demonstrated a highly significant impact of the cumulative steroid dose on symptomatic ON occurrence in the whole cohort as well as in the two therapeutic subgroups. In the HSCT subgroup, we also found that the post-transplant steroid dose was a major risk factor. In addition, our analysis by quartile suggests a threshold cumulative steroid dose as well as a threshold post-transplant dose for the risk of symptomatic ON. The majority of patients with symptomatic ON had a total dose of steroids 6150 mg/m2 or over, or a total post transplant dose of corticosteroids 2055 mg/m2 or over. To our knowledge, this study is the first that suggests threshold doses. Interestingly, published data from different childhood ALL trials that reported both ON incidence and cumulative steroid doses also indicate that the higher the total dose of steroids, the higher the risk of ON is. In the CCG-1882 and the DFCI 87-01/91-01 trials, steroid dose in PDN equivalent was 7,782–11,150 and 7,600–21,530, respectively, the corresponding ON incidence being 9.3% and 6–9%.15,24 Conversely ON incidence was only 1.8% in the ALL-BFM95 trial with a steroid dose of 3,411–6,993.21
Dexamethasone may cause more adverse effects than PDN including infection, mood and behavior problems, myopathy and skeletal morbidity (defined as musculoskeletal pain, fracture or ON).33,34 However, DXM has not been incontrovertibly proven to cause more ON that PDN. Strauss et al.15 described an association between DXM and higher risk of fractures, but not higher risk of ON. In our study, no difference was observed between DXM and PDN, perhaps because the large proportion of children who had received both types of steroid precluded sufficient statistical power. Modalities of administration and duration of DXM therapy may also be implicated. In one study, the incidence of ON decreased significantly when the duration of DMX exposure during the intensification phase was shortened from 3–4 weeks to two weeks, independently of the cumulative total dose, suggesting that the duration of DMX treatment might be as equally important as the total dose.16 In the CCG-1961 trial, alternate-week DXM (given from Days 1–7 and Days 15–21) during 2 delayed intensifications reduced the risk of ON compared with continuous DXM during only one delayed intensification in rapid early responders.35,36
Several limitations of our current study must be considered. Although the studied cohort was large, the final number of symptomatic ON is quite small and only 9 among 24 affected patients were in the chemotherapy group. This clearly limits the study’s statistical power to detect risk factors. Moreover, even if the study included only childhood leukemia survivors, we acknowledge that some heterogeneity in types of leukemia and treatments received may be confounding factors. On the other hand, in this context, the highly significant impact of steroid cumulative dose and our findings regarding threshold doses can be stressed in both the chemotherapeutic and the HSCT groups. In our univariate analysis, symptomatic ON occurred more frequently during the most recent years than in the past. This was concomitant with a more intensive use of steroids in the most recent French ALL protocols.37–41 It might also reflect a larger use of unrelated donors and cord blood in the HSCT group, with its subsequent effect on the post-transplant steroid dose. Finally, we cannot exclude that diagnosis of symptomatic ON was less accurate in the early period. Interestingly, when the date of diagnosis and the steroid dose were entered together in the multivariate models, the steroid dose remained the statistically significant criteria whereas the effect of the date lost its significance.
Other drugs may influence the risk of ON. L-asparaginase was included in all chemotherapeutic ALL protocols used in France during the study period. L-asparaginase-induced coagulopathy might increase the risk of ON,42 but to our knowledge, this hypothesis has never been confirmed. Several authors have suggested that high-dose methotrexate is a risk factor for osteoporosis.43 However, in one study that compared cumulative methotrexate dose given in the Nordic ALL protocols,16 the higher cumulative dose of methotrexate was associated with a decreased risk for ON, probably because patients who received more methotrexate received lower steroid dose.
Several studies have recently been carried out to evaluate the QoL among survivors of childhood cancer.44–50 Although impairment in several domains of QoL have been described, its relationships with different long-lasting adverse effects such as ON remain largely unknown. Our study specifically assessed the impact of symptomatic osteonecrosis on QoL of adults surviving childhood leukemia. We detected major and statistically significant differences in the physical domains of QoL. The large effect sizes of these differences underline their potential clinical relevance and the need for careful evaluation of this side effect.
Acknowledgments
For their assistance with the LEA database, we sincerely thank D. Orbicini, F. Garnier, B. Play and A. Loundou, as well as the entire LEA program staff. We also thank all the survivors who agreed to participate in this study.
Footnotes
The online version of this paper has a Supplementary Appendix.
Funding
This study was financially supported by the French National Cancer Institute (InCA) and the Regional «PACA cancéropole ».
Authorship and Disclosures
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Pui CH, Carroll WL, Meshinchi D, Arceci RJ. Biology, risk stratification, and therapy of pediatric acute leukemias: an update. J Clin Oncol. 2011;29(5):551–65 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Oeffinger KC, Mertens AC, Sklar CA, Kawashima T, Hudson MM, Meadows AT, et al. Chronic health conditions in adult survivors of childhood cancer. N Engl J Med. 2006;355(15):1572–82 [DOI] [PubMed] [Google Scholar]
- 3.Murphy RG, Greenberg ML. Osteonecrosis in pediatric patients with acute lymphoblastic leukemia. Cancer. 1990;65(8):1717–21 [DOI] [PubMed] [Google Scholar]
- 4.Körholz D, Bruder M, Engelbrecht V, Rüther W, Göbel U. Aseptic osteonecrosis in children with acute lymphoblastic leukemia. Pediatr Hematol Oncol. 1998;15(4):307–15 [DOI] [PubMed] [Google Scholar]
- 5.Socié G, Sélimi F, Sedel L, Frija J, Devergie A, Esperou Bourdeau H, et al. Avascular necrosis of bone after allogeneic bone marrow transplantation: clinical findings, incidence and risk factors. Br J Haematol. 1994; 86(3):624–8 [DOI] [PubMed] [Google Scholar]
- 6.Kadan-Lottick NS, Dinu I, Wasilewski-Masker K, Kaste S, Meacham S, Mahajan A, et al. Osteonecrosis in Adult Survivors of Childhood Cancer: A Report From the Childhood Cancer Survivor Study. J Clin Oncol. 2008;26:3038–45 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kaste SC. Skeletal toxicities of treatment in children with cancer. Pediatr Blood Cancer. 2008;50(2 Suppl):469–73 [DOI] [PubMed] [Google Scholar]
- 8.Karimova EJ, Rai SN, Howard SC, Neel M, Britton L, Pui CH, et al. Femoral head osteonecrosis in pediatric and young adult patients with leukemia or lymphoma. J Clin Oncol. 2007;25(12):1525–31 [DOI] [PubMed] [Google Scholar]
- 9.Mitchell DG, Rao VM, Dalinka MK, Spritzer CE, Alavi A, Streinberg ME, et al. Femoral head avascular necrosis: correlation of MR imaging, radiographic staging, radionuclide imaging, and clinical findings. Radiology. 1987;162(3):709–15 [DOI] [PubMed] [Google Scholar]
- 10.Inaba H, Pui CH. Glucocorticoid use in acute lymphoblastic leukaemia. Lancet Oncol. 2010;11(11):1096–106 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.McNeer JL, Nachman JB. The optimal use of steroids in paediatric acute lymphoblastic leukaemia: no easy answers. Br J Haematol. 2010;149(5):638–52 [DOI] [PubMed] [Google Scholar]
- 12.Labar B, Suciu S, Willemze R, Muus P, Marie JP, Fillet G, et al. Dexamethasone compared to prednisolone for adults with acute lymphoblastic leukemia or lymphoblastic lymphoma: final results of the ALL-4 randomized, phase III trial of the EORTC Leukemia Group. Haematologica. 2010;95(9):1489–95 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Michel G, Bordigoni P, Simeoni MC, Curtillet C, Hoxha S, Robitail S, et al. Health status and quality of life in long-term survivors of childhood leukaemia: the impact of haematopoietic stem cell transplantation. Bone Marrow Transplant. 2007;40(9):897–904 [DOI] [PubMed] [Google Scholar]
- 14.Haynes RC, Jr, Murad F. Adrenocorticotropic hormone; adrenocortical steroids and their analogs; inhibitors of adrenocortical steroid biosynthesis. In: Gilman AG, Goodman LS, Rall TW, et al. (eds): The Pharmacological Basis of Therapeutics (ed 7). New York, NY: Macmillan Publishing Company, 1985, pp. 1459–89 [Google Scholar]
- 15.Strauss AJ, Su JT, Dalton VM, Gelber RD, Sallan SE, Silverman LB. Bony morbidity in children treated for acute lymphoblastic leukemia. J Clin Oncol. 2001;19(12):3066–72 [DOI] [PubMed] [Google Scholar]
- 16.Niinimaki RA, Harila-Saari AH, Jartti AE, Seuri RM, Riikonen PV, Pääkkö EL, et al. Body Mass Index increases the risk of osteonecrosis in childrem with acute lymphoblastic leukemia. J Clin Oncol. 2007; 25(12):1498–504 [DOI] [PubMed] [Google Scholar]
- 17.Leplege A, Ecosse E, Verdier A, Perneger TV. The French SF-36 Health Survey: translation, cultural adaptation and preliminary psychometric evaluation. J Clin Epidemiol. 1998;51(11):1013–23 [DOI] [PubMed] [Google Scholar]
- 18.Reulen RC, Zeegers MP, Jenkinson C, Lancashire ER, Winter DL, Jenney ME, et al. The use of the SF-36 questionnaire in adult survivors of childhood cancer: evaluation of data quality, score reliability and scaling assumptions. Health Qual Life Outcomes. 2006;4:77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Cohen J. Statistical power analysis for the behavioural sciences, 2nd ed Lawrence Eribaum Associates Publishers, Hillsdale, NJ, USA: 1998 [Google Scholar]
- 20.Te Winkel ML, Pieters R, Hop WC, De Groot-Kruseman HA, Lequin MH, Van der Sluis IM, et al. Prospective study on incidence, risk factors and long-term outcome of osteonecrosis in pediatric acute lymphoblastic leukemia. J Clin Oncol. 2011; 29(31):4143–50 [DOI] [PubMed] [Google Scholar]
- 21.Burger B, Beier R, Zimmermann M, Beck JD, Reiter A, Schrappe M. Osteonecrosis:a treatment related toxicity in chilhood acute lymphoblastic leukemia (ALL), experiences from trail ALL-BFM 95. Pediatr Blood Cancer. 2005;44(3):220–5 [DOI] [PubMed] [Google Scholar]
- 22.Patel B, Richards SM, Rowe JM, Goldstone AH, Fielding AK. High incidence of avascular necrosis in adolescents with acute lymphoblastic leukemia: a UKALL XII analysis. Leukemia. 2008;22(2):308–12 [DOI] [PubMed] [Google Scholar]
- 23.Tragiannidis A, Athanassiadou F, Papageorgiou T, Petsatodis G, Sidi V, Kolouskas D. Osteonecrosis in children with acute lymphoblastic leukemia: a 10 year study from Northern Greece. Pediatr Blood Cancer. 2007;49(5):764. [DOI] [PubMed] [Google Scholar]
- 24.Mattano LA, Jr, Sather HN, Trigg ME, Nachman JB. Osteonecrosis as a complication of treating acute lymphoblastic leukemia in children: a report from the children’s cancer group. J Clin Oncol. 2000; 18(18):3262–72 [DOI] [PubMed] [Google Scholar]
- 25.Högler W, Wehl G, Van Staa T, Meister B, Klein-Franke A, Kropshofer G. Incidence of skeletal complications during treatment of childhood acute lymphoblastic leukemia: comparison of fracture risk with the general practice research database. Pediatr Blood Cancer. 2007;48(1):21–7 [DOI] [PubMed] [Google Scholar]
- 26.Te Winkel ML, Appel IM, Pieters R, Van den Heuvel-Eibrink MM. Impaired dexamethasone-related increase of anticoagulants is associated with the development of osteonecrosis in childhood acute lymphoblastic leukemia. Haematologica. 2008; 93(10):1570–4 [DOI] [PubMed] [Google Scholar]
- 27.Pui CH, Campana D, Pei D, Bowman WP, Sandlund JT, Kaste SC, et al. Treating childhood acute lymphoblastic leukemia without cranial irradiation. N Engl J Med. 2009;360(26):2730–41 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Faraci M, Calevo MG, Lanino E, Caruso S, Messina C, Favr C, et al. Osteonecrosis after allogenic stem cell transplantation in childhood: a case control study in Italy. Haematologica. 2006;91(8):1096–9 [PubMed] [Google Scholar]
- 29.Sharma S, Leung WH, Deqing P, Yang J, Rochester R, Britton L, et al. Osteonecrosis in children after allogeneic hematopoietic cell transplantation: study of prevalence, risk factors and longitudinal changes using MR imaging. Bone Marrow Transplant. 2012;47 (8):1067–74 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Barr RD, Sala A. Osteonecrosis in children and adolescents with cancer. Pediatr Blood Cancer. 2008;50(2 Suppl):483–5 [DOI] [PubMed] [Google Scholar]
- 31.Kawedia JD, Kaste SC, Pei D, Panetta JC, Cai X, Cheng C, et al. Pharmacokinetic, pharmacodynamic and pharmacogenetic determinants of osteonecrosis in children with acute lymphoblastic leukemia. Blood. 2011;117(8):2340–7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.French D, Hamilton LH, Mattano LA, Sather HN, Devidas M, Nachman JB, et al. A PAI-1 (SERPINE1) polymorphism predicts osteonecrosis in children with acute lymphoblastic leukemia: a report from the Children’s Oncology Group. Blood. 2008; 111(9):4496–9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Teuffel O, Kuster SP, Hunger SP, Conter V, Hitzier J, Ethier MC, et al. Dexamethasone versus Prednisone for induction therapy in childhood acute lymphoblastic leukemia: a systematic review and meta-analysis. Leukemia. 2011;25(8):1232–8 [DOI] [PubMed] [Google Scholar]
- 34.Elmantaser M, Stewart G, Young D, Duncan R, Gibson B, Ahmed SF. Skeletal morbidity in children receiving chemotherapy for acute lymphoblastic leukemia. Arch Dis Child. 2010;95(10):805–9 [DOI] [PubMed] [Google Scholar]
- 35.Mattano LA, Jr, Devidas M, Nachman JB, Sather HN, Hunger SP, Steinherz PG, et al. Effect of alternate-week versus continuous dexamethasone scheduling on the risk of osteonecrosis in paediatric patients with acute lymphoblastic leukaemia: results from the CCG-1961 randomised cohort trial. Lancet Oncol. 2012;13(9):906–15 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Van den Heuvel-Eibrink MM, Pieters R. Steroids and risk of osteonecrosis in ALL: take a break. Lancet Oncol. 2012; 13(9):855–7 [DOI] [PubMed] [Google Scholar]
- 37.Schaison G, Sommelet D, Bancillon A, Perel Y, Leblanc T, Bergeron C, et al. Treatment of acute lymphoblastic leukemia French protocol Fralle 83–87. Leukemia. 1992;6(Suppl 2):148–52 [PubMed] [Google Scholar]
- 38.Oudot C, Auclerc MF, Levy V, Porcher R, Piguet C, Perel Y, et al. Prognostic factor for leukemic induction failure in children with acute lymphoblastic leukemia and outcome after salvage therapy: the Fralle 93 study. J Clin Oncol. 2008; 26(9):1496–503 [DOI] [PubMed] [Google Scholar]
- 39.Vilmer E, Suciu S, Ferster A, Bertrand Y, Cavé H, Thyss A, et al. Long-term results of three randomized trials (58831, 58832, 58881) in childhood acute lymphoblastic leukemia: a CLCG EORTC report. Leukemia. 2000;14(12):2257–66 [DOI] [PubMed] [Google Scholar]
- 40.Uyttebroeck A, Suciu S, Laureys G, Robert A, Pacquement H, Ferster A, et al. Treatment of childhood T-cell lymphoblastic lymphoma according to the strategy for acute lymphoblastic leukemia, without radiotherapy: long term results of the EORTC CLG 58881 trial. Eur J Cancer. 2008;44(6):840–6 [DOI] [PubMed] [Google Scholar]
- 41.De Moerloose B, Suciu S, Bertrand Y, Mazingue F, Robert A, Uyttebroeck A, et al. Improved outcome with pulses of vincristine and corticosteroids in continuation therapy of children with average risk acute lymphoblastic leukemia (ALL) and lymphoblastic non-Hodgkin lymphoma (NHL): report of the EORTC randomized phase III trial 58951. Blood. 2010;116(1):36–44 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Hanada T, Horigome Y, Inudoh M, Takita H. Osteonecrosis of vertebrae in a child with acute lymphocytic leukaemia during L-asparaginase therapy. Eur J Pediatr. 1989; 149(3):162–3 [DOI] [PubMed] [Google Scholar]
- 43.Pfeilschifter J, Diel JJ. Osteoporosis Due to Cancer Treatment: Pathogenesis and Management. J Clin Oncol. 2000;18(7): 1570–93 [DOI] [PubMed] [Google Scholar]
- 44.Chiou SS, Jang RC, Liao YM, Yang P. Health-related quality of life and cognitive outcomes among child and adolescent survivors of leukemia. Support Care Cancer. 2010;18(12):1581–7 [DOI] [PubMed] [Google Scholar]
- 45.Armenian SH, Sun CL, Kawashima T, Arora M, Leisenring W, Sklar CA, et al. Long-term health-related outcomes in survivors of childhood cancer treated with hematopoietic cell transplantation (HCT) versus conventional therapy: a report from the Bone Marrow Transplant Survivor Study and Childhood Cancer Survivor Study. Blood. 2011;118(5):1413–20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Hudson MM, Mertens AC, Yasui Y, Hobbie W, Chen W, Gurney JG, et al. Health status of adult long-term survivors of childhood cancer: a report from the childhood cancer survivor study. JAMA. 2003;290(12):1583–92 [DOI] [PubMed] [Google Scholar]
- 47.Hamidah A, Wing CY, Tamil AM, Zarina LA, Zulkifli ZS, Jamal R. Health-related quality of life (HRQOL) among pediatric leukemia patients in Malaysia. Pediatr Blood Cancer. 2011;57(1):105–9 [DOI] [PubMed] [Google Scholar]
- 48.De Vries MA, van Litsenburg RR, Huisman J, Grootenhuis MA, Versluys AB, Kaspers GJ, et al. Effect of dexamethasone on quality of life in children with acute lymphoblastic leukemia: a prospective observational study. Health Qual Life Outcomes. 2008; 26;6:103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Clarke SA, Skinner R, Guest J, Darbyshire P, Cooper J, Vora A, et al. Clinical outcomes and health-related quality of life (HRQOL) following haematopoietic stem cell transplantation (HSCT) for paediatric leukemia. Child Care Health. 2010;37(4):571–80 [DOI] [PubMed] [Google Scholar]
- 50.Pallua S, Giesinger J, Oberguggenberger A, Kemmler G, Nachbaur D, Clausen J, et al. Impact of GVHD on quality of life in long-term survivors of haematopoietic transplantation. Bone Marrow Transplant. 2010; 45(10):1534–9 [DOI] [PubMed] [Google Scholar]