

Abstract
Associations between water sources, socio-demographic characteristics and household drinking water quality are described in a representative sample of six coastal districts of Ghana’s Central Region. Thirty-six enumeration areas (EAs) were randomly chosen from a representative survey of 90 EAs in rural, semi-urban and urban residence strata. In each EA, 24 households were randomly chosen for water quality sampling and socio-demographic interview. Escherichia coli per 100 ml H2O was quantified using the IDEXX Colilert® system and multi-stage regression models estimated cross-sectional associations between water sources, sanitation and socio-demographic factors. Almost three quarters, 74%, of the households have > 2 E. coli /100 ml H2O. Tap water has significantly lower E. coli levels compared with surface or rainwater and well water had the highest levels. Households with a water closet toilet have significantly lower E. coli compared with those using pit latrines or no toilets. Household size is positively associated, and a possessions index is negatively associated, with E. coli. Variations in community and household socio-demographic and behavioural factors are key determinants of drinking water quality. These factors should be included in planning health education associated with investments in water systems.
Keywords: E. coli, Ghana, household water source, rural urban effects, sanitation, water quality
INTRODUCTION
Unsafe water, sanitation and hygiene are responsible for almost 4% of the global total in disability adjusted life years (DALYs), and among high mortality countries almost 6% of the total attributable DALYs (WHO 2002). This is due to the strong and consistent association in developing nations between unsafe water and hygiene, and infant and child mortality arising from diarrhoeal diseases (Shier et al. 1996; Huttly et al. 1997; Boadi & Kuitunen 2005a). Recent studies of the mortality transitions in the US in the late 19th and early 20th centuries attribute three-quarters of the infant mortality decline and two-thirds of the child mortality decline to the development and spread of clean water technologies (Cutler & Miller 2005).
The decade 2005–2015 was declared the International Water Decade by the United Nations. The UN alerted policy makers about a ‘global water crisis’, noting in the 2006 Human Development Report that 2 million children die annually from diseases related to water-borne illnesses, and millions more women and children spend hours just collecting water, restricting their opportunities to do other things (UN 2006). Additionally, water-borne infectious diseases create more poverty and slow economic growth. The International Water Decade’s goal, to be achieved by 2015, is to reduce by half the proportion of people who regularly obtain their drinking water from unhealthy sources or from far away places. The goal also calls for better access to basic sanitation.
Despite the consensus on the critical need for clean water to improve child and population health, simple provision of clean water through municipal or private piped systems has not yielded the expected immediate health improvements in most developing world communities (Clasen & Cairncross 2004). Recent systematic reviews and meta-analyses of interventions to improve water quality suggest that, although such interventions are generally effective in preventing diarrhoea, the substantial variation across water improvement trials points to still unknown factors that influence water quality and diarrhoea (Clasen et al. 2006, 2007). This suggests to us that detailed research is needed on how household socio-demographic and sanitation factors influence water quality by structuring access to, and use of, different types of water source.
These structuring factors include spatial factors such as origin of, as well as distance to, water sources, especially in rural areas (Jagals et al. 1999), and the location of households along the rural to urban continuum (Wright et al. 2004). Urban places with high population densities may not have access to safe drinking water, and water transported long distances may be of dubious quality and safety (Wright et al. 2004). Household socio-economic status measures such as education and occupation may be associated with exposure to, and perceived salience of, health education about water quality and sanitary habits. For example, detailed evidence from behavioural studies of water use and quality indicates the roles played by variations in household storage of water and sanitary habits, such as hand washing, on microbiological contamination of household water supply (Clasen & Bastable 2003; Brick et al. 2004; Trevett et al. 2005). Household social and economic variables are also associated with types of toilet facility and waste disposal pattern, which directly affect water quality (Wright et al. 2004; Cronin et al. 2006). Despite the demonstrated importance of more proximate individual behavioural factors on water quality, socio-demographic studies of household water quality may help answer questions about variations at community and household level in water acquisition, use and quality. As investments are made to establish modern water systems, such research can lead to more efficient design and targeting of household and community training about water sources, safe use and storage as well as waste disposal.
The purpose of this paper is to examine associations between social and demographic characteristics, water sources, sanitation factors and household drinking water quality in a representative sample of residents of the six coastal districts of Ghana’s Central Region, one of the ten administrative regions in Ghana. Although key proximate determinants of water quality such as hand-washing and water storage have been established, this report focuses on more ultimate socio-economic variations between communities and households that contribute to household water quality levels and which may produce health inequalities, such as differences in diarrhoea risk. As infrastructure improvements proceed as part of economic development, increasing attention must be paid to the link between socioeconomic and health inequalities for aetiologic understanding and applied interventions (Braveman & Tarimo 2002; Marmot 2005).
METHODS
Study setting and population
Our study population resides in six coastal districts of the Central Region, Ghana, namely Komenda-Edina-Eguafo-Abirem (KEEA), Cape Coast, Abura-Asebu-Kwamankese, Mfantsiman, Gomoa and Awutu-Efutu-Senya1. The coastal belt of the Central Region through Accra to Togo experiences rainfall totals which are atypically drier than most tropical coastal regions. The coast from Cape Coast to Accra has rainfall of around 760 MM (Dickson & Benneh 1994), compared with Axim, on the southwest coast of Ghana, which receives about 2,160 MM of rainfall. Worldwide coastal areas within the tropical zone experience rainfall totals of not less than 2,030 MM per annum. This unusual dry condition along the coast of the Central Region has given rise to acute water shortages for most parts of the year. To offset the water shortages, boreholes and wells have been sunk in some of the rural communities.
The two major cities within the Central Region are Cape Coast, the regional capital, and Winneba, a city about halfway between Cape Coast and Accra. The water system for Cape Coast was built in 1927–28 to serve the population of the town which at that time was less than 20,000. The water system has not seen any major expansion since it was built in spite of the increase in population and the expansion of the system to nearby settlements. As a result, the pipe-borne water supply in the area is inadequate to meet the demands of the increasing population. The Awutu-Efutu-Senya district (where Winneba is located) and the Gomoa district are among the driest along the coastal zone. As with all the major towns along the coast in Central Region, Winneba experiences water shortages for most of the year.
This area of Ghana is primarily inhabited by the Fante ethnic group (an Akan sub-group linguistically related to the Asante), as well as other smaller groups (e.g. Ewe, Ga-Dangme, etc.). Nationally, the Fante compose about 10% (about 1.7 million people) of Ghana’s total population. While Ghana’s major sources of foreign exchange are gold, timber and cocoa, economic activities in the study area include fishing, small-scale farming, salt production and some tourism activities (concentrated around the former slave trading castles dotting the Central Region coastline which now operate as museums).
Sample selection
The household water quality study took place with a sample chosen to be representative of the six coastal districts of the Central Region. The representative survey is based on a two-stage stratified sampling design. The Ghana Statistical Service provided a list of enumeration areas (EA) and their population information. We selected equal numbers of EAs in each of our three residence strata (rural, semi-urban and urban) and we compensate for this in our analyses through the use of weights. We chose this design in order to evenly spread the sample across the strata, ensuring that there is sufficient sample size in each strata type. The stratification was done for the six districts, which, when multiplied by the three stratum types, resulted in a total of 18 strata. Within each of the 18 strata, we selected five EAs using probability proportional to size of the EA. Thus, we initially drew a representative sample of 90 EAs, 54 of which were used in earlier survey work in 2002, and the remainder used for this study conducted in 2004.
After we generated our first-stage sample of EAs, survey teams listed all the households in our 36 selected EAs for the 2004 fieldwork. We then randomly selected 24 households from each EA. Survey interviewing teams then conducted the socio-demographic interview with household heads and collected a drinking water sample from each selected household. The target sample was 864 households, of which 749 households were interviewed. Some households refused to give us a sample of their drinking water, resulting in a final sample size of 703 households with both a water sample and a socio-demographic interview. We found no significant differences in the key variables later used in our incremental logistic regression model between those households providing a water sample and those that did not.
Measures
Quality of drinking water
Drinking water samples were collected from the main water vessel in each household. Because many households have multiple water storage vessels (e.g. large vessel outside the structure and smaller serving vessels inside), care was taken to ensure that the water sample came directly from the vessel used to dispense water for immediate consumption. Drinking water (100 ml) was poured into sterile (γ-irradiated) plastic containers and stored on ice. The samples were transported from the field to the laboratory in ≤6 hours. Total coliforms and Escherichia coli were quantified using enzyme-based defined substrate technology (IDEXX Colilert©). A modified most probable number (IDEXX Quanti-Tray/2000©) assay was used to estimate the abundance of the two indicators. The Quanti-Tray/200 has a working range of <1 to 2,049 indicator organisms in 100 ml. E. coli were enumerated as number of colonies per 100 ml of water. This method has been compared with more traditional assays and yields similar results (Hamilton et al. 2005).
The distribution of E. coli/100 ml H2O is adjusted by a natural logarithm because of its right skew. E. coli counts were classified into two categories, 0–1 and 2 to >1,000 E. coli/100 ml in order to contrast those with relatively safe water and those with contaminated water (Moe et al. 1991).
Household information
Interviews were conducted by trained local assistants with the head of household about the sources of the drinking water, walking time to usual water source, toilet facilities, refuse disposal, physical characteristics and possessions of the household, and household social and demographic characteristics. Water sources included pipes or taps, boreholes, wells, surface water, bottled water, water in sachets, tankers or rainwater. Boreholes are 10 to 20 feet deep, covered at ground level, and fitted with hand pumps. Wells are stone or clay round pits that are wide in diameter at the surface and not covered. Typically a carrying vessel is dipped into the well to retrieve water. Surface water could be from a pond, lake, rainwater or river water. Tankers are trucks with large water tanks which dispense water. Rainwater is collected from house roofs in barrels. Bottled water or water in plastic sachets are generally purchased from shops or street sellers. An index of material possessions was created based on whether the household owned the following items: working radio or cassette player, television, video recorder, telephone or mobile phone, stove, refrigerator or freezer, clock, sofa or chair with cushions, bed with mattress, bicycle, motorcycle or motorbike, car or other motor vehicle, working boat or canoe, and fishing nets. This index serves as our indicator of household wealth.
Villages were selected in urban, semi-urban and rural strata but after initial statistical models with the trichotomous residence location variable we combined the semi-urban and rural groups and contrasted that with the urban group.
Statistical analysis
Two types of regression model were performed. Ordinary least squares models were used to determine factors associated with the natural logarithm of E. coli water quality measures. Second, logistic regression was used to estimate the odds of unsafe household water quality, i.e. > 2 E. coli /100 ml. For both types of regression analysis we estimated four models in stages to allow for inferences about the potential confounding of some of the relationships: the first model included water source and the walking time to the water source; the second model included toilet type; the third added place for waste disposal; and the fourth model included presence of electricity in the home, and urban or rural and semi-urban residence, household size, the socio-economic status (SES) index and ownership of farmland. We also conducted analyses in the sub-sample of households, N = 275, who did not receive their water from a tap to explore the interrelationships of water source and sanitary habits with socio-economic factors.
RESULTS
Based on the original sampling design, one-third of the households in the study sample is urban (population over 5,000), one-third is semi-urban (population between 2,500 and 5,000) and one-third is rural. Over 50% have electricity, and almost half own farmland (Table 1).
Table 1.
Description of household water sources, sanitation and socio-demographic characteristics
| Characteristics | Percentage or mean and standard deviation |
|---|---|
| Water source | |
| Tap | 61.5 |
| Borehole | 14.1 |
| Surface water | 9.20 |
| Well | 8.20 |
| Bottled or sachet water | 4.3 |
| Tanker | 2.01 |
| Rainwater | 0.9 |
| Toilet type | |
| Pit | 62.1 |
| No facility | 28.5 |
| Water closet | 9.4 |
| Residence | |
| Urban | 33.6 |
| Semi-grban | 34.1 |
| Rural | 32.2 |
| Electricity | |
| Yes | 52.9 |
| No | 47.1 |
| Owns farmland | |
| Yes | 46.1 |
| No | 53.2 |
| Location of waste disposal | |
| Public bin or dump | 56.4 |
| Bush | 23.4 |
| Beach or lagoon | 16.4 |
| Pit in compound | 2.7 |
| Other disposal area | 1.1 |
| Household size | Mean = 3.99, std dev. = 2.37 |
| Minutes to water source | Mean = 13.30, std dev. = 15.45 |
| Number of possessions owned (out of 14) |
Mean = 3.07, std dev. = 2.42 |
More than 60% of households get their household water from a tap, almost 10% obtain water from surface water sources and 1% directly from rainwater. About 4% of households obtain water from bottled water or sachets, i.e. small plastic bags sold in shops and on the street (Dodoo et al. 2006). Almost 30% of households do not regularly use a toilet facility. A low level of household possessions characterizes the sample; the mean number of possessions is 3 out of 14 possible possessions. The average walking time to a water source is around 13 minutes; approximately 21% needed 30 minutes or more to get to a water source.
Household water quality was characterized by relatively high levels of E. coli/100 ml. The mean was 320.3 (s.d. = 662.3) with a median of 228.1 and a range from 0 to > 2,425 E. coli/100 ml H2O (Figure 1). Almost three quarters of the households, 74%, had water with > 2 E. coli /100 ml H2O.
Figure 1.
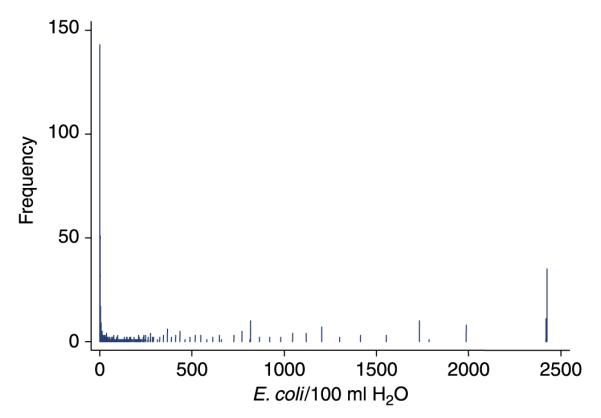
Frequency distribution of E. coli/100 ml H2O.
Household water from the tap had lower E. coli/100 ml H2O compared with all sources except from bottled water and sachets (Table 2). Water from wells has significantly more E. coli than surface or rainwater. Although few households use rainwater, it has lower E. coli levels than surface water after adjustment for all socio-demographic and sanitation factors. The pattern of associations between E. coli levels and water source remains after adjustment for other sanitation factors, rural/urban residence and household SES factors.
Table 2.
Estimates from OLS regression predicting the natural log of E. coli
| Independent variables | Model I | Model II | Model III | Model IV |
|---|---|---|---|---|
| Minutes to water source | Beta/(95% CI) 0.017*** (0.005, 0.029) |
Beta/(95% CI) 0.010* (−0.001, 0.022) |
Beta/(95% CI) 0.011* (−0.001, 0.022) |
Beta/(95% CI) 0.008 (−0.004, 0.020) |
| Water source | ||||
| Tap (ref.) | ||||
| Surface water | 2.861*** (2.227, 3.495) | 2.471*** (1.821, 3.121) | 2.508*** (1.854, 3.161) | 2.448*** (1.797, 3.101) |
| Rainwater | 2.635*** (0.599, 4.670) | 1.635 (−0.389, 3.659) | 1.467 (−0.572, 3.507) | 1.101 (−0.933, 3.135) |
| Well | 2.829*** (2.201, 3.456) | 2.609*** (1.989, 3.229) | 2.620*** (1.999, 3.242) | 2.504*** (1.885, 3.124) |
| Borehole | 0.933*** (0.434, 1.432) | 0.817*** (0.327, 1.308) | 0.800*** (0.308, 1.292) | 0.672*** (0.180, 1.163) |
| Tanker | 1.134* (−0.076, 2.344) | 0.668 (−0.550, 1.886) | 0.566 (−0.657, 1.789) | 0.682 (−0.537, 1.902) |
| Bottle or sachet | −1.453 *** (−2.409, −0.497) | −0.964** (−1.927, −0.002) | −0.928* (−1.890, 0.034) | −0.507 (−1.481, 0.467) |
| Toilet type | ||||
| Water closet (ref.) | ||||
| No toilet | 1.894*** (1.231, 2.558) | 1.655*** (0.948, 2.362) | 1.357*** (0.614, 2.101) | |
| Pit | 1.265*** (0.681, 1.849) | 1.106*** (0.514, 1.698) | 0.807** (0.186, 1.428) | |
| Where waste is disposed | ||||
| Public pit (ref.) | ||||
| Public bin | 1.555*** (0.516, 2.594) | 1.565*** (0.528, 2.603) | ||
| Bush | 1.434*** (0.355, 2.511) | 1.410** (0.329, 2.491) | ||
| Beach or lagoon | 1.713*** (0.573, 2.852) | 1.904*** (0.758, 3.050) | ||
| Other disposal mechanism | 1.388 (−0.813, 3.590) | 1.411 (−0.768, 3.590) | ||
| Electricity (none ref.) | −0.191 (−0.554, 0.172) | |||
| Residence (urban ref.) | 0.432** (0.036, 0.829) | |||
| Household size | 0.112*** (0.040, 0.183) | |||
| Possessions | −0.074* (−0.157, 0.090) | |||
| Owns farmland (does not own ref.) |
0.038 (−0.323, 0.400) | |||
| Constant | 2.461 | 1.294 | −0.048 | −0.180 |
| N | 703 | 703 | 703 | 703 |
| Adjusted R 2 | 0.231 | 0.255 | 0.261 | 0.277 |
P < 0.10
P < 0.05
P < 0.01.
Although the time to walk to a water source is positively associated with E. coli levels, this relationship is attenuated and becomes non-significant after adjustment for sanitary factors and socio-demographic characteristics.
Drinking water from households that use a water closet type of toilet has significantly lower E. coli compared with those who do not use any facility. Households using a pit latrine type toilet also have significantly lower E. coli in drinking water. These associations remain significant after further adjustment for sanitary and socio-demographic factors.
Urban households have lower E. coli levels than rural and semi-urban households. Household size is positively associated, and the household possessions index is marginally negatively associated, with E. coli levels.
The logistic regression models estimated that water from wells is 20–25 times more likely to be contaminated, i.e. > 2 E. coli/100 ml H2O, compared with tap water (Table 3). Household water collected from surface water sources is also associated with a 4–5 times elevated odds of contamination. Water from boreholes appears to be more contaminated but this effect disappears with further adjustment for sanitary and socio-demographic factors.
Table 3.
Estimates from Logit Regression Predicting E. Coli count (0 = Less than 2, 1 = 2 or more)
| Independent variables | Model I | Model II | Model III | Model IV |
|---|---|---|---|---|
| Minutes to water source | OR/(95% CI) 1.022** (1.005, 1.040) |
OR/(95% CI) 1.015* (0.998, 1.033) |
OR/(95%CI) 1.015* (.997, 1.033) |
OR/(95% CI) 1.012 (0.994, 1.030) |
| Water source | ||||
| Tap (ref.) | ||||
| Surface water | 5.152*** (1.786, 14.858) | 3.943** (1.335, 11.652) | 4.046** (1.355, 12.081) | 4.070** (1.359, 12.194) |
| Rainwater | 9.458* (0.937, 95.492) | 4.604 (0.439, 48.338) | 3.904 (0.359, 42.423) | 3.224 (0.290, 35.807) |
| Well | 24.914*** (3.409, 182.069) | 21.529*** (2.935, 157.928) | 25.123*** (3.270, 192.999) | 24.411*** (3.142, 189.641) |
| Borehole | 1.948*** (1.117, 3.392) | 1.795** (1.024, 3.148) | 1.742* (0.989, 3.086) | 1.612 (906, 2.867) |
| Tanker | 2.380 (0.519, 10.897) | 1.874 (0.379, 9.257) | 1.696 (0.341, 8.428) | 2.023 (0.400, 10.230) |
| Bottle or sachet | 0.309* (0.127, 0.755) | 0.429* (0.167, 1.101) | 0.451 (0.137, 1.172) | 0.609 (0.227, 1.631) |
| Toilet type | ||||
| Water closet (ref.) | ||||
| No toilet | 4.451*** (2.258, 8.773) | 3.780*** (1.808, 7.902) | 3.169*** (1.436, 6.994) | |
| Pit | 2.976*** (1.714, 5.166) | 2.298*** (1.536, 4.739) | 2.238*** (1.222, 4.101) | |
| Where waste is disposed | ||||
| Public pit (ref.) | ||||
| Public bin | 4.252** (1.363, 13.267) | 4.282** (1.373, 13.356) | ||
| Bush | 3.786** (1.163, 12.325) | 3.692** (1.124, 12.118) | ||
| Beach or lagoon | 4.77** (1.330, 17.109) | 5.125** (1.429, 18.388) | ||
| Other disposal mechanism | 1.387 (0.118, 16.241) | 1.294 (0.112, 15.001) | ||
| Electricity (none ref.) | 1.046 (0.686, 1.593) | |||
| Residence (urban ref.) | 1.387 (0.910, 2.115) | |||
| Household size | 1.092** (1.006, 1.186) | |||
| Possessions | 0.936 (0.855, 1.026) | |||
| Owns farmland (does not own ref.) |
1.047 (697, 1.573) | |||
| N | 703 | 703 | 703 | 703 |
| Pseudo R 2 | 0.10 | 0.12 | 0.13 | 0.15 |
P < 0.10
P < 0.05
P < 0.01
Households with a pit toilet or no toilet facilities have 2–3 times higher odds of contaminated water relative to those with a water seal toilet, even after adjustment for other sanitary and socio-demographic characteristics. Lastly, size of the household is associated with a significant increase in the odds of contaminated water.
In the subsample of 275 households who do not acquire water from taps, E. coli levels are significantly (P < 0.001) lower in water from boreholes, tankers and other sources compared with water from surface sources, but marginally (P < 0.06) higher in well water. Also in that subsample, there was a positive significant (P < 0.05) association between walking time to the water source and E. coli level. Households with no toilet or who use a pit latrine have significantly (P < 0.001) higher E. coli levels relative to those who use a water closet toilet. There were no associations between socio-economic or demographic factors and E. coli levels in the subsample after prior adjustment for water source and toilet type. In this subsample there were significant bivariate associations between socio-economic factors and both water source and toilet type. Households with a lower possessions index were more likely (P < 0.0001) to have no toilet facility and to use well and surface water sources.
DISCUSSION
Our results indicate a general problem of poor household water quality in the Central Region with almost three-quarters of the households having > 2 E. coli /100 ml H2O and almost one-quarter having > 250 E. coli/100 ml H2O. Access to safe water and sanitary infrastructure was moderate to low in our study in the Central Region of Ghana. This is similar to many other areas in developing nations and to other regions in Ghana (Ghana Statistical Service 2002; Keraita et al. 2003; Boadi & Kuitunen 2005a, b, c). Use of tap water for water consumption characterized 61% of the households, higher than the 40% reported in a study in the Accra metropolitan area (Boadi & Kuitunen 2005a), or the 32% estimated from a child health study of Accra households (Boadi & Kuitunen 2005b). We found that <10% of households had a flush toilet and that 29% had no toilet facility. This compares with 33% of households with a flush toilet and 2% with no toilet in Accra (Boadi & Kuitunen 2005b). Over 95% of our sample disposed of waste in public dumps or open spaces compared with about 86% in a study of urban Accra (Boadi & Kuitunen 2005c).
The combination of poor water quality and low level of infrastructure for safe water and sanitation suggest substantial risk from water-borne infectious diseases in this region. Given that 23% of childhood communicable diseases can be attributed to unsafe water and sanitation (WHO 2002), urgent attention is needed to extend safe water systems, provide direct investments for sanitary facilities and conduct household level health education campaigns about water and sanitation (Soares et al. 2002).
Despite the general patterns of poor water safety and sanitation, household water quality in the Central Region of Ghana is independently associated with water sources, human and other waste disposal patterns and socio-demographic factors. The most consistent finding in both the ordinary least squares (OLS) and logistic regression models is the strong independent association between lower water quality and water from wells and surface sources. In addition, in both models, lower water quality is associated with households using a pit toilet or without a toilet altogether, and households which dispose of waste in public bins, the bush or water bodies.
Water sources exert powerful direct influences on water safety and quality in the absence of household interventions to improve water quality (Shier et al. 1996; Steyn et al. 2004; Clasen et al. 2005, 2006, 2007; Cronin et al. 2006). Piped water from private or public systems generally has fewer pathogens than surface or well water, which are affected by drainage of human, animal and other wastes, particularly when sanitary waste disposal systems are lacking or poorly maintained. In the OLS model, water from boreholes had significantly higher E.coli levels, but, in contrast, boreholes were not strongly associated with unsafe water in the logistic regression using our criterion of > 2 E. coli/100 ml H2O. Previous studies suggest that boreholes often are a better quality source of drinking water relative to wells and surface water (Moe et al. 1991), and provide safer water during the dry season in Ghana (Shier et al. 1996).
Rainwater used for household consumption was not significantly different in E. coli levels from tap water, suggesting the potential utility of rainwater collection in areas without water infrastructure improvements. However, we note the very low proportion and number of households, n = 6, who report collecting rain for household water consumption. Because of the cost and waiting time for installation of piped water to households throughout the Central Region of Ghana, and especially in more remote and sparsely settled communities, rainwater collection may represent an alternative or supplementary mechanism for gathering drinking water. Further study is required on how rainwater is collected and stored by households since there is potential contamination of high quality rainwater by dirty house roofs as well as post-collection sanitary habits.
Our findings on the associations of toilet type and waste disposal habits with water quality replicate well-established results from many other studies about sanitary habits and local environmental hygiene infrastructure (Duse et al. 2003; Howard et al. 2003; Cronin et al. 2006). In our study in Ghana such factors raise the odds of poor water quality, > 2 E. coli/100 ml H2O, by 2–5 times after adjustment for water source and socio-economic factors. This suggests the critical importance of reducing these pathways to contamination of household water through a variety of investments from health education to investment in sustainable waste water and disposal systems (Clasen et al. 2007).
Increased walking time to water source was associated with lower water quality but this effect was attenuated to non-significance with the addition of water source, sanitary and socio-economic effects. Nonetheless in the subsample that obtain water from sources other than the tap, walking time is significantly (P < 0.05) associated with higher E. coli levels. This suggests that distance from the water source to the household may increase water contamination regardless of source – perhaps through contamination during transport, or in association with some household sanitary behaviours linked in currently unknown ways to the distance from the source (Jagals et al. 1999).
Several household socio-demographic factors are independently associated with water quality, in addition to the clear influence of water source and sanitation factors. Urban residence is associated with lower E. coli levels, and wealthier households have marginally lower E. coli levels, even after adjusting for urban vs. rural residence. In addition, smaller households are consistently associated with higher household water quality in both types of regression model. These associations between indicators of higher socio-economic status and better water quality replicate other studies of water quality and health which use various measures of social position in developing world populations (Manun’ebo et al. 1994; Shier et al. 1996; Nyati 2004).
We note that associations between SES and water quality and health are not found in all studies, including among recent refugees residing in Sierra Leone (Clasen & Bastable 2003) and a Russian city with deteriorating infrastructure (Egorov et al. 2002). These exceptions highlight the key role of the overall political and socio-economic context in partially determining the water quality available to households. In some political and economic situations, socio-demographic variation in household wealth, size and urban or rural residence may have little influence on water quality because of larger community or regional factors.
The finding that wealthier and smaller households regardless of rural or urban residence have better water quality is also not surprising, and probably reflects a variety of possible influences. For example, wealthier households without piped water may have a favoured location within easy walking distance of public facilities, including a public tap or public borehole (Jagals et al. 1999). Second, households with more wealth are likely to have accumulated resources that would make the household more sanitary in general through ownership or access to a flush instead of a pit toilet. Likewise, covered metallic or ceramic containers, or special storage vessels could be used to store household water, which may reduce contamination (Mazengia et al. 2002; Quick et al. 2002; Clasen & Bastable 2003; Brick et al. 2004). Lastly, higher parental education and occupation may be associated with greater understanding of water quality, sanitary behaviours and even purchasing safer water for consumption.
The results in the subsample of households without piped water generally support the findings in the whole sample about the importance of water source and toilet type. Although there are simple bivariate associations between the possessions index and water source and toilet type in this subsample, no independent effects of socioeconomic or demographic factors on water quality were detected in the OLS model. This suggests that social and economic factors exert their influence indirectly on water quality, operating through the expected associations of SES and water source and sanitation variables. Future research should focus on understanding the more complex indirect and direct associations of water quality and socio-demographic factors.
The expansion of water systems, especially in metropolitan regions, is a goal of many developing countries. If economic and political investments allow this expansion we predict that semi-urban households in Ghana’s Central Region may begin to have access to better water quality, while rural areas may still suffer lower quality water sources. It will be important to conduct longitudinal studies of water quality as metropolitan regions develop and identify key promoters and impediments to expansion of public and private water systems (Budds & McGranahan 2003).
This study has several strengths, most importantly the careful sampling of the six coastal districts of the Central Region of Ghana, one of ten national administrative regions. This yielded a large representative survey sample which allows us to describe with confidence patterns of water quality and its association with water sources, sanitation and household socio-demographic factors. The water collection techniques and bioassay provided a reliable and valid standard way to assess E. coli levels in household water. We also used multi-stage OLS and logistic regression modelling to systematically determine the independent influence of various factors on E. coli levels and on water safety using a consensus criterion (Moe et al. 1991). The specification of water sources also allowed us to detect a putative beneficial habit of collecting rainwater for consumption. Despite these advantages the cross-sectional design and the collinearity among some of the water source, sanitation and socio-demographic factors constrained our ability to make clear causal inferences. Our decision to exclude factors such as hand washing and types of water storage limits our ability to fully understand all sources of variation in household water quality. We did so to focus on the ultimate or structural influences at the community and household level. Because of the relatively low rainfall in this region, future work should also assess seasonal changes in water sources and reliance on multiple water sources. Our unpublished qualitative data from individual interviews and focus groups indicate such seasonal variations.
Despite the few independent associations of water quality with socio-demographic variables in our results, we believe that socio-economic factors are likely to play an ultimate causal role in the pathways that increase or decrease exposure to poor water quality. Further analysis using multi-level modelling may show how neighbourhoods and households structure the influences of water source, toilet type and waste disposal. This seems intuitive given the overwhelming role of poverty in developing country populations in determining access to basic infrastructure and services. But the challenge remains for ecosocial researchers on water quality to provide inferences about specific water access, use, storage and consumption behaviours at the household, neighbourhood and village levels which are likely to be structured by social and economic variations. Future research is needed in our study area about individual level behaviours related to drinking water collection, water storage and sanitary habits such as hand washing and use of soap (Trevett et al. 2005).
CONCLUSIONS
We conclude that poor water quality is widespread in this area of Ghana and speculate that there may be a substantial elevated risk for childhood diarrhoea and other water-borne infectious diseases. Because of the demonstrated associations of household water quality with unsafe water sources and waste disposal patterns the expansion of piped water systems should be linked to household and neighbourhood health education and training programmes about safety of water sources and waste disposal. Although we do not assess individual level influences on water quality in this report, our focus on more ultimate socio-economic factors provide important findings about structural influences at the community and household level.
ACKNOWLEDGEMENTS
This research was funded by NIH Fogarty HEED grant R21-TW006508, the MacArthur Foundation and the Mellon Foundation. We are grateful to the Department of Geography, University of Cape Coast research staff, as well as the Department of Oceanography, University of Rhode Island, for testing the collected water samples.
Contributor Information
Stephen T. McGarvey, International Health Institute, Brown University, Box G-S121, 121 South Main Street, Room 220, Providence, RI 02912, USA
Justin Buszin, Population Studies & Training Center, Brown University, Box 1836, Providence, RI 02912, USA.
Holly Reed, Population Studies & Training Center, Brown University, Box 1836, Providence, RI 02912, USA.
David C. Smith, Graduate School of Oceanography, University of Rhode Island, Narragansett, RI 02882, USA
Zarah Rahman, Population Studies & Training Center, Brown University, Box 1836, Providence, RI 02912, USA.
Catherine Andrzejewski, Population Studies & Training Center, Brown University, Box 1836, Providence, RI 02912, USA.
Kofi Awusabo-Asare, Department of Geography, University of Cape Coast, Cape Coast, Ghana.
Michael J. White, Population Studies & Training Center, Brown University, Box 1836, Providence, RI 02912, USA
REFERENCES
- Boadi KO, Kuitunen M. Childhood diarrhoeal morbidity in the Accra Metropolitan Area, Ghana: Socio-economic, environmental and behavioral risk determinants. J. Health Popul. Dev. Countries. 2005a;7(1):1–13. [Google Scholar]
- Boadi KO, Kuitunen M. Environment, wealth inequality and the burden of disease in the Accra metropolitan area, Ghana. Int. J. Environ. Health Res. 2005b;15(3):193–206. doi: 10.1080/09603120500105935. [DOI] [PubMed] [Google Scholar]
- Boadi KO, Kuitunen M. Environmental and health impacts of household solid waste handling and disposal practices in third world cities: The case of the Accra Metropolitan Area, Ghana. J. Environ. Health. 2005c;68(4):32–36. [PubMed] [Google Scholar]
- Braveman P, Tarimo E. Social inequalities in health within countries: Not only an issue for affluent nations. Soc. Sci. Med. 2002;54:1621–1635. doi: 10.1016/s0277-9536(01)00331-8. [DOI] [PubMed] [Google Scholar]
- Brick T, Primrose B, Chandrasekhar R, Roy S, Muliyil J, Kang G. Water contamination in urban south India: Household storage practices and their implications for water safety and enteric infections. Int. J. Hyg. Environ. Health. 2004;207:473–480. doi: 10.1078/1438-4639-00318. [DOI] [PubMed] [Google Scholar]
- Budds J, McGranahan G. Are the debates on water privatization besides the point? Experiences from Africa, Asia and Latin America. Environ. Urban. 2003;15(2):87–114. [Google Scholar]
- Clasen T, Bastable A. Faecal contamination of drinking water during collection and household storage: The need to extend protection to the point of use. J. Water Health. 2003;1(3):109–115. [PubMed] [Google Scholar]
- Clasen TF, Cairncross S. Editorial: Household water management: refining the dominant paradigm. Trop. Med. Int. Health. 2004;9(2):187–191. doi: 10.1046/j.1365-3156.2003.01191.x. [DOI] [PubMed] [Google Scholar]
- Clasen TF, Roberts I, Rabie T, Cairncross S. Interventions to Improve Water Quality for Preventing Diarrhoea (Protocol) John Wiley & Sons; New York: 2005. [DOI] [PubMed] [Google Scholar]
- Clasen T, Roberts I, Rabie T, Schmidt WP, Cairncross S. Interventions to improve water quality for preventing diarrhoea. Cochrane Database Syst. Rev. 2006;19(3):CD004794. doi: 10.1002/14651858.CD004794.pub2. [DOI] [PubMed] [Google Scholar]
- Clasen T, Schmidt WP, Rabie T, Roberts I, Cairncross S. Interventions to improve water quality for preventing diarrhoea: Systematic review and meta-analysis. BMJ. 2007 Mar 12; doi: 10.1136/bmj.39118.489931.BE. www.bmj.com/cgi/content/short/bmj.39118.489931.BEv1. [DOI] [PMC free article] [PubMed]
- Cronin AA, Breslin N, Gibson J, Pedley S. Monitoring source and domestic water quality in parallel with sanitary risk identification in northern Mozambique to prioritise protection interventions. J. Water Health. 2006;4(3):333–345. doi: 10.2166/wh.2006.029. [DOI] [PubMed] [Google Scholar]
- Cutler D, Miller G. The role of public health improvements in health advances: The twentieth-century United States. Demography. 2005;42(1):1–22. doi: 10.1353/dem.2005.0002. [DOI] [PubMed] [Google Scholar]
- Dickson KB, Benneh G. A New Geography of Ghana. Longman; London: 1994. [Google Scholar]
- Dodoo DK, Quagraine EK, Okai-Sam F, Kambo DJ, Headley JV. Quality of ‘sachet’ waters in the Cape Coast municipality of Ghana. J. Environ. Sci. Health A. 2006;41(3):329–342. doi: 10.1080/10934520500423238. [DOI] [PubMed] [Google Scholar]
- Duse AG, da Silva MP, Zietsman I. Coping with hygiene in South Africa, a water scarce country. Int. J. Environ. Health Res. 2003;13(Suppl 1):S95–105. doi: 10.1080/0960312031000102859. [DOI] [PubMed] [Google Scholar]
- Egorov A, Ford T, Tereschenko A, Drizhd N, Segedevich I, Fourman V. Deterioration of drinking water in the distribution system and gastrointestinal morbidity in a Russian city. Int. J. Environ. Health Res. 2002;12:221–233. doi: 10.1080/09603/202/000000989. [DOI] [PubMed] [Google Scholar]
- Ghana Statistical Service . 2000 Population and Housing Census: Summary Report of Final Results. Accra; Ghana: 2002. [Google Scholar]
- Hamilton WP, Kim M, Thackston EL. Comparison of commercially available Escherichia coli enumeration tests: Implications for attaining water quality standards. Water Res. 2005;39:4869–4878. doi: 10.1016/j.watres.2005.02.006. [DOI] [PubMed] [Google Scholar]
- Howard G, Pedley S, Barrett M, Nalubega M, Johal K. Risk factors contributing to microbiological contamination of shallow groundwater in Kampala, Uganda. Water Res. 2003;37(14):3421–3429. doi: 10.1016/S0043-1354(03)00235-5. [DOI] [PubMed] [Google Scholar]
- Huttly SR, Morris SS, Pisani V. Prevention of diarrhoea in young children in developing countries. B. World Health Organ. 1997;75(2):163–174. [PMC free article] [PubMed] [Google Scholar]
- Jagals P, Bokako TC, Grabow W. Changing consumer water-patterns and their effect on microbiological water quality as a result of an engineering intervention. Water SA. 1999;25(3):297–300. [Google Scholar]
- Keraita B, Drechsel P, Amoah P. Influence of urban wastewater on stream water quality and agriculture in and around Kumasi, Ghana. Environ. Urban. 2003;15(2):171–178. [Google Scholar]
- Manun’ebo MN, Haggerty PA, Kalengaie M, Ashworth A, Kirkwood BR. Influence of demographic, socioeconomic and environmental variables on childhood diarrhea in a rural area of Zaire. J. Trop. Med. 1994;97:31–38. [PubMed] [Google Scholar]
- Marmot M. Social determinants of health inequalities. The Lancet. 2005;365(9464):1099–1104. doi: 10.1016/S0140-6736(05)71146-6. [DOI] [PubMed] [Google Scholar]
- Mazengia MS, Chidavaenzi M, Bradley M, Jere M, Nhandara C, Chigunduru D, Murahwa EC. Effective and culturally acceptable water storage in Zimbabwe: Maintaining the quality of water abstracted from upgraded family wells. J. Environ. Health. 2002;64:15–18. [PubMed] [Google Scholar]
- Moe CL, Sobsey MD, Samsa GP, Mesolo V. Bacterial indicators of risk of diarrhoeal disease from drinking-water in the Philippines. B. World Health Organ. 1991;69(3):305–317. [PMC free article] [PubMed] [Google Scholar]
- Nyati H. Evaluation of the microbial quality of water supplies to municipal, mining and squatter communities in the Bindura urban area of Zimbabwe. Water Sci. Technol. 2004;50(1):99–103. [PubMed] [Google Scholar]
- Quick RE, Kimura A, Thevos A, Tembo M, Shamputa I, Hutwagner L, Mintz E. Diarrhoea prevention through household-level water disinfection and safe storage in Zambia. Am. J. Trop. Med. Hyg. 2002;66(5):584–589. doi: 10.4269/ajtmh.2002.66.584. [DOI] [PubMed] [Google Scholar]
- Shier RP, Dollimore N, Ross DA, Binka FN, Quigley M, Smith PG. Drinking water source, mortality and diarrhoea morbidity among young children in northern Ghana. Trop. Med. Int. Health. 1996;1(3):334–341. doi: 10.1046/j.1365-3156.1996.d01-55.x. [DOI] [PubMed] [Google Scholar]
- Soares LC, Griesinger MO, Dachs JN, Bittner MA, Tavares S. Inequities in access to and use of drinking water services in Latin America and the Caribbean. Rev. Panam. Salud Publica. 2002;11(506):386–396. doi: 10.1590/s1020-49892002000500013. [DOI] [PubMed] [Google Scholar]
- Steyn M, Jagals P, Genthe B. Assessment of microbial infection risks posed by ingestion of water during domestic water use and full-contact recreation in a mid southern African region. Water Sci. Technol. 2004;50(1):301–308. [PubMed] [Google Scholar]
- Trevett AF, Carter RC, Tyrell SF. Mechanisms leading to post-supply water quality deterioration in rural Honduran communities. Int. J. Hyg. Environ. Health. 2005;208(3):153–161. doi: 10.1016/j.ijheh.2005.01.024. [DOI] [PubMed] [Google Scholar]
- UN (United Nations) Human Development Report 2006. United Nations Development Programme; New York: 2006. [Google Scholar]
- WHO (World Health Organization) World Health Report 2002: Reducing Risks, Promoting Healthy Life. World Health Organization; Geneva: 2002. [Google Scholar]
- Wright J, Gundry S, Conroy R. Household drinking water in developing countries: A systematic review of microbiological contamination between source and point-of use. Trop. Med. Int. Health. 2004;9(1):106–117. doi: 10.1046/j.1365-3156.2003.01160.x. [DOI] [PubMed] [Google Scholar]