

Abstract
Background:
The most common complication of hospitalization in intensive care units (ICUs) is infections caused by health care. Although sepsis results in a small percentage of infections, it has a high mortality rate. Intensive care nurses play a critical role in the prevention, early detection, and beginning of therapeutic interventions in patients with sepsis. This study aimed to review the effects of an educational program on knowledge, attitude, and practice of ICU nurses in Shariati Hospital, Isfahan, Iran.
Materials and Methods:
This was a quasi-experimental study on 64 nurses with at least one year of experience in ICU. The subjects were randomly selected and divided into test and control groups. Scores of knowledge, attitude, and practice of the participants were reviewed through a researcher-made questionnaire before and immediately and three weeks after a one-day workshop.
Findings:
Compared to baseline, there were significant increases in mean scores of knowledge, attitude, and practice in the test group immediately and three weeks after the education. Mean scores of knowledge in the test group before and immediately and 3 weeks after the intervention were 64.5, 84.9 and 85.2, respectively. The corresponding values for attitude were 73, 79.7, and 83.3. Mean scores of practice were 81.8, 90.5, and 91.3 before and immediately and 3 weeks after the intervention, respectively. In the control group, mean scores of knowledge before and immediately and 3 weeks after the educational course (which they did not attend) was 63.7, 63.9, and 63.5, respectively. Mean scores of attitude were respectively 72.8, 73.3, and 73.2 at the mentioned intervals. The corresponding values for practice were 82.1, 82.9, and 82.7.
Conclusions:
Training significantly improved levels of knowledge, attitude, and practice of ICU nurses in sepsis care. Therefore, compiling and organizing seminars and continuous basic educational workshops for sepsis care are recommended for health caregivers.
Keywords: Continuing education, sepsis, knowledge, attitude, practice
INTRODUCTION
Sepsis and its related signs are among the most common causes of mortality worldwide.[1] Although a small percentage of infections (approximately 5%), is allocated to sepsis, it has a high mortality rate which is more than 50% in some microorganisms causing infection.[2,3] Furthermore, it is the most important subject of health care since it has a high incidence, pathogenicity, and mortality and consumes a great deal of care resources.[4] The World Health Organization reported 60% of mortalities in developing countries to be caused by infectious diseases. On the other hand, severe sepsis is responsible for 50% of these deaths in the first 24-hour after infection.[5]
Each year, almost 751,000 cases of sepsis are reported in the U.S. among whom 215,000 lead to death. About 30-50% of these cases are associated with mortality.[6] Moreover, in a European comprehensive study, more than one-third of adult patients in intensive care units (ICUs) had sepsis among whom 25% had acquired the disease in other wards.[7]
Despite advances in medical knowledge during the past three decades, only a small reduction has occurred in mortality caused by sepsis. Therefore, sepsis is still considered among the important research areas.[8] The importance of sepsis is because it primarily requires early diagnosis and treatment in health centers.[9] The role of critical care nurses in detecting sepsis is important, because astute observation and assessment of patients can result in early and prompt diagnosis and treatment, with a subsequent decrease in sepsis-related mortality.[10] Furthermore, lack of a specific diagnostic test for early detection of sepsis, along with the rapid progress and high mortality rate of this disease would make the role of nurses more significant in prevention, diagnosis of early signs, and care.[11,12] Accordingly, due to the importance of nursing cares in ICUs, nurses working in such wards should be able to use all their knowledge, awareness, and experiences as quick as possible to save patients’ lives. They are also required to permanently seek to increase their knowledge and awareness.[13] Therefore, increasing knowledge and attitude and improving the practice of nurses are effective methods to control sepsis.[14,15]
As many studies have shown,[16,17] continuous educational programs are necessary for empowerment of nurses to maintain their current skills and theoretical knowledge.[16–19] Training nurses in all working areas and domains and in various wards is something inevitable and important. However, training the staff of ICUs seems more vital and important due to the extraordinary sensitivity of such units.[20] In order to enable nurses to provide the best care for patients at risk of developing sepsis, their education about sepsis should include items such as identifying different stages of sepsis, prevention, monitoring physiological parameters, and caring.[21]
Despite few studies on sepsis in Iran, there are no accurate statistics about the incidence of this disease.[22,23] On the other hand, global statistics have shown low rates of knowledge, attitude, and practice of treatment groups in this regard.[24–26] Therefore, this study aimed to review the effects of an educational program about sepsis care on knowledge, attitude, and practice of ICU nurses. The main objective of the researchers was to evaluate mean scores of knowledge, attitude, and practice of ICU nurses about sepsis before and immediately and three weeks after the educational program in test and control groups.
MATERIALS AND METHODS
This was a quasi-experimental interventional study with two groups and three stages during which the effects of the dependent variable (educational program on sepsis care) on independent variables (knowledge, attitude, and practice) were assessed. The study population included nurses of intensive care units [ICUs, critical care unit (CCU), and hemodialysis and emergency units] in Shariati Hospital of Isfahan.
Using convenient sampling followed by table of random numbers, 32 nurses were enrolled in each of the test and control groups. The inclusion criteria were having a bachelor’s degree or higher and 1 year of experience in ICU. Subjects were not included if they had participated in a similar study and was a member of the Infection Control Committee.
Data collection tool was a 4-part researcher-made questionnaire. The first part determined demographic characteristics such as age, sex, education, experience in intensive units, and employment status. The second part consisted of 18 questions to review the knowledge of nurses about sepsis care using a 3-point Likert scale (Yes/No/No Idea). Thus, correct and incorrect answers were scored as 2 and 1, respectively. If the participant did not know the answer, the score was 0. The third and fourth parts (with 12 and 16 questions) used 1 5-point Likert scale to respectively evaluate the attitude and practice of nurses. Correct choices were scored as 5 and incorrect choices as 1 (for negative items, scoring was reversed). Mean scores of knowledge, attitude, and practice were then compared between groups.
The validity of the questionnaire was assessed by content validity. More precisely, a questionnaire was first developed by searching the available printed and online literature. It was then revised, evaluated, and corrected by 11 faculty members and relevant experts.
The reliability of the tool was obtained by calculating Cronbach’s alpha coefficient. To do so, during a session, the questionnaires were distributed among 10 randomly selected nurses with similar inclusion criteria. Cronbach’s alpha was obtained as 80.9%, 77.0%, and 90.7% for knowledge, attitude, and practice, respectively.
The intervention was a one-day workshop (8 hours) of educational program on sepsis care. The test group attended the workshop in the clinical skills workshop of Shariati Hospital. The contents of the workshop, the questionnaire, and the educational pamphlets matched and included educational objectives, sepsis principals, nosocomial infections and sepsis, and prevention, treatment and nursing care in sepsis. The educational content was prepared using reliable resources. It was presented as a Microsoft PowerPoint slideshow by a 5-member team including an anesthesiologist, an intensive care expert, 2 professional nurses (with PhD and MSc degrees), and one of the researchers. The test group was divided into 4 subgroups of 8. A patient with sepsis was then introduced to each subgroup who analyzed the disease and related nursing process. The final conclusions were explained by representatives of subgroups.
The questionnaires were simultaneously distributed among the study subjects before and immediately and 3 weeks after the educational workshop (although the control group received no education). At the end of the educational workshop, considering the information level of subjects, some sources were introduced to them. They were also provided with an educational pamphlet. It is however noteworthy that for ethical considerations, after the end of the study, the control group received similar education (i.e. class and pamphlet).
In data analysis, mean and standard deviation, chi-square test, independent t-test, and repeated measures analysis of variance (ANOVA) in SPSS18(SPSS Inc., Chicago, IL, USA) were used. The statistical significance was determined as p < 0.05.
Limitations and Ethical Considerations
Limitations of the study included differences in features of ICUs in terms of facilities, equipment, and type of patients. In addition, subjects could achieve different levels of information through mass media, books, or articles which consequently influenced the study. These limitations however, could not be controlled by the researchers. During the study, the researchers remained committed to ethical values since the subjects were human beings and respecting their rights was necessary.
FINDINGS
Sex and employment status of the study subjects were reviewed by chi-square test. In addition, age and work experience were compared through independent t-test. The results showed that the two groups had no significant differences in terms of age, sex, work experience, and employment status. The two groups were thus justified based on the mentioned variables, i.e. random allocation of variables could control some confounding factors.
Independent t-test indicated that mean scores of knowledge, attitude, and practice of ICU nurses in the test and control groups had no significant differences before the intervention (Table 1). In addition, comparing the mean scores of knowledge, attitude, and practice of the control group before and immediately and 3 weeks after the intervention using repeated measures ANOVA showed no significant differences (p > 0.05) (Table 1). In the test group however, mean scores of knowledge significantly increased immediately after the intervention (Table 1). In contrast, no significant changes were observed between mean scores of knowledge immediately and 3 weeks after the intervention. Besides, the mean scores of attitude increased immediately after the intervention and the trend continued until 3 weeks later. Moreover, mean scores of practice of the test group significantly increased immediately after the intervention but did not change during the next 3 weeks. These changes indicated the stable impacts of education on promoting knowledge, attitude, and practice of nurses after 3 weeks.
Table 1.
Mean scores of knowledge, attitude, and practice of intensive care unit nurses before and immediately and 3 weeks after the intervention in the test and control groups
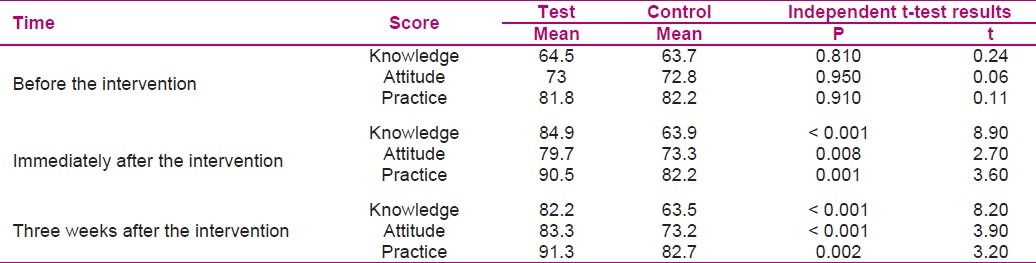
According to independent t-test, mean scores of knowledge, attitude, and practice of ICU nurses in the test group were significantly higher than the control group immediately and 3 weeks after the intervention (p < 0.05) (Table 1).
DISCUSSION
We assessed mean scores of knowledge, attitude, and practice of ICU nurses before and immediately and 3 weeks after an educational workshop. We also found significant improvements in knowledge and skill of study subjects after education. Furthermore, there was a strong correlation between attitude and education. In other words, after the education, the study subjects developed a more positive attitude. In a study by Tromp et al. in Netherlands, the knowledge scores of participants about sepsis increased after the education and remained stable until 4 to 6 months later.[26] Although similar to the study of Tromp et al. in terms of knowledge scores, our study had a low number of subjects and re-evaluated the participants after a very short period (which are considered as study limitations). Similarly, in a Turkish study, Yilmaz et al. evaluated the effects of education on knowledge and practice of nurses before and immediately and 3 months after the intervention. They reported levels of knowledge and practice of the staff had slight increments immediately after education and at the beginning of the third month. Surprisingly, the levels increased by 2.08 folds after the third month.[16] In the present study, the scores of attitude of the test group 3 weeks after the intervention were higher than the scores immediately after the intervention which indicated the positive effects education on their attitude toward sepsis. However, knowledge and practice were stable 3 weeks after the intervention compared to immediately after it which again reflect our limitations i.e. short educational course and lack of theoretical and practical involvement of nurses with sepsis in ICUs.
Therefore, it can be concluded that passing time does not negatively affect knowledge, attitude, and practice of the subjects. In fact, it can even lead improve and promote the mentioned variables if education is continuous. Therefore, although many studies have reviewed the effects of education on knowledge, attitude, and practice at various time intervals, continuous education at work can overshadow other factors. Educational courses on sepsis should hence be given more attention.
The findings of this study showed that mean scores of knowledge, attitude, and practice of ICU nurses immediately and 3 weeks after the intervention were significantly higher in the test group compared to the control group (Table 1). Our results were in accordance with the findings of Ghorbani et al. on knowledge and attitude of nurses about acquired immune deficiency syndrome (AIDS) in Tehran, Iran.[27]
Previous research has indicated that among the obstacles in implementation of care guidelines in treatment of sepsis are lack of motivation, awareness, and acceptance toward managing this disease. Therefore, introducing sepsis care programs not only does progress the acceptance of documented recommendations provided about sepsis, but also can reduce its related mortality. Comprehensive knowledge about this disease is thus an important condition for early diagnosis and treatment.[28]
CONCLUSION
The results of the present study showed that sepsis care education was effective on attitude, knowledge, and practice of ICU nurses. According to the findings of the present study, hospital nurses can participate in educational programs and promote their knowledge in this regard and consequently carry out the appropriate and correct care of patients. The results of this study can be a basis for future activities and a source for further research about sepsis.
ACKNOWLEDGMENT
Hereby, many thanks and appreciations go to all individuals who helped us in conducting this study, particularly the esteemed professors of School of Nursing and Midwifery of Isfahan University of Medical Sciences, and managers and staff of intensive care units of Shariati Hospital, Isfahan, Iran.
Footnotes
This Article was derived from an MSc in Isfahan University of Medical Sciences, Isfahan, Iran, No: 390258
Source of Support: Isfahan University of Medical Sciences
Conflict of Interest: None declared.
REFERENCES
- 1.Rubulotta FM, Ramsay G, Parker MM, Dellinger RP, Levy MM, Poeze M. An international survey: Public awareness and perception of sepsis. Crit Care Med. 2009;37(1):167–70. doi: 10.1097/ccm.0b013e3181926883. [DOI] [PubMed] [Google Scholar]
- 2.Javadi AA, Mobasherizadeh S, Soroushnia M, Bahman Ziari F, Shahrokhi SH. Prevention from nosocomial infections, World Health Organization. Tehran: Salman Publications; 2004. [In Persian] [Google Scholar]
- 3.Marino P. In: The comprehensive book of ICU. Asgari MR, Soleimani M, translators. Tehran: Boshra Publication; 2008. [Google Scholar]
- 4.Reinhard KR. The Role of the acute nursing practitioner in the early identification and management of sepsis [MSc Thesis] Arizona: College of Nursing, The University of Arizona; 2008. [Google Scholar]
- 5.Santhanam I, Kissoon N, Kamath SR, Ranjit S, Ramesh J, Shankar J. GAP between knowledge and skills for the implementation of the ACCM/PALS septic shock guidelines in India: is the bridge too far? Indian J Crit Care Med. 2009;13(2):54–8. doi: 10.4103/0972-5229.56049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Giuliano KK, Kleinpell R. The use of common continuous monitoring parameters: a quality indicator for critically ill patients with sepsis. AACN Clin Issues. 2005;16(2):140–8. doi: 10.1097/00044067-200504000-00004. [DOI] [PubMed] [Google Scholar]
- 7.Steen C. Developments in the management of patients with sepsis. Nurs Stand. 2009;23(48):48–55. doi: 10.7748/ns2009.08.23.48.48.c7203. [DOI] [PubMed] [Google Scholar]
- 8.Robson WP. From A&E to ICU: how nurses can support the Surviving Sepsis Campaign. Intensive Crit Care Nurs. 2004;20(3):113–5. doi: 10.1016/j.iccn.2004.04.002. [DOI] [PubMed] [Google Scholar]
- 9.Zadsar M. Sepsis Syndrome and New Therapeutic Horizons. Bulletin of Blood Transfusion in North of Tehran, No 54 [Online] 2010. Available from: URL: www.ibto.ir/ [In Persian]
- 10.Kleinpell R. Advances in treating patients with severe sepsis. Role of drotrecogin alfa (activated) Crit Care Nurse. 2003;23(3):16–29. [PubMed] [Google Scholar]
- 11.Ely EW, Kleinpell RM, Goyette RE. Advances in the understanding of clinical manifestations and therapy of severe sepsis: an update for critical care nurses. Am J Crit Care. 2003;12(2):120–33. [PubMed] [Google Scholar]
- 12.Campbell J. The effect of nurse champions on compliance with Keystone Intensive Care Unit Sepsis-screening protocol. Crit Care Nurs Q. 2008;31(3):251–69. doi: 10.1097/01.CNQ.0000325050.91473.0b. [DOI] [PubMed] [Google Scholar]
- 13.Ouls L, Siment A. In: Health education, Practical tips for health seekers. Shidfar M, translator. Mashhad: Siavash Publication; 1993. [Google Scholar]
- 14.Nikravan Mofrad M, Shiri H. Nursing Care in ICU. Tehran: Nour-e-Danesh Publication; 2008. [In Persian] [Google Scholar]
- 15.Hosseini Shamlou S. Reviewing the effect of in-service education on knowledge, attitude and practice of healthcare workers about controlling nosocomial infections in hospitals affiliated to Iran University of Medical Sciences and Health Services. Journal of Nursing and Midwifery, Iran University of Medical Sciences. 1996;14–15:68–79. [In Persian] [Google Scholar]
- 16.Yilmaz G, Caylan R, Aydin K, Topbas M, Koksal I. Effect of education on the rate of and the understanding of risk factors for intravascular catheter-related infections. Infect Control Hosp Epidemiol. 2007;28(6):689–94. doi: 10.1086/517976. [DOI] [PubMed] [Google Scholar]
- 17.Plambech MZ, Ipsen HL. Intervention to improve screening andtreatment of sepsis. Scand J Trauma Resusc Emerg Med. 2010;18(Suppl 1):P17. [Google Scholar]
- 18.Nikpour B. Health Management and Planning. Tehran: Tehran University Press; 1989. [In Persian] [Google Scholar]
- 19.Weprey P. In: Nursing Principles and Techniques. Asadi Noghabi A, Shiri M, Zebardast A, translators. Tehran: Boshra Publications; 2010. [Google Scholar]
- 20.Mohammadi GH, Ebrahimian A, Mahmoudi H. Assessing nurses’ knowledge in intensive care units. Journal of Critical Care Nursing, Semnan University of Medical Sciences. 2009;2(1):41–6. [In Persian] [Google Scholar]
- 21.Robson W, Beavis S, Spittle N. An audit of ward nurses’ knowledge of sepsis. Nurs Crit Care. 2007;12(2):86–92. doi: 10.1111/j.1478-5153.2007.00210.x. [DOI] [PubMed] [Google Scholar]
- 22.Entezari M. Reviewing the prevalence rate of sepsis and septic shock and its clinical course in patients admitted in ICU of Fatemi Hospital in Ardabil, 2000. Proceedings of the 3rd Iranian Congress of Intensive Care Medicine; 2003 Oct 30-Noov 1-2; Isfahan, Iran. 2003. [In Persian] [Google Scholar]
- 23.Hajibagheri K, Afrasiabian SH. Epidemiologic study of nosocomial infections in hospitalized patients in the ICU and post-ICU and its associated factors in Tohid Hospital in Sanandaj. Scientific Journal of Kurdistan University of Medical Sciences. 2005;10(4):44–50. [In Persian] [Google Scholar]
- 24.Durthaler JM, Ernst FR, Johnston JA. Managing severe sepsis: a national survey of current practices. Am J Health Syst Pharm. 2009;66(1):45–53. doi: 10.2146/ajhp080067. [DOI] [PubMed] [Google Scholar]
- 25.Ziglam HM, Morales D, Webb K, Nathwani D. Knowledge about sepsis among training-grade doctors. J Antimicrob Chemother. 2006;57(5):963–5. doi: 10.1093/jac/dkl042. [DOI] [PubMed] [Google Scholar]
- 26.Tromp M, Sleeker-Rovers CP, van AT, Kullberg BJ, Hulscher M, Pickkers P. Internal medicine residents’ knowledge about sepsis: effects of a teaching intervention. Neth J Med. 2009;67(9):312–5. [PubMed] [Google Scholar]
- 27.Ghorbani GA, Alishiri GH, Jonaidi N, Esfahani AA, Hosaini MJ. Effect of education on knowledge and attitude of nurses about AIDS 20 years after its epidemic in Iran. Iran J Infect Dis Trop Med. 2006;11(35):85–9. [In Persian] [Google Scholar]
- 28.Vandijck DM, Blot SI, Vogelaers DP. Implementation of an evidence-based sepsis program in the intensive care unit: evident or not. Crit Care. 2009;13(5):193. doi: 10.1186/cc8056. [DOI] [PMC free article] [PubMed] [Google Scholar]