

Abstract
Background:
Each group or profession has its own discourse. Discourses create identity, support institutions and reproduce power relationships. Professional identity of Iranian nurses, which has recently had the opportunity to represent itself in social arena, needs investigation. This study aimed to make internal aspect of this identity clear.
Materials and Methods:
This study was conducted by discourse analysis, using data of 23 semi-structured individual interviews and 4 focus group interviews with nurses and senior nursing students of Tehran and Isfahan University of Medical Sciences, Iran, to evaluate their professional identity.
Findings:
In professional self-concept, elements like spirituality value and low financial benefits were identified as well as conflicting features of holiness and humility, identity emerging, identity escape, low professional self-confidence and justice seeking, lost professional authority and pride.
Conclusions:
Nursing professional identity has been formed based on cultural social structure, values and beliefs governing health system. This is a spectrum of a growing and emerging identity to a developed but forgotten identity. Although nursing discourse is subordinate in health system discourse, signs of moving toward professional maturity have emerged.
Keywords: Professional identity, nursing, discourse analysis
INTRODUCTION
Asking about what and who, and attempting to find answers to the question of “Who am I?” has created ‘identity’. Identity is not hereditary, inborn or natural, but it forms by trying, discussing, negotiating, especially in dominant-subordinate relationships, and integrating with historical conditions and in group experience. From sociology viewpoint, identity is formed by interaction via culture and discourse.[1]
Social identity has an important role in developing a society. A society without identity has low self-esteem, has underdeveloped ethical reasoning, suffers from serious interpersonal problems, is not faithful to its values, and depends on alien identity. Individuals forget organizational benefits, and replace public interests with their private ones and feel less intimate with people in his group. Identity is the prerequisite of social action and necessary condition for development and a source of meaning for social activists.[2]
Professional identity is a form of social identity which is related with group interactions at workplace and how people compare themselves with other professional groups and make distinctions. Professional identity includes acquiring insight to professional functioning, creating professional ideals and values. It can be defined as attitudes, values, knowledge, beliefs, and skills that are common among a professional group. Professional identity is related with professional roles a person can take in that profession.[3] Professional identity is nurses’ concept of nursing and functioning as a nurse.[4] This identity includes individual’s experience, and feeling of oneself as a nurse (self-concept), and others’ image of that person as a nurse (social image).[5]
Professional identity is the foundation for professional functioning and different roles in nursing. Nurses who have obtained professional identity are more flexible when facing with role changes.[6] Realizing the way nurses create their identity is essential because it impacts the determination and development of their roles in future.[7] Clarity and desirability of roles leads to professional identity for the practitioners of that profession; on the other hand, ambiguity and undesirability of the roles leads to loss of professional identity. It seems that nurses cannot improve their functioning and care of patients unless they have a clear, appropriate and acceptable concept of their profession’s nature, its borders and professional roles. The results of a study in Iran showed that most of the nurses knew little to average about their professional roles.[8]
Formation of professional identity begins at the time of studying, and is expected to be one of the outcomes of professional socialization of nurses in the early educational programs,[9] and continue in their professional life.[5] Professional socialization is a complicated process through which individual’s knowledge, skills and professional identity are acquired. This process is made possible through work experiences and roles and creates professional identity.[3]
Nursing has changed its professional training pattern form traditional hospital based training to modern university based training in an attempt to acquire a proper identity and status. The shift from internship in hospitals to university education is the most important approach to improve professional status of nurses.[10] Nursing education in Iran, along with the global movement, entered universities 3 decades ago. Professional socialization process requires role models for newcomers so they can obtain the appropriate identity.[3] The university model of a nurse presented by nursing teachers is based on nursing theories, nursing process and patient’s special care. This image is in contrast with what students face in practice. Despite its huge advantages in professional perspective, it has made students confused.[11]
Having a specific body of knowledge is an important criterion of a profession.[12] Lack of specific professional knowledge in nursing causes biomedical paradigm domination in health science education including nursing. Values of nursing are seldom recognized in health system because medical values and models have been accepted as normal. Professional identity of nursing is overshadowed by medicine which considers all health arenas its legal territory. Furthermore, nursing is always being compared with medicine, which leads to a feeling of professional inferiority.[13] Applying biomedical model in teaching nursing has distorted professional nursing territory and identity. A local study showed that most of the nursing students did not have the right image of nursing and considered it related to medicine.[14]
Nurse’s self-concept is closely related to social image of nursing. A study showed that Iranian nurses are considered physician’s assistant both in professional and social grounds. They have weak social image and inappropriate social status.[15] Another study showed that only 9.6% of nurses considered society’s opinion of nursing as favorable and 44% considered it bad.[16] A study on nursing and non-nursing students showed that from their perspective, nursing has low to moderate social status. Nursing students feel that nursing does not have appropriate social status more than other students.[17] Most of the nursing drop-outs claim their main reason to drop out was lack of social acceptance, misunderstanding and inappropriate atmosphere of nursing.[18] Another study found the following as the main social factors in nurse’s leaving their jobs: wrong concept of nursing in society, projecting the nonscientific image of nursing in media, lack of social status for nurses, lack of suitable relationship between peers, lack of professional attraction in society and lack of nurses’ family knowledge of the profession.[19]
Despite undeniable progresses of nursing in Iran, it seems that nurses have a lot of problems with their jobs and are not proud of being a nurse. Nurses are embarrassed to say they are a nurse even in their family or to their parents.[20] Even nursing teachers doubt their efficiency and independence.[21] These are some presentations of disturbances in professional socialization and acquiring processional identity in Iranian nurses that mandate a study on nursing professional identity. With regard to the difference in social and cultural conditions, both the context in which nurses work, and how they act as a nurse should be studied to realize professional identity of nurses.
The question of how Iranian nurses’ professional identity is, remains one of the concerns of nursing thinkers. The researcher believes that by knowing nursing discourse, actions and reactions of the members of this profession can be predicted in certain situations and be directed even before they are expressed; something that is called identity management or memetics these days.[2]
The researcher’s main concern is recognizing identity elements (genes) in order to achieve a practical solution in professional memetics. He wants to re-recognize professional nursing identity in order to re-construct professional identity concept on the basis of esthetic, inborn and cultural ethical values.
MATERIALS AND METHODS
This article was extracted from a PhD thesis, where nursing professional identity was studied from self-concept perspective using discourse analysis. Identity is a discourse based phenomenon, and is represented in relationships and interactions. The focus of discourse analysis is on the manner of construction of social relationships, identities, knowledge and power in oral and written texts.[22] Therefore, discourse analysis was used to examine nursing professional identity. In this study, a post-structuralism hybrid method of Laclau and Mouffe, and Fairclaugh approach was used to analyze texts. The reason for using hybrid method was the Laclau and Muffe approach, which is a macro scale approach, and does not contain detail tools for text analysis. In contrast, Fairclaugh approach has precise and detailed tools for text analysis.
Participants were nurses and nursing students selected from two major educational centers in Iran, that is, Tehran University of Medical Sciences, and Isfahan University of Medical Sciences. The study population comprised of 20 nurses in different ranks of 8 clinical nurses, 5 head nurses, 2 supervisors, one nursing manager and one faculty member, one member of the board, 2 nursing students and 3 physicians including one general practitioner, one resident and one faculty member. Furthermore, 4 focus groups comprising of 3 female clinical nurses, 4 male students, 8 female students and 4 female students were among participants. Preliminary analysis of interviews showed that from nurses’ viewpoint, physicians were considered ’others’. Because of this viewpoint, the researcher interviewed 3 physicians as participants in order to familiarize with physician’s discourse.
The researcher entered the research environment after obtaining necessary permits. All participants signed informed written consent to enter the study. Data were collected by semi-structured interview and by using lead questions. The interview began with main questions like ‘What does nursing mean to you?, ‘How do you feel about being a nurse?’, ‘What qualities does your model nurse have?’, and continued with open questions. Interviews were scheduled at participants’ convenience in their office or researcher’s office. Each interview took 45 to 120 minutes. With prior permission from the participants, all interviews were recorded using an MP3 IC recorder, notes were taken during the interview and the scripts of interviews were immediately transcribed verbatim.
In order to analyze interview texts, several text analysis techniques like determining the themes, word selection, collocation, determining the key signifiers, contradictory poles, and intertextuality were used.
During discourse analysis, the researcher continuously moves from surface to the depth of the text. Superficial analysis is concerned with vocabulary and linguistic properties of the text while deep analysis is concerned with hyper-textual properties, that is, cultural and social structures of the text.[23] That is why, simultaneous with text analysis, the researcher made extensive review of literature of women’s sociology, nursing and medicine sociology, and nursing history.
Text analysis was conducted based on researcher-made algorithm (Figure 1). On the basis of this algorithm, text was read several times to determine the themes. Then, text was read word by word and line by line to determine textual properties such as collocations (words that accompanied ’nurse’ and ’nursing’), word.
Figure 1.
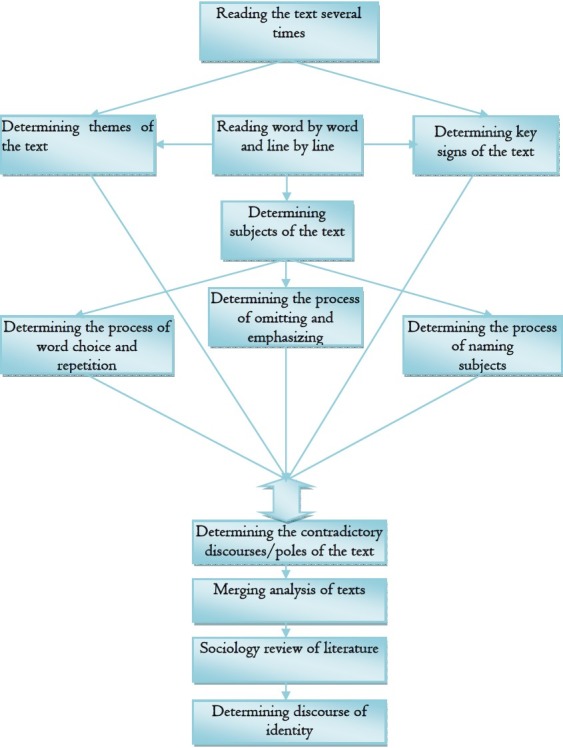
Algorithm of interview analysis
Selection (adjectives and verbs attributed to nurses), word repetition (repetition of words in the text), signifiers and poles of the text which reflected the identity of nurses and nursing; these properties along with pieces from the text that represented such properties were entered into text analysis tables. The results of the analysis of each text were recorded in a separate table and finally, the results were merged, data were reduced, and common and main elements were extracted. At this stage, findings of text analysis were compared and contrasted with similar texts in sociology evidences.
With regard to validity and reliability of the data, post--structural paradigm considers internal and external validity, reliability and credibility as attempts to gain authority in a text. From post-structuralism view, a text is valid if it has grounded deep into its data, is based on naturalistic criteria, is meticulously paired with the related theory and paradigm, is honest and logical based on the reflection of that phenomenon. The rigor and validity of a text lies in its representation in the social world under study.[24] Discourse analysis recognizes several interpretations of a text, but the process of interpretation should be appropriately supported by theory, the analyzed text should be proportional to the research question, data collection and analysis should suit the selected paradigm, and a complete description should be made of the collection and analysis of data.[22] The researcher tried to design questions, analysis method, data collection method, and interpretation of results and implement the research by considering philosophical foundations and methodology of post-structuralism discourse analysis so that the study has the rigor, confidence, credibility, truth, conformability and perfection. The researcher utilized all his efforts, commitment and creativity to fulfill these requirements.
Samples were selected as many as was sufficient. To do so, 27 individual and group interviews were arranged with different ranks of nurses. During data analysis, the researcher merged in the data to form a new understanding of the nursing discourse. During the study, emphasizing on a deep understanding, maintaining the quality of the data, and observing the right trend of the study, the legitimacy and acceptability of the researcher were considered as a vital principle in discourse analysis.
To protect individual’s rights, and observe ethical principles of research, the following steps were considered: all permits were taken for the research, objectives and procedures were explained to the participants, informed consent was taken from participants to do the interviews, all the information was kept confidential, participants’ identities were hidden, participating was voluntary, participants could exit the study at any time, the copyright of other authors were observed.
FINDINGS
In studying professional self-concept of nurses, what was heard from most nurses was familiar discourse, and I was inside the discourse because of my position. That is the reason that this study is a kind of internal view to this discourse. In nursing discourse, ‘professional alienation’ represented itself in different ways in nurses’ statements. I called this prevalent expression ‘identity meta-narration’ of the Iranian nurse. Iranian nurses do not know who they are, why they have entered this profession, and what the values of their profession are. That is why they feel they are at loss. This identity crisis is what Mowlana (Mewlana), the famous Persian poet represents in his poem: ‘Where have I come from? Why have I come? Where am I going now….?’ These are some of statements.
Nurse N4: ‘When I’m tired and angry, I insult nightingale. To tell the truth, I say, Goddamn her to found this profession.’
Supervisor S1: ‘A guy said he wanted to bring his daughter to the hospital to work before she got married. I told him no way! Don’t do it! You’d ruin her fortune this way. Don’t let her be labeled as someone who worked in a hospital. People say she was a nurse in a hospital.’
Student P7: ‘My mom with 28 years of experience (of nursing) told me, ’Mahshid, when you enter this job, beware! Your colleague, who is your best friend, will stab you in the back, rest assured. I mean my mom had the experience and said it to me straight forward.’
Member of the board NP: ‘Something that has created controversy is that the young community of nurses as it is…. There are probabilities. One of these probabilities is that it does not believe its profession, disbelief. It doesn’t believe profession’s values. It does not have the outlook of the profession. Like what nursing says in the world. Like what it says in Iran. It doesn’t know its objective. It doesn’t know professional responsibilities.’
During the analysis of the interview transcripts, a look at the themes resulted in a general discourse of nursing. Themes of individual interviews contained issues like spirituality value of nursing, hardship of nursing, inappropriate social view of nursing, feeling of identity, and feeling of oppression. In students and those with less experience, the feeling of identity was less expressed, and the feeling of professional inferiority and oppression was prominent while in those with more experience, especially those in management, the feeling of identity was stronger. In group interviews, the main themes were hardship of nursing, spiritual value of nursing on one side and lack of power and support, feeling of professional inferiority, and inappropriate social view of nursing on the other side. The feeling of professional identity, and emphasis on professional values were less evident, and identity crisis was presented more vividly in nurses’ and especially students’ statements. Studies in other countries show the challenges of identity in nurses. Chinese nurses have low professional self-confidence, which is mostly due to the lack of social respect.’[25] Armenian nurses did not have developed professional identity and organization, so they did not have any outlook for their profession.[26]
Analysis of the interviews on textual property of collocations showed that certain words are associated with nurse and nursing. Some of them like ‘undisputed governor of the ward’, jack of all trades’, and ‘strong’ considered the nurse full of power and identity, while some like ‘powerless’, ‘convicted’, ‘interns’ and residents’ foot person’, ‘escape goat’, ‘doll’, ‘doctor’s flunky’, and ‘ward secretary’ introduced her as without power and identity. Some words like ’angel of mercy’, and ‘service provider’ have discursive concept. Based on this part of analysis, it can be concluded that even nurses do not have a homogeneous and appropriate description of their identity. Interestingly, they stress their emotional aspects more than scientific and specialized ones. Nursing characteristics swung within a spectrum which harbored spiritual, humane and divine values on one side, and materialistic and earthly values on the other. Stress was placed more on emotional and humane aspects rather than professional and scientific ones. The word ‘nurse’ had a gendered bias and was mostly described in a ‘feminine’ fashion. A study in Scandinavia showed that professional identity represents in a spectrum of maturity and sophistication with two opposite poles of strong and weak professional identity. The nursing professional identity is mainly constituted of compassion, qualification, certainty, conscience, commitment, and bravery.[5]
The analysis of interviews with regard to property of word selection showed the language and culture of nursing and portrayed the geography of nursing discourse. Words express unpleasant and difficult work conditions. A job that not only has a difficult nature and is bound with ‘stress’, ‘sheet’, ‘bed pan’, ‘injured’, ‘patient’s resuscitation’, and ‘comatose patient’, but also harbors the conditions of ’ stab in the back’, ‘pull the rug from under your feet’, ‘resident’s insult’, ‘patient’s family’s insult’, ‘coworker’s enmity’, ‘being under control’. The only thing that keeps nurses strong is reliance on ‘spiritual values’ and ‘spiritual satisfaction’. A look at these words shows that this is not a powerful discourse, but a marginalized discourse and being dominated. Despite spiritual, humanity and ethical values of the profession, inappropriate social outlook is not in line with these values. The following examples of nurses’ statements show this:
Nurse N4: ‘People think that nurses are, excuse me, harum-scarum and lazy, who just pay attention to their appearance, and are not hard working at all. When I meet some families, as a nurse who studied 4 years and has a lot of knowledge, they don’t know what I do; they think I just give patients shots. It’s not yet realized.’
Nurse N5: ‘I like my major. I love my job, helping the greatest of God’s creation is satisfactory. When I help people, I feel satisfied. I like to grow in it and help the society, and develop my profession, too. But financial and spiritual aspects should go together. Nursing is good, but its social value is below zero. It’s one of the most difficult jobs because you have to deal with people. It’s full of stress. You have to dedicate yourself and all you have to people, just for God’s sake. When a nurse doesn’t have enough income, nor does she have a descent holiday, nor social value, well, it makes you hopeless.’
Repetition of words in texts shows the importance and high status of that word, and the semantic system of the discourse. The analysis of interviews with regard to word repetition showed that words like ‘job difficulties’, ‘fatigue’, ‘hardship’, ‘expectations’, ‘spiritual value’ of the profession have been repeated frequently. Some other such words are ‘care’, ‘health’, ‘sacrifice’, ‘love’, ‘emotion’, ‘help’, ‘service’, ‘self-dedication’, ‘ethics’, ‘humane’, ‘devotion’, ‘science’, ‘justice’, and ‘client’s rights’, some of which are values of the profession. With regard to the central role of these words in the studied discourse, these words are signifiers of nursing discourse. Signifiers comprise semantic system of a discourse, and each has a signified or special meaning in that discourse. Figure 2 shows semantic system and key signifiers of nursing discourse in interviews.
Figure 2.

Semantic system and key signs of nursing discourse in interviews
The subjects of nurses’ statements are mostly nurses and doctors. Nurses consider doctors powerful and dominant in health system, and with social status, and they consider themselves powerless and oppressed. However, a general practitioner, and a medicine lecturer have a different opinion and say:
Physician P: [Physician’s] social status has changed so much these days. It’s not like before at all. Once doctors were really special, now it’s not like that at all. Patients’ behavior always shows it to us. Most of the time, we’re humiliated worse than that. That status and holiness is gone. People’s opinion of medicine has changed.
Medicine lecturer MP: ‘You say you are a doctor, but you can imagine that the trust that we had once, is damaged now. Assuming that for example you prescribe a test that might not be that necessary, or prescribe a drug, but you have a deal with the pharmacy.’
Bordering and distinguishing ‘us’ and ‘them’, or 𠆄allied’ and ‘other’ are important discourse parameters. Each discourse, like a group or individual, needs ‘other’ to have identity. In other words, each discourse needs a rival discourse to confront and show its distinct identity. Conflict between the two rivals polarizes the text, and subjects’ mind and words and behaviors. The poles of the interviews showed that nurses usually consider doctors as ‘other’, so nurses’ discourse rivals physicians’ discourse from nurses’ viewpoint.
Ultra textual processes are macro scale social and cultural structures that influence subjects’ behavior and texts. Interviews revealed points like feminine profession, justice, spiritual values, holiness, royal nurse, past discipline, lord and servant relation, working with ’namahram (not intimate)’ patients, mini doctors, medical tyranny among the ultra-textual processes which could not be realized without referring to the context they were in. Nurses’ status and low attitude toward it, roots in cultural and social structures that govern it, and unsaid and unwritten values and beliefs in the context of Iranian culture. These beliefs lead thoughts, and actions of social activists and nurses unconsciously as mental presumptions. Some of these values and beliefs are reflected in Iran in the form of preferring comfort to hard work, material things to spiritual things, high social status to healthy conscience, independence to dependence, superiority to cooperation, fame to purity and anonymity physical pleasure to spiritual satisfaction, and mental work to manual work. Hajilari reported that in the past two decades, Iranian society has inclined to materialistic values like comfort, wealth, economic progress while tendency to ultra-materialistic values has decreased.[27]
DISCUSSION
An important process in each profession is creation and development of professional identity.[28] Realizing nurses’ professional identity is not possible unless through recognizing nursing discourse. Nurses are a member of the complicated health system, whose discourse directs their actions and statements. The dominance of medical discourse on health system and even in social arena has medicalized a lot social problems, which receive medical prescriptions. Medicalization of society means medical model has taken social problems like alcoholism, psychological problems and addiction into its territory.[29]
The results of this study showed that professional values which are basis of professional identity have not been institutionalized in nursing discourse. Nursing professional identity is going through its pre-maturity period, which I called ’infant professional identity’. Furthermore, signs of a decent but forgotten identity was seen in nursing (nurses who were trained before Islamic Revolution), which I called ’professional identity with Alzheimer’. Nursing discourse is marginal in our health system, but recent establishment of professional organizations, and scientific development of nursing, signs of a movement of a novel and infant identity discourse has emerged. The dominance of medical discourse in health system has made it impose its values on educational system through biomedical paradigm. So, instead of training nurses with strong identity (super nurses), it has trained self-alienated nurses (little doctors), who not only do not feel professional decency, but also have forgotten being a nurse and have caught professional Alzheimer’s. Roberts believes nursing values in the field of caring are seldom recognized because medical values and models have been recognized as suitable and institutionalized. The nursing identity has been overshadowed by medicine, which has made all areas of health its own territory.[30]
Our findings showed that nurses do not show appropriate self-concept that indicates distinctive and developing identity. They range on two extremes of spirituality-materialism spectrum, that is; they either extremely focus on the spiritual and sacrificial aspects of their job in a way that the scientific and professional aspects are overshadowed or extremely stress the hardships of their profession and materialistic demands. Misuse of values and extreme emphasis on concepts like sacrifice and devotion by others, is sometimes, not out of belief and respecting the profession, but in line with the idea of ‘heavenly profession’ and justifying the unpleasant work conditions of nurses.
Analyzing vocabulary of health system, I realized that some words have discursive power and others do not. Words like medicine, physician, treatment, disease, drug and diagnosis are associated with science, and accompany a kind of superiority and power. On the other hand, words like care, nursing, nurse and health are marginalized and not associated with science. The word ‘nurse’ indicates non-scientific service providing, which seems to have impacted its low social status because of this historical semantic load. Words like ‘white coat angel’, ‘angel of mercy’, ‘earthly angels’, and ‘holy’ which are used to describe nurses emphasize the emotional aspect of the profession, not its scientific value.
Nursing discourse needs to break the norms of its own and its rival’s discourse in order to project a desirable image of nurse. Words like medicine and treatment, which have been given special privilege because of their identity and omitting others (nursing and care), need to be deconstructed.[31] Accompanying words ‘nurse’, and ‘nursing’ with new scientific and specialized concepts instead of current traditional ones in media and society can deconstruct the norms of these words and reconstruct them. Furthermore, nurse and nursing should be avoided in combination with words that are associated with traditional definitions of nursing, for example, ‘home nurse’, and ‘baby nurse’. Reconstructing professional identity of nurses is possible through stressing professional roles, describing nursing by these roles and using words that introduce scientific, professional and ethical characteristics of nurses. In this regard, emphasis on professional functioning of nurses and projecting a professional image that harbors characteristics like responsibility, responsiveness, observing professional ethics, establishing human relationships, defending the client, having specialty knowledge can deconstruct norms and reconstruct social image of nurses. The feedback from improved social image can improve professional self-concept of nurses, which will develop nursing professional identity.
Although the project of otherness making of medicine is in some ways the first step of identity seeking, remaining in this step fails the identity seeking. In order to enhance professional identity, inter-professional cooperation in the form of health team is necessary. This cooperation represents professional identity in professional and inter-professional functioning. ‘The last step of professional identity seeking is working in inter-professional groups, and respecting each other’s cooperation.’[30] If medicine and nursing, i.e., doctor and nurse, are considered complementary and interactive rather than rival and contradictory, their synergistic functioning can guarantee health of the patients and the society. ‘Each one (doctor and nurse) gets its existence by interacting and complementing each other. Both create harmony and balance by cooperating. Although they are on opposite sides, they need each other and do not need to confront each other.’[31]
It seems reaching a developing professional identity needs formation of a strong and new discourse, which contains articulation of signifiers extracted from the nature of the profession, and also signifiers that are acceptable in discourse system of the society like health, client, defending client’s rights. Such a discourse may get out of the margin and enter the center of health system. The developing nursing professional identity based on professional roles can emerge out of this discourse. The formation of this discourse needs a common language and culture in the first place, and then representatives, speakers and organizations that represent this discourse and develop it.
Footnotes
This article was derived from PhD dissertation in the Tehran University of Medical Sciences
Source of Support: Isfahan University of Medical Sciences
Conflict of Interest: None declared.
REFERENCES
- 1.Miers M. Gender Issues and Nursing Practice. London: Palgrave MacMillan; 2000. [Google Scholar]
- 2.Alikhani AA. Theoretical principles of identity and identity crisis. Tehran: Humanities Research Center; 2004. [In Persian] [Google Scholar]
- 3.Adams K, Hean S, Sturgis P, Macleod Clark J. Investigating the factors influencing professional identity of first-year health and social care students. Learning in Health and Social Care. 2006;5(2):55–68. [Google Scholar]
- 4.Fagermoen MS. Professional identity: values embedded in meaningful nursing practice. J Adv Nurs. 1997;25(3):434–41. doi: 10.1046/j.1365-2648.1997.1997025434.x. [DOI] [PubMed] [Google Scholar]
- 5.Ohlen J, Segesten K. The professional identity of the nurse: concept analysis and development. J Adv Nurs. 1998;28(4):720–7. doi: 10.1046/j.1365-2648.1998.00704.x. [DOI] [PubMed] [Google Scholar]
- 6.Cook TH, Gilmer MJ, Bess CJ. Beginning students’ definitions of nursing: an inductive framework of professional identity. J Nurs Educ. 2003;42(2 Suppl1):311–7. doi: 10.3928/0148-4834-20030701-08. [DOI] [PubMed] [Google Scholar]
- 7.Ewens A. Changes in nursing identities: supporting a successful transition. J Nurs Manag. 2003;11(4):224–8. doi: 10.1046/j.1365-2834.2003.00405.x. [DOI] [PubMed] [Google Scholar]
- 8.Nasiri Moghadam SH. Nurses’ awareness of their roles in hospitals affiliated with Kerman University of Medical Sciences [MSc Thesis] Kerman: Kerman University of Medical Sciences; 1997. [In Persian] [Google Scholar]
- 9.MacIntosh J. Reworking professional nursing identity. West J Nurs Res. 2003;25(6):725–41. doi: 10.1177/0193945903252419. [DOI] [PubMed] [Google Scholar]
- 10.Apesoa-Varano EC. Educated Caring: The Emergence of Professional Identity Among Nurses. Humanities, Social Sciences and LawQualitative Sociology. 2007;20(3):227–49. [Google Scholar]
- 11.Pilhammar AE. Marginality: concept or reality in nursing education? J Adv Nurs. 1995;21(1):131–6. doi: 10.1046/j.1365-2648.1995.21010131.x. [DOI] [PubMed] [Google Scholar]
- 12.Chitty KK, Black BP. Professional Nursing: Concepts & Challenges. 5th ed. Philadelphia: Elsevier Health Sciences; 2007. [Google Scholar]
- 13.Andrist LC, Nicholas PK, Wolf K. A History of Nursing Ideas. London: Jones & Bartlett Learning; 2006. [Google Scholar]
- 14.Adib-Hajbaghery M, Dianati M. Undergraduate nursing students’ compatibility with the nursing profession. BMC Med Educ. 2005;5:25. doi: 10.1186/1472-6920-5-25. [In Persian] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Nasrabadi AN, Emami A, Yekta ZP. Nursing experience in Iran. Int J Nurs Pract. 2003;9(2):78–85. doi: 10.1046/j.1322-7114.2003.00404.x. [In Persian] [DOI] [PubMed] [Google Scholar]
- 16.Jalili M. Problems of nursing based on poll from nurses in the city of Tehran [MSc Thesis] Tehran: School of Social Sciences, University of Tehran; 1986. [In Persian] [Google Scholar]
- 17.Goodarzi M, Masinaie Nejad N, Ildarabadi A, Firoozkoohi M. Social status of nursing from students’ viewpoint. Iranian Journal Of Nursing & Midwifery Research. 2004;9(1):59–65. [Google Scholar]
- 18.Keshavarz A. The reasons for nursing student drop out in nursing faculties of Tehran [MSc Thesis] Tehran: University of Tehran; 1996. [In Persian] [Google Scholar]
- 19.Hooshmand Bhabadi A, Seif H, Nikbakht Nasrabadi A. The reasons for nurses’ quitting their job in a ten year period from 1989-1999. Teb va Tazkieh. 2004;13(4):10–20. [In Persian] [Google Scholar]
- 20.Nikbakht Nasrabadi AR Phenomenology of nature of nursing in Iran [MSc Thesis] Tabriz: Tabriz of University; 2002. [In Persian] [Google Scholar]
- 21.Adib HM, Salsali M. A model for empowerment of nursing in Iran. BMC Health Serv Res. 2005;5(1):24. doi: 10.1186/1472-6963-5-24. [In Persian] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Crowe M, Luty S. Recovery from depression: a discourse analysis of interpersonal psychotherapy. Nurs Inq. 2005;12(1):43–50. doi: 10.1111/j.1440-1800.2005.00250.x. [DOI] [PubMed] [Google Scholar]
- 23.Mirfakhraie T. The process of discourse analysis. Tehran: Media Research Center; 2004. [In Persian] [Google Scholar]
- 24.Denzin NK, Lincoln YS. The Qualitative Inquiry Reader. London: SAGE; 2002. [Google Scholar]
- 25.Smith DR. Nursing in China: Historical Development, Current Isssues and Challenges [Online] 2004. Available from: URL: http://www oita-nhs ac jp/journal/PDF/5_2/5_2_1 pdf/
- 26.Jenkins DL, Brush K, McGonagle E, Vartanian M, Levy K. Expanding the role of nurses in Armenia. J Nurses Staff Dev. 2000;16(3):138–43. doi: 10.1097/00124645-200005000-00008. [DOI] [PubMed] [Google Scholar]
- 27.Hajilari AR. The changes of values after victory of the Islamic Revolution. Tehran: Daftar Nashr Maaref Enqelab; 2006. [In Persian] [Google Scholar]
- 28.Polifko KA, Polifko-Harris K. Concepts of the Nursing Profession. Carolina: Thomson Delmar Learning; 2007. [Google Scholar]
- 29.Adam P, Hertsling Cl. In: Sociology of disease and medicine. Katebi A, translator. Tehran: Nei Publications; 2006. [Google Scholar]
- 30.Roberts SJ. Development of a positive professional identity: liberating oneself from the oppressor within. ANS Adv Nurs Sci. 2000;22(4):71–82. doi: 10.1097/00012272-200006000-00007. [DOI] [PubMed] [Google Scholar]
- 31.Watson J, Dossey BM, Dossey L. Postmodern Nursing and Beyon. 1st ed. Philadelphia: Elsevier Health Sciences; 1999. [Google Scholar]