

Abstract
Background:
Chronic renal disease is a health problem in today’s world. In the end-stages of renal disease patients depend upon alternative therapies including dialysis for their survival. However, dialysis causes several stressors on physical, mental and social performance of patients. The present study aimed to review and compare the self-concept in patients undergoing hemodialysis and peritoneal dialysis.
Materials and Methods:
This was a case-control study including two groups of patients, undergoing hemodialysis and peritoneal dialysis, who referred to Al-Zahra and Ali Asghar Hospitals, which are affiliated to Isfahan University of Medical Sciences. These groups were compared to the control group. Data were collected through completing the form of demographic characteristics and a questionnaire, written by the researcher, pertaining to the self-concept which was collected by the samples. The data were analyzed by the Software SPSS version 18.
Findings:
ANOVA (analysis of variance) showed that statistically there was a significant difference between mean score of self-concept in the three physical (body-image), psychological, and social self aspects in the two groups of hemodialysis and peritoneal dialysis with the control group; however, Duncan’s post-hoc analysis showed no significant difference between mean score of self-concept in the three mentioned aspects in the two groups of hemodialysis and peritoneal dialysis. Furthermore, ANOVA (analysis of variance) showed that there was no significant difference between mean score of the spiritual aspect of the self-concept in the two groups of hemodialysis and peritoneal dialysis with the control group. Duncan’s post-hoc analysis also showed no significant difference in this aspect between the two groups of hemodialysis and peritoneal dialysis.
Conclusions:
Patients undergoing dialysis have many psychological disorders and the type of dialysis is not of much importance in this regard; therefore, adequate education and information for clients in order to use appropriate methods of adaptation as well as appropriate social relationship, continuing social support and developing health policies seem necessary in order to prevent mental disorders and providing required services and supports for patients.
Keywords: Self-concept, hemodialysis, peritoneal dialysis
INTRODUCTION
Chronic kidney disease is a health issue in today’s world which brings about a threatening situation for the economic, social and health status of the diseased individual, and his/her family and society. Thus, in the past few years, it has drawn considerable attention to itself particularly in advanced countries.[1] The importance of such a disease is the dynamic nature of the disease over time and the fact that it will eventually lead to end-stage renal disease.[2] End-stage renal disease is a clinical condition in which the kidneys will not be able to maintain metabolic tasks and keep the balance of the body’s fluids and electrolytes.[3] Using alternative kidney therapies is inevitable for the patients survival.[4]
The prevalence rate of end-stage renal disease has been reported to be 242 cases per one million people[5] and this amount is annually rising by 8%.[6] Currently, there are more than 450,000 people with end-stage renal disease only in the U.S.[7] According to the statistics in Iran, 1200 to 1600 people are annually infected by this disease.[8] According to the report of the principle of the Management Center for Specific Diseases in the Ministry of Health and Medical Education, the population of patients with end-stage renal disease is 32,000 people in Iran[9] which seems to have increased to 40,000 people by 2010.[10] Moreover, according to the studies in Iran, the prevalence rate of end-stage renal disease has increased from 234.49 patients per one million people in the year 2000 to 357.63 patients per one million in 2006.[11]
One of the alternative renal therapies is dialysis, of which there are different types.[4] The aim of undergoing dialysis is to create a balance between acid and base status of blood fluids and electrolytes, as well as to remove the blood’s metabolic waste.[12] Treatment with dialysis (Dialysis Therapy) has two hemodialysis and peritoneal dialysis.[4] hemodialysis is considered as a more common method in the world and Iran.[13] More than 60 percent of patients with end-stage renal disease in the U.S. are treated by hemodialysis.[7] According to the statistics by the Ministry of Health and Medical Education in Iran, 163,372 patients underwent dialysis in 2008, of whom 15,172 patients were treated by hemodialysis. They also reported that 2000 people are annually added to the number of patients undergoing hemodialysis and the number of patients treated by dialysis will be doubled in the next five years.[11]
The other type of dialysis is peritoneal dialysis (PD).[14] Peritoneal dialysis is done in various forms. The most common method of peritoneal dialysis is Continuous Ambulatory Peritoneal Dialysis. Peritoneal dialysis is the optional treatment of those patients with chronic kidney disease who are unable or unwilling to undergo hemodialysis.[4] However, only 8.4 percent of patients with end-stage renal disease tend to perform peritoneal dialysis.[15]
In many cases, diagnosis of chronic renal disease and the necessity of implementing dialysis are a cause of concern for patients and their families and will lead to major changes in the individual’s lifestyle.[4] Dialysis enables greater survival rate of patients,[9] however it causes several stressors on physical, mental and social performance of patients.[16] Current complicated therapeutic methods in Iran have strongly limited the activity of patients undergoing dialysis and have caused a decrease in their energy level, inability, lose of independence, financial stress, sexual dysfunctions, reduction of self-esteem, change in self-concept, and disruption in their family life.[17] For example, they are fully adapted to the stressors[18] and feel they are different from others;[19] therefore, one of the concepts inside patients which is disrupted severely by undergoing dialysis is self-concept.
The Self-concept is one of the profound psychological concepts which is very influential in the patient’s attitude toward a healthy relationship with others, life expectancy, and adaptability to circumstances.[20] Self-concept does not exist from birth, but is acquired during mutual contact with others or with the environment.[21] Self-concept is all the ideas and desires someone has about the identity, values, abilities, and limitations and is changeable.[22]
Carson believes that the self-concept has four physical, psychological, social and spiritual aspects. Carson also believes that the image each person has about her/his own physical image is called the mental image of body.[23] Any change in mental image from body would seriously disrupt the balance of the individual; these changes can be caused by accidents, diseases, or evolutionary changes in the structure and function of the body.[21] Psychological self or personal identity is the combination of perceptual, cognitive, and emotional perceptions someone has of themselves; moreover, sexual identity is also part of an overall sense of identity as well as the self-image someone has as a male or female person. Social self is defined by means of the roles we accept. Role is defined as the pattern of expected behavior related to the individual’s function in a group which is largely influenced by culture.[23] Finally, the spiritual self helps the individual communicate with God so that his/her life is meaningful. This dimension of the self-concept includes the individual’s beliefs about the universe and the position she/he has, and a great sense of hope and love.[23,24]
Chronic renal disease and dialysis therapy have many adverse effects on the mental and physical conditions of people and cause different kinds of deprivations and lifestyle changes such as dependency on others, sexual problems, inadaptability to new conditions and social attitudes,[25] financial problems, lack of employment, limitation in liquid intake and diet, change in familial roles and tasks and reduction in ability to achieve life’s long-term goals,[26,27] anger, depression, anxiety, denial, lack of cooperation, and stress due to physical complications, sense of inefficiency or incompetency, and fear of death.[18]
Studies have indicated that people with chronic diseases could have better adaptability to the disease if they have a positive self-concept. However, their self-esteem would be decreased if they have a sense of uncertainty from the new identity, a negative self-concept, which this negative evaluation would cause.[28] The fact that an individual is the only valid and authoritative reference for his/her own health assessment is gaining the attention of more researchers every day., However, the occurrence of disease will largely destroy the individual’s self-concept.[20]
There are some differences between hemodialysis and peritoneal dialysis in terms of satisfaction of patients, dependency on others, physical changes, ease of implementation, economic status, employment and etcetera. Moreover, peritoneal dialysis is a relatively newer method than hemodialysis. Also due to the existence of differences in ethnic, cultural and social attitudes in Iran, as well as various available resources and facilities for such patients, the present study aimed to review and compare the self-concept in patients undergoing hemodialysis and peritoneal dialysis; because the improvement and promotion of patients’ self-concept can be done only by the identification of these problems.
MATERIALS AND METHODS
This was a case-control quantitative-analytical study conducted in 2010 in Al-Zahra and Ali Asghar hospitals, which are affiliated to Isfahan University of Medical Sciences. Sampling in the peritoneal dialysis group was done randomly among the patients undergoing peritoneal dialysis who had the inclusion criteria. Sampling of the hemodialysis group was done in the same way as the peritoneal dialysis group. For selecting the samples of the control group, the two peritoneal dialysis and hemodialysis groups were randomly asked to introduce some healthy relatives and friends who were close to them in terms of demographic characteristics, socio-cultural and economic conditions, and had no history of renal disease. Thereafter, the introduced individuals (who were 44 people in each group) were asked to complete the demographic data form and a questionnaire.
The inclusion criteria were: Iranian Nationality, Moslem, Persian speaker, having an active hospital record, within the age range of 18–75,[29] ability to complete the questionnaire or interview, no physical or mental disability, lack of acute physical or mental diseases during the study,[30] BMI less than 30,[31] no severe crisis in their life during the past six months, treated by dialysis for at least three months and no renal transplantation surgery.[32] Provided that due to any reason, any of the patients who was not willing to continue the participation, and/or did not answer the questionnaire completely, or had the inclusion criteria but was about to perform the kidney transplant, was excluded from the study.
Data collection tools included a demographic data form and a questionnaire. Demographic data form included age, marital status, BMI, education, current employment status, family income, and the cause of their end-stage renal disease. The used questionnaire was written by the researcher and was pertaining to self-concept in patients undergoing dialysis. The researchers designed the questionnaire by referring to the existing scientific resources and articles, and inspiration by the self-image inventory from Rogers and Beck Self-concept Scale. Scoring was done based on the 5-degree Likert scale (from zero to four representing never, seldom, sometimes, often, and always) so that score 4 was the most desirable score and zero was as the most unfavorable score in each question.
Validity of the tool was determined through the comments of experts and scientists in this regard, and content validity. The reliability was calculated to be 96.7% according to the Cronbach’s alpha coefficient. All the obtained data were encoded through inferential and descriptive statistical methods and were analyzed by the Software SPSS version 18. Error rate was considered to be 5%. ANOVA (analysis of variance) was used to compare the mean score of self-concept in different aspects in the three groups.
FINDINGS
Mean age (SD) in the hemodialysis, peritoneal dialysis and control groups was 45.6 (15.2), 48.2 (12.7) and 43.8 (14.8) years, respectively. In the groups undergoing hemodialysis, and peritoneal dialysis and the control group there were 21 (46.7%) female and 24 male (53.3%), 16 female (35.6%) and 29 male (64.4%) and 24 female (54.5%) and 20 male (45.5%) participants, respectively. In total there were 61 female (45.5%) and 73 male (54.5%) participants. The majority of the participants in hemodialysis, peritoneal dialysis and control groups were married (80.7%, 57%, and 75%, respectively). Mean (SD) BMI in hemodialysis, peritoneal dialysis and control groups was 23.5 (4.5), 24.7 (2.7), and 25 (2.9) kg/m2, respectively. In the hemodialysis group, 25 samples were below the high school graduate level (51.1%), and 22 were high school graduates and higher (48.8%). In the peritoneal dialysis group, 26 samples were below the high school graduate level (57.8%), and 19 were high school graduates and higher (42.3%). In the control group, 23 samples were below high school graduate level (51.1%), and 22 were high school graduates and higher (48.8%). Twenty one samples (46.7%) in the hemodialysis group reported their family income to be less than their expenses and 22 samples (48.9%) reported it to be the same as their expenses However, in the peritoneal dialysis group, 30 samples (66.7%) reported their family income less than their expenses and 15 samples (33.3%) reported it to be the same as their expenses. Sixteen samples (35.6%) in the control group also reported their family income less than their expenses and 29 samples (64.4%) reported it as the same as their expenses. In the hemodialysis and peritoneal dialysis groups, 32 (71.1%) and 31 (68.8%) samples were unemployed respectively, while 20 samples (44.4%) were unemployed in the control group. The most common cause of end-stage renal disease in both groups was diabetes (27% and 47.7% frequency in hemodialysis and peritoneal dialysis groups, respectively).
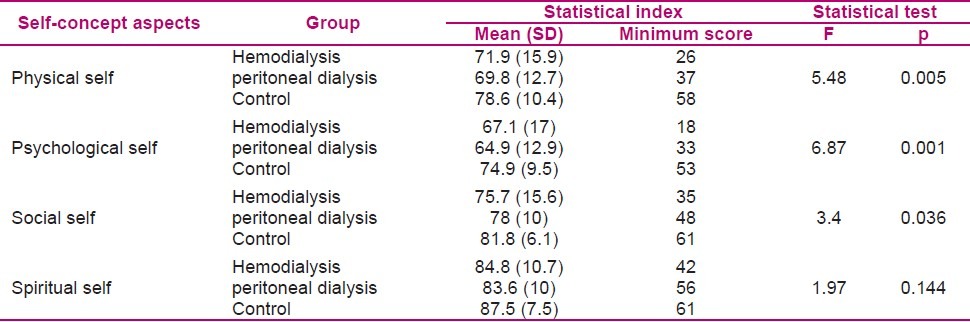
The results of ANOVA test indicated that statistically there was a significant difference between the mean score of self-concept in physical, psychological and social self in the three hemodialysis, peritoneal dialysis and control groups (p < 0.05). However, Duncan’s post hoc test showed that mean score of self-concept in the mentioned aspects had no significant difference in the hemodialysis and peritoneal dialysis groups (p > 0.05). In other words, mean score of self-concept in aspects, mentioned above, in hemodialysis and peritoneal dialysis groups was significantly lower than in the control group. Furthermore, the minimum score of self-concept, in above mentioned aspects, in patients of the peritoneal dialysis group was greater than patients of the hemodialysis group. However, mean score of self-concept statistically had no significant difference between the three groups in terms of spiritual self aspect (p = 0.144) (Table 1).
Table 1.
Comparing the mean score of self-concept in different aspects in the studied subjects of the three groups
DISCUSSION
The results of this study showed that mean score of self-concept in the three physical, psychological and social self aspects was different for the hemodialysis, peritoneal dialysis and control groups. However, statistically they had no significant difference in spiritual self. In other words, mean score of self-concept in physical, psychological and social self aspects for hemodialysis and peritoneal dialysis groups was lower than for the control group. However, mean score of self-concept in each three aspects in the hemodialysis and peritoneal dialysis groups had no significant difference.
In line with the results of the present study, Partridge and Robertson found that disturbance level in body-image for male and female participants undergoing dialysis was significantly higher than that of the healthy population of society[33] In addition, Rezai et al. found that 56% of subjects undergoing hemodialysis had a completely negative mental image of their own appearance and physiological activities, 57.3% had a completely negative mental image of their own daily activities against social and personal stimuli (e.g. daily activities and business tasks), 70.7% had a relatively negative mental image of family and society’s reactions toward themselves, and 20% had a completely negative mental image of their communication and presence in the society.[19] The results obtained from Juergensen et al. also indicated that patients undergoing peritoneal dialysis had more satisfaction with their body-image, social and family life compared to those undergoing hemodialysis. However, it was only in the social and family life that a statistically meaningful difference was observed between the two groups.[25] A 6–12 month follow-up by Koike in the U.S. showed that the depression level in patients with chronic physical illness was significantly greater than others.[34] The findings of Bao et al. also indicated that in the group undergoing hemodialysis, the prevalence of erectile dysfunction was significantly higher and the score of erectile dysfunction was considerably lower in the control group and this issue had overwhelmed these patients mentaly.[35] Kazemi et al. showed that patients undergoing hemodialysis, experience changes in their social interaction with others. They believed that the Iranian culture causes patients to try to hide their illness from others which will lead to social isolation and will subsequently reduce patients’ social interaction with others.[36] Stewart stated that there was a relationship between sexual dysfunction in male patients undergoing hemodialysis with reduction in social interactions, social functioning and role-related limitations.[37] The results of Hojjati et al. showed that patients undergoing hemodialysis who had higher frequency of prayer had higher spiritual health.[38] All the above mentioned studies were in accordance with the results of the present study.
However, Wu et al. found that patients undergoing peritoneal dialysis had higher rates of disorder in special aspects of body-image due to the existence of permanent catheter and dialysate in the peritoneal cavity.[39] Yaziciet al. also reported a depression level of 43.8%, 75.3% and 4.2% in female patients undergoing hemodialysis, peritoneal dialysis and within the control groups, respectively. This problem was particularly inversely correlated to sexual function.[40] Juergensen et al. also showed that patients undergoing hemodialysis had lower satisfaction from religion and spirituality than patients undergoing peritoneal dialysis and there was a significant statistical difference between the two groups.[25] The results of the above study was not in accordance with the present study. It seems using different tools, unjustified number of subjects, research on one gender in the studied groups and ethnic, cultural, social and spiritual differences between the nations were the cause of the inconsistency of these studies with the present study.
Generally, the stressors challenge the individual’s adaptability capacities. Changes in physical, mental, emotional, sexual, familial, and socio-cultural health will influence the self-concept.[41] Therefore, patients undergoing dialysis may suffer from injuries in many aspects of their lives such as losing their job, role reduction, functional and nutritional limitations, change in sexual function, potential damage to independence, social isolation, changes in appearance of body due to the nature of the disease and undergoing dialysis, and consequently changes in self-concept[42] which may result in irreversible consequences.
In addition to the results of the study, perhaps it can be said that patients undergoing dialysis have issues with their self-concept due to stresses and disorders caused by treatment, and are weaker in different aspects of self-concept compared to the control group. Moreover, it seems that the type of dialysis does not cause much difference; therefore, appropriate education and adequate information for patients with end-stage renal disease to use appropriate methods of adaptation[9] as well as appropriate social relationships, continuing social support,[30] and developing health policies seem necessary to prevent mental disorders and provide the required services and supports for patients.
ACKNOWLEDGMENT
We would like to thank all the participating patients, and all the staff of dialysis centers in affiliated hospitals of Isfahan University of Medical Sciences who assisted us in conducting the present study.
Footnotes
This article was derived from MSc thesis in the Isfahan University of Medical Sciences, No: 389265
Source of Support: Isfahan University of Medical Sciences
Conflict of Interest: None declared.
REFERENCES
- 1.Lederer E, Ouseph R. Chronic kidney disease. Am J Kidney Dis. 2007;49(1):162–71. doi: 10.1053/j.ajkd.2006.09.021. [DOI] [PubMed] [Google Scholar]
- 2.Monahan FD, Sands JK, Neighbors M, Marek JF, Green CJ. Phipps’ medical-surgical nursing: health and illness perspectives. 8th ed. Philadelphia: Elsevier Mosby; 2007. p. 1003. [Google Scholar]
- 3.Osborn KS, Wraa CE, Watson AB. Medical-surgical nursing:preparation for practice. California: Pearson; 2009. p. 1780. [Google Scholar]
- 4.Brunner LS, Smeltzer SC, Bare BG, Hinkle J, Cheever KH. Brunner and Suddarth’s textbook of medical-surgical nursing. 12th ed. Philadelphia: Lippincott Williams & Wilkins; 2010. p. 1328.p. 1337.p. 1339.p. 1342. [Google Scholar]
- 5.Borazpardenjani SH, Mohammadi I, Boroumand B. The effect of diet education on laboratory indices and overweight between two sessions of dialysis in patients undergoing maintenance hemodialysis. Journal of Shahrekord University of Medical Sciences. 2006;8(1):20–7. [Google Scholar]
- 6.Brunner LS, Smeltzer SC, Bare BG, Hinkle J, Cheever KH. Brunner and Suddarth’s textbook of medical-surgical nursing. 11th ed. Philadelphia: Lippincott Williams & Wilkins; 2008. p. 1527. [Google Scholar]
- 7.Welch JL, Perkins SM, Johnson CS, Kraus MA. Patterns of interdialytic weight gain during the first year of hemodialysis. Nephrol Nurs J. 2006;33(5):493–9. [PubMed] [Google Scholar]
- 8.Zaman Zadeh V, Heydar Zadeh M, Eshvandi KH, Lakdizeji S. The correlation between quality of life and social support in hemodialysis patients. Medical Journal of Tabriz University of Medical Science & Health Service. 2007;29(1):49–54. [Google Scholar]
- 9.Peron K, Abdollah zadeh F, Ghouha Zadeh M, Ahangar R. The stressors and adaptability methods for patients undergoing peritoneal dialysis. Nursing & Midwifery Journal of Tabriz. 2010;5(17):34–41. [Google Scholar]
- 10.Najafi I. Complications of Hemodialysis. Tehran: Lahzeh publications; 2007. p. 16. [Google Scholar]
- 11.Aref Zadeh AR, Lesan Pezeshki M, Seyfi S, Khatami MR. The cost of hemodialysis in Iran. Iranianp. Journal of Medical Council of Islamic Republic of Iran. 2008;26(1):76–82. [Google Scholar]
- 12.Black JM, Hawks JH. Medical-surgical nursing: clinical management for positive outcomes. 8th ed. Philadelphia: Saunders; 2009. p. 816. [Google Scholar]
- 13.Mahdavi Mazdeh M, Hemmat Abadi M, Ahmadi F, Seyfi S. Comparing acute clinical intra hemodialysis compatibility and biocompatibility of polysulfone versus hemophane membranes. Arak Medical University Journal. 2006;9(4):88–92. [Google Scholar]
- 14.Timby BK, Smith NE. Introductory Medical-Surgical Nursing. 10th ed. Philadelphia: Lippincott Williams & Wilkins; 2009. p. 936. [Google Scholar]
- 15.Urden LD, Stacy KM, Lough ME. Critical Care Nursing, Diagnosis and management. 6th ed. Philadelphia: Mosby Elsevier; 2010. p. 815. [Google Scholar]
- 16.Udaya Kumar TR, Amalraj A, Soundarajan P, Abraham G. Level of stress and coping abilities in patients on chronic hemodialysis and peritoneal dialysis. Indian J Nephrol. 2003;13(3):89–91. [Google Scholar]
- 17.Asti T, Kara M, Ipek G, Erci B. The experiences of loneliness, depression, and social support of Turkish patients with continuous ambulatory peritoneal dialysis and their caregivers. J Clin Nurs. 2006;15(4):490–7. doi: 10.1111/j.1365-2702.2006.01330.x. [DOI] [PubMed] [Google Scholar]
- 18.Rahimi A, Ahmadi F, Ghaliaf M. The effect of continuous care model on self-esteem of hemodialysis patients. Journal Of Zanjan University Of Medical Sciences And Health Services. 2005;13(53):16–21. [Google Scholar]
- 19.Rezai R, Hejazi SH, Shahnazarian J, Mahmoudi M, Seidiandi SJ. Comparing the body-image in patients undergoing hemodialysis with kidney transplant. Payesh. 2009;8(3):279–87. [Google Scholar]
- 20.Yaghmai F, Khalfi A, Khoust N, Alavimajd A. Reviewing the correlation of self-concept with aspects of health status in patients undergoing hemodialysis in selected hospitals affiliated to Shahid Beheshti University of Medical Sciences and Health Services in 2004. Pajoohandeh journal. 2006;10(6):389–94. [Google Scholar]
- 21.De Gas BV. In: Principles of care from De Gas patient. 2nd ed. Atash zadeh F, Barzabadi Z, Khazai N, Anbouhi S, translators; Ezzati J, editor. Tehran: Golban Publications; 2007. pp. 827–33. [Google Scholar]
- 22.Koushan M, Vaghei S. Psychiatric Nursing, Mental Health. Tehran: Andishe Rafi Publications; 2005. p. 54. [Google Scholar]
- 23.Carson VB. Mental Health Nursing: The Nurse-patient journey. 2nd ed. New York: Lightning Source Inc; 2006. p. 168. (169, 170, 171, 172, 173, 174, 177). [Google Scholar]
- 24.Pahlevan Zadeh S, Maghsoudi J. Mental Health. Isfahan: Isfahan University of Medical Sciences Publication; 2005. pp. 103–4. [Google Scholar]
- 25.Juergensen E, Wuerth D, Finkelstein SH, Juergensen PH, Bekui A, Finkelstein FO. Hemodialysis and peritoneal dialysis: patients’ assessment of their satisfaction with therapy and the impact of the therapy on their lives. Clin J Am Soc Nephrol. 2006;1(6):1191–6. doi: 10.2215/CJN.01220406. [DOI] [PubMed] [Google Scholar]
- 26.Thomas N. Renal nursing. 2nd ed. Philadelphia: Elsevier Health Sciences; 2002. p. 191. [Google Scholar]
- 27.Brown EA, Parfrey PS. Complications of long-term dialysis. Oxford: Oxford University Press; 1999. pp. 220–1. [Google Scholar]
- 28.Tahmasebi S, Ghafrani pour F, Ravaghi K, Moghaddasi J, Sadegh Moghaddam L, Kazem Nejad A. Reviewing the efficacy of group discussion on mental image of thalassemic 11 to 18-year-old adolescents. Journal of Shahrekord University of Medical Sciences. 2005;7(4):50–7. [Google Scholar]
- 29.Meira FS, Poli de Figueiredo CE, Figueiredo AE. Influence of sodium profile in preventing complications during hemodialysis. Hemodial Int. 2007;11(Suppl 3):S29–S32. doi: 10.1111/j.1542-4758.2007.00226.x. [DOI] [PubMed] [Google Scholar]
- 30.Sertoz OO, Asci G, Toz F, Duman S, Elbi H, Ok E. Planning a social activity to improve psychological well-being and quality of life of hemodialysis patients: a pilot study. Ther Apher Dial. 2009;13(4):366–72. doi: 10.1111/j.1744-9987.2009.00690.x. [DOI] [PubMed] [Google Scholar]
- 31.Williams AG, Crane PB, Kring D. Fatigue in African American women on hemodialysis. Nephrol Nurs J. 2007;34(6):610–7. 644. [PubMed] [Google Scholar]
- 32.De PC, Pistorio ML, Sorbello M, Parrinello L, Corona D, Gagliano M, et al. Body image in kidney transplantation. Transplant Proc. 2010;42(4):1123–6. doi: 10.1016/j.transproceed.2010.03.071. [DOI] [PubMed] [Google Scholar]
- 33.Partridge KA, Robertson N. Body-image disturbance in adult dialysis patients. Disabil Rehabil. 2011;33(6):504–10. doi: 10.3109/09638288.2010.498556. [DOI] [PubMed] [Google Scholar]
- 34.Koike AK, Unutzer J, Wells KB. Improving the care for depression in patients with comorbid medical illness. Am J Psychiatry. 2002;159(10):1738–45. doi: 10.1176/appi.ajp.159.10.1738. [DOI] [PubMed] [Google Scholar]
- 35.Ban J, Yu Q, Yu H, Hao J, Liu J, Yao J, et al. Erectile dysfunction in male hemodialysis patients in China--one center experience. Clin Nephrol. 2011;75(2):135–40. doi: 10.5414/cn106408. [DOI] [PubMed] [Google Scholar]
- 36.Kazemi M, Nikbakht Nasrabadi A, Hasanpour M, Hassankhani H, Mills J. Experience of Iranian persons receiving hemodialysis: A descriptive, exploratory study. Nursing & Health Sciences. 2011;13(1):88–93. doi: 10.1111/j.1442-2018.2011.00586.x. [DOI] [PubMed] [Google Scholar]
- 37.Stewart M. Narrative literature review: sexual dysfunction in thepatient on hemodialysis. Nephrol Nurs J. 2006;33(6):631–41. [PubMed] [Google Scholar]
- 38.Hojjati H, Ghorbani M, Nazari R, Sharifnia SH, Akhoundzadeh G. The association of praying with spiritual health in patients undergoing hemodialysis. The Journal of Fundamentals of Mental Health. 2010;12(46):514–21. [Google Scholar]
- 39.Wu AW, Fink NE, Marsh-Manzi JV, Meyer KB, Finkelstein FO, Chapman MM, et al. Changes in quality of life during hemodialysis and peritoneal dialysis treatment: generic and disease specific measures. J Am Soc Nephrol. 2004;15(3):743–53. doi: 10.1097/01.asn.0000113315.81448.ca. [DOI] [PubMed] [Google Scholar]
- 40.Yazici R, Altintepe L, Guney I, Yeksan M, Atalay H, Turk S, et al. Female sexual dysfunction in peritoneal dialysis and hemodialysis patients. Ren Fail. 2009;31(5):360–4. doi: 10.1080/08860220902883012. [DOI] [PubMed] [Google Scholar]
- 41.Potter PA, Perry AG. Fundamentals of nursing. Philadelphia: Elsevier Mosbyp; 2009. pp. 414–5. [Google Scholar]
- 42.Muringai T, Noble H, McGowan A, Channey M. Dialysis access and the impact on body image: role of the nephrology nurse. Br J Nurs. 2008;17(6):362–6. doi: 10.12968/bjon.2008.17.6.28900. [DOI] [PubMed] [Google Scholar]