

Abstract
This paper presents an unusual case of gingival ALCL, which mimicked a benign hyperplastic lesion that occurred in a 57-year-old white man representing the first clinical manifestation of acquired immunodeficiency syndrome (AIDS). The patient was referred to the Dental Clinic of PUCPR complaining of a lobulated nodule on the gingiva of his upper central incisors. The presence of advanced chronic periodontitis and dental plaque raised suspicion for a benignancy. An excisional biopsy was performed, and large pleomorphic cells with an abundant cytoplasm, sometimes containing prominent nucleoli and “Hallmark” cells, were observed through hematoxylin and eosin staining. The tumor cells showed strong CD30 expression, EMA, Ki-67, and LCA, and negative stain for p80NPM/ALK, CKAE1/AE3, CD20, CD3, CD56, and CD15. The final diagnosis was ALCL (ALK-negative). Further laboratory tests revealed positivity for human immunodeficiency virus (HIV). The patient was submitted to chemotherapy, but four months after diagnosis, the patient died due to pneumonia and respiratory failure. Oral anaplastic large-cell lymphoma (ALCL) is a rare disorder. Only 5 cases involving the gingiva have been reported, and to our knowledge, this is the first case reported of the ALCL, which mimicked a hyperplastic benignancy as the first clinical manifestation of AIDS.
1. Introduction
Malignant lymphomas (MLs) are a large group of neoplasms affecting the lymphoid system and are subdivided into two main groups: Hodgkin's and non-Hodgkin's lymphomas (NHLs) [1]. ML is considered an opportunistic neoplasm because it frequently affects immunocompromised patients. The prevalence of ML has increased considerably with improved acquired immune deficiency syndrome (AIDS) survivorship [2, 3]. NHLs appear in 3% of HIV-seropositive patients [4]. The NHLs may be present outside the lymphoid system, in which case they are called extranodal [5]. This type of lymphoma is located at an extranodal site in 40% of cases [5] and its extranodal presentation occurs in almost 75% of human-immunodeficiency-virus- (HIV-) seropositive patients [2]. Furthermore, only 2% to 3% of these extranodal cases occur in the oral cavity [6].
In the group of NHLs, mature T cell and natural killer (NK) cell neoplasms make up only 12% of NHL cases worldwide [1]. Within this heterogeneous category, anaplastic large-cell lymphoma (ALCL) is found [7, 8] and is listed in the Revised European-American Classification of Lymphoid Neoplasms (REAL) as an independent entity [9]. A couple of ALCL cases have been reported, although some were the B-cell phenotype now classified as an anaplastic type of diffuse large B-cell lymphoma [10]; therefore, these cases were excluded from the present review. ALCL is characterized by proliferation of the anaplastic large lymphoid cells with abundant cytoplasm and strong expression of CD30 antigen; however, its final diagnosis is a challenge for oral pathologists [8, 11–17]. Two distinct clinical entities of ALCL are recognized by the World Health Organization (WHO) lymphoma classification: cutaneous and systemic lymphomas [1, 5]. The cutaneous ALCLs are characterized by indolent growth and may show spontaneous remission and good prognosis [18, 19]. The systemic ALCLs can be ALK-positive or -negative [18]. The ALK-positive ALCLs usually occur in male pediatric patients and show a good prognosis taking into account their affective response to chemotherapy, whereas the ALK-negative ALCLs occur in elderly patients and present a poor prognosis [18, 20].
ALCL especially affects the skin of the body [6]. This T-type lymphoma in the oral cavity is an extremely rare disorder characterizing 1% of lymphomas overall [19]. From the scientific literature, we found around 15 cases of ALCL in the oral cavity [2, 6, 8, 11–17, 21, 22]. Only 5 cases of ALCL located in gingiva have been reported in the literature [12, 17, 22], and our case is the fourth reported occurrence of ALCL in the oral cavity of a HIV-seropositive patient [2, 11]. Besides, this paper is the first to present an unusual case of oral ALK-negative ALCL that mimicked a benign hyperplastic lesion as a first clinical manifestation of AIDS.
2. Case Report
A 57-year-old white man was referred to the Dental Clinic of PUCPR complaining of an asymptomatic hyperplastic lesion on the gingiva of his upper central incisors, which had grown significantly in the last two months. The patient was a nonsmoker and his medical history did not reveal other relevant information. The extraoral examination showed a small swelling of the upper lip and absence of cervical lymphadenopathy. The intraoral examination showed advanced chronic periodontitis and the presence of a lobulated reddish nodule, pedunculated, measuring around 2.5 cm on the gingival area between both upper central incisors which had mobility and accumulation of dental plaque (Figure 1). The lesion did not have an ulcerated surface, and palpation revealed a soft consistency with bleeding on the surface. Panoramic radiography showed a significant resorption of bone mainly in the anterior area of the maxillary, compatible with advanced chronic periodontitis (Figure 2).
Figure 1.

Clinical presentation: a 2,5 cm red nodule, pedunculated, located on the gingival between upper central incisors.
Figure 2.

Radiographic image: panoramic radiography showing the extensive bone resorption in the anterior area of the maxilla compatible with advanced periodontal disease.
Taking into account that the first impression of the lesion revealed clinical characteristics of a benignancy, as the pedunculated nodule, circumscribed, freely moveable, the presence of dental plaque, and advanced chronic periodontitis, we initially suspected that it could be related to a reactive hyperplastic lesion. These lesions include pyogenic granuloma, focal fibrous hyperplasia, peripheral giant cell granuloma, and peripheral ossifying fibroma. Therefore, considering these main hypotheses, an excisional biopsy of the nodule was performed under local anesthesia. Furthermore, the patient was referred for periodontal treatment.
Hematoxylin and eosin-stained sections showed a lesion characterized by a diffuse proliferation of lymphoid tumor cells underneath an epithelium (Figure 3(a)). The slices also showed large pleomorphic cells with an abundant cytoplasm, sometimes containing prominent nucleoli. “Hallmark” cells with eccentric, horse-shoe, or kidney-shaped nuclei were also observed (Figure 3(b)). The tumor cells frequently demonstrated mitotic figures. Immunohistochemical analysis using a streptavidin-biotin protocol [14] was performed with the antibodies: CKAE1/AE3, CD20, CD3, CD30, Ki-67, epithelial membrane antigen (EMA), CD56, leukocyte common antigen (LCA), p80NPM/ALK, and CD15. The tumor cells showed strong CD30 expression with a membrane and Golgi distribution in the majority of tumor cells (Figure 3(c)). Ki-67 positive stain was observed in 90% of tumor cells (Figure 3(d)). Positive stain in tumor cells was also identified for EMA and LCA. Negative stain was identified for p80NPM/ALK, CKAE1/AE3, CD56, and CD15. The tumor was a null-cell type (negatively stained for CD20 and CD3). Based on clinical, histological, and immunohistochemical findings, the final diagnosis was extranodal ALK-negative ALCL.
Figure 3.
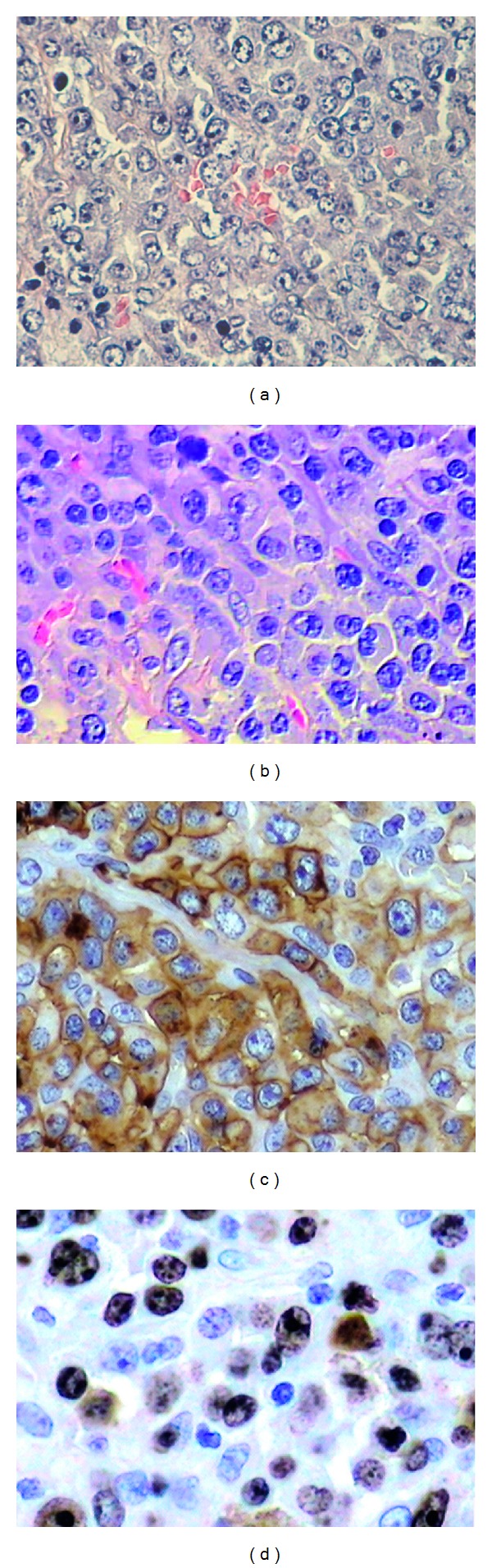
Histologic features: (a) diffuse proliferation of lymphoid tumor cells (hematoxylin-eosin stain (HE), magnification ×200) was observed. (b) Large pleomorphic cells with an abundant cytoplasm, sometimes containing prominent nucleoli, were verified. “Hallmark” cells with eccentric, horse-shoe, or kidney-shaped nuclei were also identified (HE, magnification ×400). Immunohistochemical findings: sections showing tumor cells are positive for (c) CD30 with a membrane and Golgi distribution (streptavidin-biotin, ×400 magnification) and (d) Ki-67 (streptavidin-biotin, ×400 magnification).
The patient was referred to a specialized oncology hospital where further laboratory and imaging tests showed positivity for HIV, negativity for both hepatitis B and C, normal full blood count proportions of white and red blood cells and platelets, and absence of lymphadenopathies and metastasis. The following chemotherapy protocol consisted of six cycles of CHOP (cyclophosphamide 750 mg/m2, doxorubicin 50 mg/m2, vincristine 2 mg, and oral prednisone 100 mg) for five days [23]. However, four months after diagnosis, the patient died due to pneumonia and respiratory failure.
3. Discussion
This case report presents a rare case of ALCL in an extranodal site of a Brazilian male HIV-seropositive patient. Since ALCL was first described as a clinical entity by Stein et al. (1985) [20], this lesion was classified as Ki-1+ ALCL and currently as Ki-1 (CD30) [17], which corresponds to a cohesive proliferation of large pleomorphic cells that express CD30. The ALCL is subdivided according to the immunohistochemical features in precursor T cells or null cells, in 60% and 25% of the cases, respectively [2]. Therefore, immunohistochemistry is imperative for the correct diagnosis of ALCL considering that the cells are positive for CD30 antigen and several other markers such as EMA that is present in slightly more than 50% of cases [2]. LCA is usually positive but may be used negative in 30% to 40% of cases [2]. In most cases, other markers such as Ki-67, CD3, and CD45RO (T-cell phenotype), TIA-1 (T-cell intracytoplasmic antigen-1), perforin, granzyme B, and p80NPM/ALK will be positive [6, 17].
The clinicopathologic features of ALK-carrying ALCLs were first investigated by Shiota and Mori [24]. The authors found that ALK-positive is a distinctive entity clinically and pathogenetically and should be differentiated from ALK-negative. Indeed, based on the most recent findings, the WHO classification currently considers two ALCL types, negative and ALK-positive [25, 26]. The tumors that show a positive reaction for ALK have greater cell proliferation and can show a relatively better prognosis [19]. Recently, studies have proposed that proteins such as aberrant fusion protein (NPM-ALK), JAK-STAT, and PI3K/STAT may be a potential target in ALK-positive lymphomas [26–28]. The findings about specific antigens also suggest that ALK represents an ideal tumor antigen for vaccination-based therapies of ALCL and other ALK-positive tumors [29]. On the other hand, the cases of ALK-negative ALCL show an inaccurate behavior with a relatively unfavorable prognosis [18]. To make the diagnosis of ALK-negative ALCL, there must be a large cell predominant population with abundant cytoplasm and pleomorphic, embryo or hallmark nuclei or wreath-like giant cells, and strong CD30 expression with a membrane and Golgi distribution in virtually every cell with a highly anaplastic T-cell phenotype [17, 19]. As the current case did not express ALK, it was classified as an ALK-negative ALCL. In addition, the tumor did not show expression of NK or T-cell markers; therefore, it was classified as a null cell lymphoma. ALK-negative ALCL normally occurs in adults (40–65 years) with a modest male prevalence [3], as seen in our patient, a 57-year-old man.
Based on cases found in the review of the literature (Table 1), there is a slight male prediction (female : male, 1 : 1.5), and the patients presented at a mean age of 53.4 years old (standard deviation, 22.4). Most of the tumors were located in the gingiva (5 cases), followed by the palate (3 cases), tongue (2 cases), retromolar trigone (2 cases), lip (2 cases), floor of the mouth (1 case), and buccal mucosa (1 case). The main radiographic findings were bone resorption [11, 12, 17], and the main diagnostic hypothesis more frequent is nonspecific infection (4 cases) [2, 13, 16]. To the best of our knowledge, the present case reports the first gingival ALCL, which mimicked a benign hyperplastic lesion as the first clinical manifestation of AIDS. Positivity to HIV was reported in 3 cases [2, 11]. About 14% of the ALCL cases were ALK-negative [17]; our case is the fourth case reported [17, 22]. This highlights that studies about ALK protein were developed in the 1990s. Only in 2002 [16], p80NPM/ALK was first included in the immunohistochemical studies involving oral ALCLs. Currently, there is only one case reported that showed ALK expression in ALCL involving oral cavity [16].
Table 1.
Clinical, radiological, and ALK-profile features of oral anaplastic large-cell lymphomas.
| Age | Gender | Oral area | Clinical findings | Radiographic findings | HIV | Diagnostic hypothesis | ALK | References |
|---|---|---|---|---|---|---|---|---|
| ND | ND | ND | ND | ND | ND | ND | ND | Takahashi et al. [8] |
| 36 | M | Retromolar trigone | Mass with ulcerated surface | Diffuse radiolucency with poorly margins | + | Nonspecific infection | ND | Hicks et al. [2] |
| 42 | M | Retromolar trigone | Enlargement surrounding a crateriform ulcer | Not relevant | + | Pericoronitis or nonspecific infection | ND | Hicks et al. [2] |
| 12 | F | Gingiva | Scaly, swollen, and bleeding gingival surface | Bone resorption causing teeth displacement | + | Gingivitis | ND | Willard et al. [11] |
| 12 | M | Hard palate | Mass involving the nasal cartilage and floor of the orbit | ND | ND | ND | ND | Papadimitriou et al. [21] |
| 75 | F | Upper gingiva | Periodontitis (deep pockets) and redness of the gingiva | Bone resorption adjacent to teeth 11, 12, and 13 | ND | Periodontitis | ND | Rosenberg et al. [12] |
| 61 | M | Lower gingiva | Well-delimited ulceration | ND | ND | Eosinophilic granuloma | ND | Rosenberg et al. [12] |
| 48 | M | Upper lip | Nonfluctuant, firm, and swelling lesion | ND | ND | Nonspecific infection | ND | Chandu et al. [13] |
| 76 | F | Upper lip | Well-delimited ulceration | ND | ND | ND | ND | Chim et al. [14] |
| 65 | F | Hard palate, buccal mucosa, and floor of the mouth | Well-delimited ulceration | ND | − | ALCL | ND | Born et al. [15] |
| 77 | M | Left side of soft palate | Mass with ulcerated surface | ND | − | Lymphoma, salivary gland neoplasm, or necrotizing sialometaplasia | ND | Savarrio et al. [6] |
| 77 | M | Tongue | Nodule with ulcerated surface | A low density mass | ND | Nonspecific infection | + | Notani et al. [16] |
| 76 | F | Upper and lower gingiva | Swollen gingival | Bone resorption | ND | Chronic marginal periodontitis | − | Matsumoto et al. [17] |
| 34 | F | Upper gingiva | White/gray ulcerated mass with erythematous border | ND | ND | Lymphomatoid papulosis, fungal infection, or traumatic ulcer | − | Grandhi et al. [22] |
| 53 | M | Tongue | Mass with ulcerated surface | ND | ND | ND | − | Grandhi et al. [22] |
| 57 | M | Gingiva in maxillary incisor area | A lobulated reddish nodule, bleedin,g and pedunculated | Bone resorption | + | Reactive hyperplasic lesiona | − | Present case |
ND: not described, F: female; M: male; +: positive; −: negative; aincludes pyogenic granuloma, focal fibrous hyperplasia, peripheral giant cell granuloma, and peripheral ossifying fibroma.
Interestingly, cases of ALCL present in the gingiva also suggested that the majority of clinical aspects mimicked gingivitis or advanced chronic periodontitis with ulcers, bleeding, and swelling. All clinical aspects of ALCLs in oral cavity were associated with extensive bone resorption, which made the clinical diagnosis of ALCL more difficult. Clinical cases have reported other entities of oral lymphomas that mimicked a benignancy in HIV-seropositive patients [30]. We found only 15 cases of oral ALCL reported in the English literature (Table 1). The current case showed an unusual appearance of a reactive hyperplastic lesion associated with advanced chronic periodontitis. Indeed, this fact emphasizes the need for a thorough clinical history, HIV investigation, and also high index suspicion in both dentists and pathologists.
Oral lymphomas also occur more frequently in patients with HIV infection [31] as well as those iatrogenically immunosuppressed [31, 32]. Mechanisms other than the loss of immune surveillance appear to be involved with HIV-associated malignances [11]. In our case, the oral lymphoma with distinctive clinical appearance and associated with periodontitis occurred in an HIV-seropositive patient and was the first manifestation of AIDS. Some studies have also suggested that HIV is a risk factor for the development of ALCL, but this hypothesis is not clear yet. Similarly, the relative risk for the development of an NHL in HIV patients is approximately 3%, making the prognosis worse [2, 4]. A few cases of oral ALCL in patients with HIV infection have been reported in the literature [2, 11]. It is important to point out that ALCL prognosis is usually associated with immune status, and the death of the patient in this case due to the presence of pneumonia and respiratory failure was directly related to his poor immune systemic condition [20].
ALCL is normally treated by intensive chemotherapy with CHOP (cyclophosphamide 750 mg/m2, doxorubicin 50 mg/m2, vincristine 2 mg, and oral prednisone 100 mg from the first to the fifth day of chemotherapy) [23]. This CHOP regimen was administered every 3 weeks for a total of six cycles. Several studies demonstrate the high rate of complete remission (70%–95%) and 70%–85% long-term overall survival [23]. However, unfortunately, in the current case, the patient died.
4. Summary
In our case, it is important to highlight that the rapid growth of the lesion in the last two months reported by the patient and the presence of dental plaque and advanced chronic periodontitis indicated a reactive process in the gingiva. For this reason, the first decision to make an excisional biopsy of the lesion was kept. It is also important to stress that, if it was known that the patient was HIV-positive, our conduct would be completely different. Unfortunately, the final diagnosis was a malignant lesion.
We presented an unusual case of ALK-negative ALCL on the gingiva associated with advanced chronic periodontitis that mimicked some clinical features of a hyperplastic gingival benignancy, which manifested in a 57-year-old HIV-seropositive man. ALCL is a systemic malignant disease characterized by the extranodal type which rarely occurs in the oral cavity as the first manifestation of acquired immunodeficiency syndrome. Thus, we emphasize the importance of an accurate clinical, including HIV investigation, histological, and immunohistochemical analysis of oral lesions to establish the correct diagnosis of those lesions which in daily practice are considered benign.
Disclosure
The authors declare no conflict of interests concerning this paper. The authors have full control of all primary data of their paper. This paper is not supported by any institutional or corporate affiliation.
Acknowledgments
The authors thank Ana Paula Camargo Martins and Marina Viola Azevedo for their most valuable laboratory technical assistance.
References
- 1.Rosenerg SA, Berand CW, Brown BW., Jr. National Cancer Institute sponsored study of classifications of non-Hodgkin’s lymphomas. Summary and description of a working formulation for clinical usage. Cancer. 1982;49(10):2112–2135. doi: 10.1002/1097-0142(19820515)49:10<2112::aid-cncr2820491024>3.0.co;2-2. [DOI] [PubMed] [Google Scholar]
- 2.Hicks MJ, Flaitz CM, Nichols CM, Luna MA, Gresik MV. Intraoral presentation of anaplastic large-cell Ki-1 lymphoma in association with HIV infection. Oral Surgery Oral Medicine and Oral Pathology. 1993;76(1):73–81. doi: 10.1016/0030-4220(93)90298-i. [DOI] [PubMed] [Google Scholar]
- 3.Jaffe ES, Harris NL, Stein H, Vardiman JV. Pathology and Genetics of Tumours of Haematopoietic and Lymphoid Tissues. Lyon, France: IARC; 2001. World Health Organization: classification of tumors. Pathology and genetics: tumours of haematopoietic and lymphoid tissues; pp. 119–205. [Google Scholar]
- 4.Beral V, Peterman T, Berkelman R, Jaffe H. AIDS-associated non-Hodgkin lymphoma. The Lancet. 1991;337(8745):805–809. doi: 10.1016/0140-6736(91)92513-2. [DOI] [PubMed] [Google Scholar]
- 5.Kemp S, Gallagher G, Kabani S, Noonan V, O’Hara C. Oral non-Hodgkin’s lymphoma: review of the literature and World Health Organization classification with reference to 40 cases. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontology. 2008;105(2):194–201. doi: 10.1016/j.tripleo.2007.02.019. [DOI] [PubMed] [Google Scholar]
- 6.Savarrio L, Gibson J, Dunlop DJ, O’Rourke N, Fitzsimons EJ. Spontaneous regression of an anaplastic large cell lymphoma in the oral cavity: first reported case and review of the literature. Oral Oncology. 1999;35(6):609–613. doi: 10.1016/s1368-8375(99)00034-2. [DOI] [PubMed] [Google Scholar]
- 7.Merkel O, Kenner L, Turner SD. Anaplastic large cell lymphoma: the current state of play from a European prospective as presented at the second annual meeting of the European Research Initiative on ALCL, 27-28 June 2011. Leukemia. 2011;25(12):1795–1796. doi: 10.1038/leu.2011.295. [DOI] [PubMed] [Google Scholar]
- 8.Takahashi H, Fujita S, Okabe H, Tsuda N, Tezuka F. Immunophenotypic analysis of extranodal Non-Hodgkin’s lymphomas in the oral cavity. Pathology Research and Practice. 1993;189(3):300–311. doi: 10.1016/S0344-0338(11)80514-5. [DOI] [PubMed] [Google Scholar]
- 9.Harris NL, Jaffe ES, Stein H, et al. A revised European-American classification of lymphoid neoplasms: a proposal from the International Lymphoma Study Group. Blood. 1994;84(5):1361–1392. [PubMed] [Google Scholar]
- 10.Piris M, Brown DC, Gatter KC, Mason DY. CD30 expression in non-Hodgkin’s lymphoma. Histopathology. 1990;17(3):211–218. doi: 10.1111/j.1365-2559.1990.tb00709.x. [DOI] [PubMed] [Google Scholar]
- 11.Willard CC, Foss RD, Hobbs TJ, Auclair PL. Primary anaplastic large cell (KI-1 positive) lymphoma of the mandible as the initial manifestation of acquired immunodeficiency syndrome in a pediatric patient. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and. 1995;80(1):67–70. doi: 10.1016/s1079-2104(95)80018-2. [DOI] [PubMed] [Google Scholar]
- 12.Rosenberg A, Biesma DH, Sie-Go DMDS, Slootweg PJ. Primary extranodal CD30-positive T-cell non-Hodgkin’s lymphoma of the oral mucosa: report of two cases. International Journal of Oral and Maxillofacial Surgery. 1996;25(1):57–59. doi: 10.1016/s0901-5027(96)80013-0. [DOI] [PubMed] [Google Scholar]
- 13.Chandu A, Mitchell DA, Corrigan AM. Cutaneous CD30 positive large T cell lymphoma of the upper lip: a rare presentation. British Journal of Oral and Maxillofacial Surgery. 1997;35(3):193–195. doi: 10.1016/s0266-4356(97)90563-5. [DOI] [PubMed] [Google Scholar]
- 14.Chim CS, Chan ACL, Raymond L. Primary CD30-positive anaplastic large cell lymphoma of the lip. Oral Oncology. 1998;34(4):313–315. doi: 10.1016/s1368-8375(98)80014-6. [DOI] [PubMed] [Google Scholar]
- 15.Born S, Gaber G, Willgeroth K, Wagner U, Haneke E, Marsch WC. Metastasising malignant lymphoma mimicking necrotising and hyperplastic gingivostomatitis. European Journal of Dermatology. 1999;9(7):569–573. [PubMed] [Google Scholar]
- 16.Notani K, Shindoh M, Takami T, Yamazaki Y, Kohgo T, Fukuda H. Anaplastic large cell lymphoma (ALCL) in the oral mucosa with repeating recurrence and spontaneous regression of ulceration: report of a case. Oral Medicine & Pathology. 2002;7(2):79–82. [Google Scholar]
- 17.Matsumoto N, Ohki H, Mukae S, et al. Anaplastic large cell lymphoma in gingiva: case report and literature review. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontology. 2008;106(4):e29–e34. doi: 10.1016/j.tripleo.2008.05.037. [DOI] [PubMed] [Google Scholar]
- 18.ten Berge RL, Oudejans JJ, Ossenkoppele GJ, Meijer CJLM. ALK-negative systemic anaplastic large cell lymphoma: differential diagnostic and prognostic aspects—a review. Journal of Pathology. 2003;200(1):4–15. doi: 10.1002/path.1331. [DOI] [PubMed] [Google Scholar]
- 19.Campo E, Chott A, Kinney MC, et al. Update on extranodal lymphomas. Conclusions of the Workshop held by the EAHP and the SH in Thessaloniki, Greece. Histopathology. 2006;48(5):481–504. doi: 10.1111/j.1365-2559.2006.02369.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Stein H, Mason DY, Gerdes J. The expression of the Hodgkin’s disease associated antigen Ki-1 in reactive and neoplastic lymphoid tissue: evidence that Reed-Sternberg cells and histiocytic malignancies are derived from activated lymphoid cells. Blood. 1985;66(4):848–858. [PubMed] [Google Scholar]
- 21.Papadimitriou JC, Abruzzo LV, Bourquin PM, Drachenberg CB. Correlation of light microscopic, immunocytochemical and ultrastructural cytomorphology of anaplastic large cell Ki-1 lymphoma, an activated lymphocyte phenotype: a case report. Acta Cytologica. 1996;40(6):1283–1288. doi: 10.1159/000334022. [DOI] [PubMed] [Google Scholar]
- 22.Grandhi A, Boros AL, Berardo N, Reich RF, Freedman PD. Two cases of CD30+, anaplastic lymphoma kinase (ALK)-negative anaplastic large cell lymphoma with oral manifestations. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology. 2013;115(2):e41–e47. doi: 10.1016/j.oooo.2012.04.010. [DOI] [PubMed] [Google Scholar]
- 23.Porcu P, Nichols CR. Evaluation and management of the “new” lymphoma entities: mantle cell lymphoma, lymphoma of mucosa-associated lymphoid tissue, anaplastic large-cell lymphoma, and primary mediastinal B-cell lymphoma. Current Problems in Cancer. 1998;22(5):283–368. doi: 10.1016/s0147-0272(98)90003-4. [DOI] [PubMed] [Google Scholar]
- 24.Shiota M, Mori S. Anaplastic large cell lymphomas expressing the novel chimeric protein p80npm/alk: a distinct clinicopathologic entity. Leukemia. 1997;11(supplement 3):538–540. [PubMed] [Google Scholar]
- 25.Inghirami G, Pileri SA. Anaplastic large-cell lymphoma. Seminars in Diagnostic Pathology. 2011;28(3):190–201. doi: 10.1053/j.semdp.2011.03.002. [DOI] [PubMed] [Google Scholar]
- 26.Piccaluga PP, Gazzola A, Mannu C, et al. Pathobiology of anaplastic large cell lymphoma. Advances in Hematology. 2010;2010:10 pages. doi: 10.1155/2010/345053.345053 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Amin HM, McDonnell TJ, Ma Y, et al. Selective inhibition of STAT3 induces apoptosis and G1 cell cycle arrest in ALK-positive anaplastic large cell lymphoma. Oncogene. 2004;23(32):5426–5434. doi: 10.1038/sj.onc.1207703. [DOI] [PubMed] [Google Scholar]
- 28.Amin HM, Medeiros LJ, Ma Y, et al. Inhibition of JAK3 induces apoptosis and decreases anaplastic lymphoma kinase activity in anaplastic large cell lymphoma. Oncogene. 2003;22(35):5399–5407. doi: 10.1038/sj.onc.1206849. [DOI] [PubMed] [Google Scholar]
- 29.Chiarle R, Martinengo C, Mastini C, et al. The anaplastic lymphoma kinase is an effective oncoantigen for lymphoma vaccination. Nature Medicine. 2008;14(6):676–680. doi: 10.1038/nm1769. [DOI] [PubMed] [Google Scholar]
- 30.Bagul N, Mamatha GS, Mahalle A. Plasmablastic lymphoma of gingiva mimicking a reactive lesion: a case report. Case Reports in Dentistry. 2012;2012:4 pages. doi: 10.1155/2012/259307.259307 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Zapater E, Bagán JV, Carbonell F, Basterra J. Malignant lymphoma of the head and neck. Oral Diseases. 2010;16(2):119–128. doi: 10.1111/j.1601-0825.2009.01586.x. [DOI] [PubMed] [Google Scholar]
- 32.Safai B, Diaz B, Schwartz J. Malignant neoplasms associated with human immunodeficiency virus infection. Ca-A Cancer Journal for Clinicians. 1992;42(2):74–95. doi: 10.3322/canjclin.42.2.74. [DOI] [PubMed] [Google Scholar]