

Abstract
Diabetic muscle infarction (DMI) is an unusual complication of diabetes mellitus. It is usually seen in long-standing diabetes mellitus. This article presents a case of DMI in the left forearm of a 58-year-old woman. She had a swollen forearm. The level of creatine kinase was 5930 U/L. Her condition was initially suspected for either cellulitis or venous thrombosis. A magnetic resonance imaging (MRI) study of the forearm showed diffuse edema and abnormal signals of the left forearm. The diagnosis of DMI was made. She was treated conservatively and her symptoms resolved within a short period of time. DMI should be considered as a differential diagnosis of any painful and swollen limb in diabetic patients.
Keywords: Diabetes mellitus, infarction, muscle
INTRODUCTION
Musculoskeletal manifestations of diabetes mellitus (DM) are well-recognized complications. Diabetic muscle infarction (DMI), which was described for the first time by Angervall and Stener in 1965,[1] is a rare complication of DM. It is usually seen in long-standing DM along with complications, such as, nephropathy, retinopathy and neuropathy.[2] Until now, less than 200 cases with DMI are reported in the literature.[3] It commonly occurs in the thigh muscles and we have been able to find only five patients with upper extremity involvement.[4–6] In this article, we describe a patient with poorly controlled DM and muscle infarction of her forearm.
CASE REPORT
A 58 year-old-woman with a three-week history of left upper forearm pain was admitted to our hospital. She noted a history of type II DM, which was diagnosed five months ago. She did not have any history of retinopathy, nephropathy, or neuropathy. Her current condition began with a sudden onset of swelling and pain in the left forearm, extending to her fingers. Before this recent admission, several antibiotics and non-steroidal anti-inflammatory drugs were prescribed for her, with no improvement. On physical examination, she was afebrile with severe swelling and tenderness in her forearm. Ophthalmological examination was normal and no evidence of retinopathy or nephropathy was found. The white blood cell count was 17500 (normal, 4800–10800) with 80% neutrophils (normal, 33–75%). Fasting blood glucose was 235 mg/dl (normal, 70–105) and hemoglobin A1C was 6.5% (normal, < 6%). Other laboratory results were as follows: Erythrocyte sedimentation rate (ESR) 17 mm/hour (normal, 0–25), creatine kinase (CK) 5930 U/L (normal, 25–175), lactate dehydrogenase (LDH) 780 U/L (normal, 0–480), aspartate transaminase 89 U/L (normal, < 31), and alanine transaminase 53 U/L (normal, < 31). Blood cultures were negative. Arterial and venous Doppler ultrasound of the left forearm was normal.
Magnetic resonance imaging (MRI) showed diffuse edema and abnormal low and high signal intensities in the soft tissues of the left forearm [Figure 1]. A diagnosis of DMI was made. The blood glucose was controlled by oral hypoglycemic agents. Her muscle enzymes were gradually decreased to 143 and 504 for creatine kinase (CK) and Lactate dehydrogenase (LDH), respectively. She was discharged without any swelling or pain eight days later. On a follow-up visit after two months, she did not have any complaint in her forearm. After three months, post-treatment MRI was performed that showed no abnormal signal intensity in the soft tissues, or bony structures [Figure 2].
Figure 1.
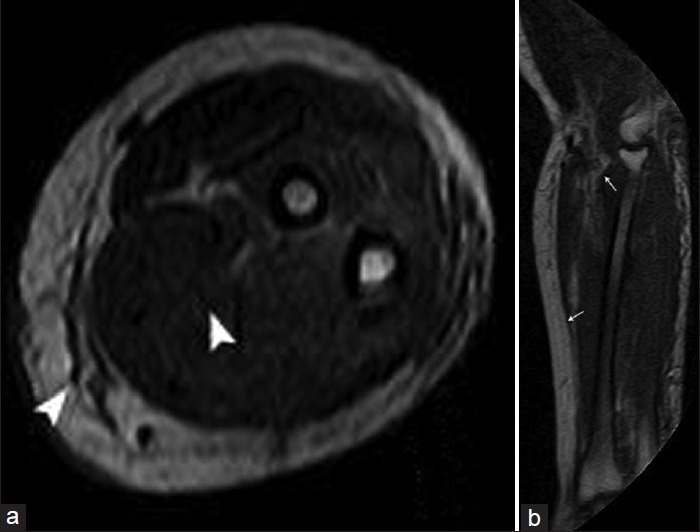
(a) Axial T1-weighted magnetic resonance image of the left forearm. It shows diffuse edema and low signal intensities in the left forearm muscles, with subcutaneous soft tissue swelling (arrowheads). (b) A Sagital T2-weighted magnetic resonance image shows diffuse edema and high signal intensities in the forearm muscles, with subcutaneous soft tissue swelling (arrow)
Figure 2.

(a) Axial T1-weighted and (b) coronal T2-weighted magnetic resonance images after three months show no abnormalities
DISCUSSION
Muscle involvement in the DM is most often related to neuropathy.[7] DMI is the only notable myopathy in DM. Its exact cause is unknown, but several hypotheses have been described, including, arteriosclerosis and microangiopathy, hypoperfusion-induced anoxia, abnormalities of the coagulation system, association with antiphospholipid antibodies, and hypoxia-reperfusion injury.[8] Most patients are young and females, with a mean age of 42 years.[9] Unlike our patient, they usually have long-standing type I DM.[10] The presentation of DMI ispain and swelling that mostly involves the thigh muscles, and rarely, like in our patient, involves the upper extremity.[11] Fever was reported in 10% of the patients.[9] ESR and CK may increase.[11] The best diagnostic tool is the MRI, which shows high and low (or normal) signal intensity on T2- and T1-weighted images, respectively.[12] Although the diagnosis of DMI can be confirmed by muscle biopsy, and it was done in a majority of the cases in the past, due to nonspecific findings and increased risk of recurrence, it is better for it to be reserved for atypical cases.[13] The differential diagnosis of DMI is broad and the most common ones are thrombophlebitis, soft tissue infection, and diabetic amyotrophy.[9,14] Our patient was afebrile, her blood cultures were negative, and we did not find any evidence of muscle or soft tissue infection. No evidence of thrombophlebitis was found either. The best method for DMI management is the conservative method, with blood glucose control.[11,15] She responded well to the rest, with blood glucose control, and without any recurrence in the follow-up visits.
Diabetic muscle infarction should be noted in the differential diagnosis of any diabetic patient presenting with a swollen and painful limb.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Angervall L, Stener B. Tumoriform focal muscular degeneration in two diabetic patients. Diabetologia. 1965;1:39–42. [Google Scholar]
- 2.Glauser SR, Glauser J, Hatem SF. Diabetic muscle infarction: A rare complication of advanced diabetes mellitus. Emerg Radiol. 2008;15:61–5. doi: 10.1007/s10140-007-0629-6. [DOI] [PubMed] [Google Scholar]
- 3.Iyer SN, Drake AJ, 3rd, West RL, Tanenberg RJ. Diabetic muscle infarction: A rare complication of long-standing and poorly controlled diabetes mellitus. Case Report Med. 2011;2011:407921. doi: 10.1155/2011/407921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Joshi R, Reen B, Sheehan H. Upper extremity diabetic muscle infarction in three patients with end-stage renal disease: A case series and review. J Clin Rheumatol. 2009;15:81–4. doi: 10.1097/RHU.0b013e31819b9610. [DOI] [PubMed] [Google Scholar]
- 5.Cardillo S, Huse JT, Iqbal N. Diabetic muscle infarction of the forearm in a patient with long-standing type 1 diabetes. Endocr Pract. 2006;12:188–92. doi: 10.4158/EP.12.2.188. [DOI] [PubMed] [Google Scholar]
- 6.Eady JL, Cobbs KF. Diabetic muscle infarction. J South Orthop Assoc. 1997;6:250–5. [PubMed] [Google Scholar]
- 7.Sander HW, Chokroverty S. Diabetic amyotrophy: Current concepts. Semin Neurol. 1996;16:173–8. doi: 10.1055/s-2008-1040973. [DOI] [PubMed] [Google Scholar]
- 8.Kapur S, Brunet JA, McKendry RJ. Diabetic muscle infarction: Case report and review. J Rheumatol. 2004;31:190–4. [PubMed] [Google Scholar]
- 9.Trujillo-Santos AJ. Diabetic muscle infarction: An underdiagnosed complication of long-standing diabetes. Diabetes Care. 2003;26:211–5. doi: 10.2337/diacare.26.1.211. [DOI] [PubMed] [Google Scholar]
- 10.Lim YW, Thamboo TP. Diabetic muscle infarction of the peroneus brevis: A case report. J Orthop Surg (Hong Kong) 2005;13:314–6. doi: 10.1177/230949900501300319. [DOI] [PubMed] [Google Scholar]
- 11.Ahmed HN, Chhaya SK, Makdissi A, Zimmerman RS. Diabetic muscle infarction: Case report of a rare complication. Am J Med. 2007;120:e3–5. doi: 10.1016/j.amjmed.2006.09.017. [DOI] [PubMed] [Google Scholar]
- 12.Khoury NJ, el-Khoury GY, Kathol MH. MRI diagnosis of diabetic muscle infarction: Report of two cases. Skeletal Radiol. 1997;26:122–7. doi: 10.1007/s002560050205. [DOI] [PubMed] [Google Scholar]
- 13.Chester CS, Banker BQ. Focal infarction of muscle in diabetics. Diabetes Care. 1986;9:623–30. doi: 10.2337/diacare.9.6.623. [DOI] [PubMed] [Google Scholar]
- 14.Rocca PV, Alloway JA, Nashel DJ. Diabetic muscular infarction. Semin Arthritis Rheum. 1993;22:280–7. doi: 10.1016/0049-0172(93)80076-r. [DOI] [PubMed] [Google Scholar]
- 15.Kapur S, McKendry RJ. Treatment and outcomes of diabetic muscle infarction. J Clin Rheumatol. 2005;11:8–12. doi: 10.1097/01.rhu.0000152142.33358.f1. [DOI] [PubMed] [Google Scholar]