

Abstract
To determine whether reduction of smoking via contingency management in dependent smokers would decrease the discounting of delayed reinforcers compared with smokers who did not reduce their smoking, moderate to heavy cigarette smokers were randomly assigned to one of two conditions: a contingency management condition and a control condition. In three phases (baseline discounting determination for hypothetical money and cigarettes, implementation of a contingency management or control condition, and postintervention discounting determination), the procedure to reinforce reduction in cigarette smoking produced CO decreases in all subjects exposed to that procedure. Discounting decreased significantly for both cigarettes and money among the group for whom smoking reductions were reinforced, whereas the control group showed no significant change for either commodity. Reductions in smoking can lead to reductions in discounting, and increased discounting in current smokers may be a reversible effect of nicotine dependence.
Delay discounting refers to the intuitive conception that the influence of a delayed reward decreases as a function of that delay (Logue, 1988). For instance, the subjective value (and thereby the influence) of some monetary reward available immediately is greater than the same reward available after 1 month, which is still greater than the same reward available after 1 year. Studies of delay discounting typically attempt to determine the present subjective value of rewards at numerous delays, resulting in some index of the rate of discounting.
Rate of discounting is a popular metric in studies of drug dependence, consistently showing that drug-dependent populations discount delayed rewards more than nondependent controls do (see Bickel & Marsch, 2001). Among the many drug-dependent populations who have undergone delay discounting measures are cigarette smokers. Studies by Baker, Johnson, and Bickel (2003), Bickel, Odum, and Madden (1999), Mitchell (1999), and others confirm that cigarette smokers discount delayed rewards more than nonsmokers do. A handful of studies further suggest that abstinence or reductions in smoking may affect discounting.
The effects of reduction in smoking on discounting have been examined in two types of studies: (1) effects of brief abstinence and (2) comparisons with exaddicted persons. For instance, Mitchell (2004) examined the effects of 24-hour abstinence from tobacco smoking on discounting. She employed, in addition to money discounting, an interesting variant of the discounting procedure in which smokers chose between cigarettes now and money later. Relative to usual smoking, 24 hours of smoking abstinence resulted in greater discounting of the immediate cigarette-versus-later-money choices but had no effect on the money-versus-money choices. The absence of effect of brief abstinence on money-versus-money choices is inconsistent with a prior comparable study conducted with opioid-dependent persons (Giordano et al., 2002) in which brief abstinence increased discounting for heroin-versus-heroin and money-versus-money choices. Nonetheless, the effects of brief abstinence periods reviewed above may be comparable to the response output typically associated with the introduction of extinction conditions. Extinction typically results in an initial increase in responding later followed by decreases in responding (Ferster & Skinner, 1957).
Bickel et al. (1999) examined the discounting by persons who were abstinent for longer durations. Specifically, the discounting of ex-smokers (abstinence for 1 year or longer) was compared with that of current smokers and nonsmokers. Discounting of money by ex-smokers was found to be less than that by current smokers and similar to that by nonsmokers. This observation is consistent with studies of long-term abstinence for other drug-dependent groups (Allen, Moeller, Rhoades, & Cherek, 1998; Bretteville-Jensen, 1999; Petry, 2001; but see Kirby & Petry, 2004, for mixed results).
These reported studies on abstinence are generally consistent with the observation that brief abstinence may increase discounting, while longer-duration abstinence may decrease discounting. Of course, these cross-sectional comparisons with ex dependent users must be interpreted with caution in at least two ways. First, the data are generally consistent with the notion that persons who discount less find it easier to abstain (less discounting leads to abstinence). Second, these data are also consistent with the notion that persons who stop using drugs, in turn, discount less (abstinence leads to less discounting). Of course, these hypotheses need not be mutually exclusive, and our understanding of these previous studies would be enhanced by prospective controlled experiments.
In this study, we conducted a randomized controlled trial in which one group of participants continued to smoke as normal (control group) while another group received a contingency management treatment that has been demonstrated to reduce smoking (e.g., Roll & Higgins, 2000). The discounting parameters of these randomly assigned persons were assessed for money and for cigarettes immediately before and after the contingency management treatment or control conditions.
Method
Subjects
Fifty-six cigarette smokers were recruited via advertisements and flyers. Inclusion criteria required subjects to be between 18 and 55 years of age, smoke 20 or more cigarettes per day, score a minimum of 6 on the Fagerström Tolerance Questionnaire (a test of nicotine dependence; Fagerström & Schneider, 1989), and not have proximate plans to quite smoking. Exclusion criteria included the current use of psychoactive medications and a recent history of medical problems, psychiatric disorders, or drug dependence other than tobacco dependence. Subjects were compensated with money for their participation. All participants provided informed consent prior to enrollment in the study.
Procedure
During the initial interview, participants provided a carbon monoxide (CO) breath sample (using a Bedfont EC50 Micro III Smokerlyzer; Bedfont Scientific, Medford, NJ) and were randomly assigned to one of two groups of 28 subjects each. For one group, reductions in CO were reinforced with money (the contingency group). The other group was instructed to follow their regular smoking patterns (the control group). The contingency group was instructed to continue their regular smoking patterns until the night before the imposition of the contingency procedure. This initial interview (held on Fridays between 1:00 p.m. and 3:00 p.m.) also included delay discounting procedures for cigarettes and money.
Discounting procedures
After a pretraining experience to ensure they understood the discounting procedures, participants responded on a paper-and-pencil delay-discounting questionnaire (Rachlin, Raineri, & Cross, 1991). In this questionnaire, subjects made a series of choices between a later amount and a sooner amount of monetary reward. For example, the first item asked subjects to choose between $1,000 now and $1,000 in 1 week. On the next question, the later item remained $1,000 in 1 week, while the sooner amount dropped to $990 now. In the following questions, the sooner amount continued to decrease. The amounts for the sooner reward were $1,000, $990, $960, $920, $850, $800, $750, $700, $650, $600, $550, $500, $450, $400, $350, $300, $250, $200, $150, $100, $80, $60, $40, $20, $10, $5, and $1. Subjects marked an “X” next to either the sooner or later amount for each question. Then the procedure was repeated, with the later choice being $1,000 in 2 weeks. The procedure was completed for the following delays: 1 week, 2 weeks, 1 month, 6 months, 1 year, 5 years, and 25 years.
Next, the procedure was repeated with cigarette amounts. Pilot data revealed that subjects could purchase an average of 420 packs of cigarettes with $1,000. Therefore, all choices started with 420 packs now or 420 packs delayed, and the immediate cigarette amount decreased by the same proportion as the money choices in each question. Cigarettes were expressed in terms of cartons, packs, and individual cigarettes where appropriate.
The indifference point (i.e., the amount of the smaller immediate award deemed subjectively equivalent to the larger delayed reward) was defined for each subject at each delay as the mean of the ascending and descending switch of preference between the immediate and delayed rewards (expressed as a proportion of the larger, later outcome). The switch of preference within each of these series (ascending and descending) was defined as the mean of the two magnitudes surrounding the switch.
Contingency and control conditions
During the following Monday through Friday, subjects in the contingency group were required to visit the laboratory three times per day. These visits occurred in the morning (9:00–11:00 a.m.), afternoon (3:00–5:00 p.m.), and evening (8:00–10:00 p.m.). On each visit, the subject provided a CO breath sample. CO measures between 8 and 10 parts per million (ppm) are frequently used as the cutoff between smokers and nonsmokers (Jarvis, Tunstall-Pedoe, Feyerabend, Vesey, & Saloojee, 1987; Morabia, Bernstein, curtin, & Berode, 2001). Given the contingency was meant for reduced smoking, CO = 12 ppm is associated with a minimum of 29% average reduction in CO for the present sample (12 ppm also is associated with the 75th percentile for smokers similar to those in the present study; Javors, Hatch, & Lamb, 2005). If the CO sample was under 12 ppm, the subject was given $10 in cash. If a CO sample was 12 ppm or above, then money was withheld from the subject. Although subjects were told that this measure detected recent smoking, they were not told the specific numeric criterion, nor were they given numeric feedback on CO reading measurements. (Though it was clear to subjects that other sources of nicotine should be avoided, we did not assess this avoidance.) Subjects in the control group were not required to come in during this week, although both groups were allowed to come in each day and pick up a free pack of their normal brand of cigarettes for the day (two packs for those who normally smoked more than one). Therefore, any abstinence or reduction in smoking among the contingency group could not be attributed to a lack of cigarettes or money to buy cigarettes. Subjects were brought in for another session on Friday (1 week after the initial session). On this day between the hours of 12:00 noon and 5:00 p.m. (before the evening CO measurement in all cases), identical questionnaires were administered in the same manner as the first Friday. Participants were compensated $90 for coming to the consent session, completing all assessments, and attending all sessions.
Statistical Methods
The free parameter in a reparameterized version of Mazur’s (1987) hyperbolic function (see the equation, below) was used to index an individual’s relative preference for small, immediate rewards to larger, delayed rewards (discounting rate g).
Via a nonlinear regression on days of delay (d), the indifference points (vd) from an individual were modeled as having additive, normal errors that have a mean of zero. With g = ln(k), the regression mean is the same as Mazur’s originally proposed hyperbolic function, with interpretation of discounting rate also remaining the same (that higher discounting rate means lower indifference points and greater discounting). Estimating g instead of k (Mazur’s discounting rates are generally not normally distributed) is desirable in that estimated g’s are approximately normal (Richards, Zhang, Mitchell, & de Wit, 1999) and, more important, that standard errors of g (i.e., a standard error for each discounting rate determination) may be easily obtained for weighting purposes in subsequent analyses. By using these standard errors in the weighting of the g’s, we account for the heterogeneous variability in the estimated g’s across individuals. (Some subjects give more predictable answers to delay discounting tasks than others do.) To evaluate within-individual changes in k between two conditions (e.g., cigarettes [C] and money [M] at baseline), we directly estimated gC − gM = ln(kC/kM). Estimated discounting parameters, weighted by their estimated precisions (i.e., the reciprocals of the squared standard errors), were then analyzed by using analysis of variance (ANOVA). Estimated effect means are the best linear unbiased estimates (Draper & Smith, 1981). All analyses were conducted in SAS/STAT Version 9.1. The threshold for statistical significance was set at 0.05.
Results
Subject Characteristics
Subjects randomly assigned to the two groups did not differ significantly on any measured demographic characteristics (see Table 1). Correlation analyses, based on Spearman’s rank correlation, failed to document any significant relationship between measured subject characteristics at baseline and treatment outcome. Observed correlations between measured subject characteristics and derived discounting parameters ranged from approximately −0.20 to +0.20.
Table 1.
Subject Characteristics, by Group
| Characteristic | Control (n = 28) | Contingency (n = 28) | p |
|---|---|---|---|
| Age (years) | 25.2 ± 9.8 | 26.6 ± 8.1 | 0.57 |
| Male (%)* | 68 | 61 | 0.58 |
| Income per month ($US) | 212 ± 110 | 291 ± 83 | 0.57 |
| Cigarettes per day | 24.1 ± 6.1 | 23.2 ± 5.3 | 0.56 |
| Fagerström score | 7.3 ± 1.4 | 7.1 ± 1.1 | 0.60 |
| CO baseline level | 21.6 ± 7.7 | 20.1 ± 7.8 | 0.46 |
| Years smoked | 9.9 ± 10.6 | 10.7 ± 8.2 | 0.75 |
| Previous quit attempts (%)* | 55 | 78 | 0.13 |
| Other drug use (%)* | 64 | 54 | 0.42 |
Note. Tabled values represent mean ± standard deviation unless otherwise indicated; significance based on two-sample t test.
Significance based on chi-square test.
Reductions in CO
The effects of the contingency on CO in the treatment group are shown in Figure 1. The mean CO reading across the group was greater than 20 ppm at baseline and below the 12 ppm CO criterion for each of the 15 CO readings during the contingency procedure (top panel). Mean CO levels at each of the 15 assessments are significantly different from baseline for subjects in this group. All 28 subjects decreased their CO levels relative to baseline, with approximately 90% of subjects achieving levels of 12 ppm or below at each assessment (bottom panel). The mean reduction in CO for all subjects in the treatment group was 55%.
Figure 1.

Upper panel shows the mean carbon monoxide (CO) readings among the group that received monetary compensation for CO < 12 ppm at baseline and at each of the 15 CO assessments. Lower panel shows the percentage of the group that provided CO < 12 ppm across the same assessments.
Delay Discounting
To ensure that the control and contingency groups did not differ prior to treatment, we tested for mean differences in (weighted) logged discounting parameters between the two groups for money and cigarettes by using independent sample t tests. Prior to the treatment, the two groups did not differ for money, t(54) = −1.31, p = 0.20, or cigarettes, t(54) = −1.84, p = 0.07. Though the differences were not significant, the control group discounted less then the contingency group for each commodity.
As all participants were assumed to come from the same population prior to the contingency procedure (henceforth, pretreatment), discounting parameters were compared between money and cigarettes across all participants. As expected, greater discounting was observed for cigarettes than for money, mean log difference = 0.69, t(55) = 3.16, p < 0.01. The top panel of Figure 2 displays the median pre- and posttreatment indifference points for money as a function of delay with best-fitting hyperbolic curves. The bottom panel of Figure 2 displays the same data for cigarettes. After the contingency procedure (henceforth, posttreatment), we accounted for the treatment group by using a one-factor ANOVA (see bottom of Figure 2). Both the control and contingency groups discounted money more than cigarettes, t(54) = 3.57, p < 0.001, and t(54) = 3.99, p < 0.001, respectively.
Figure 2.
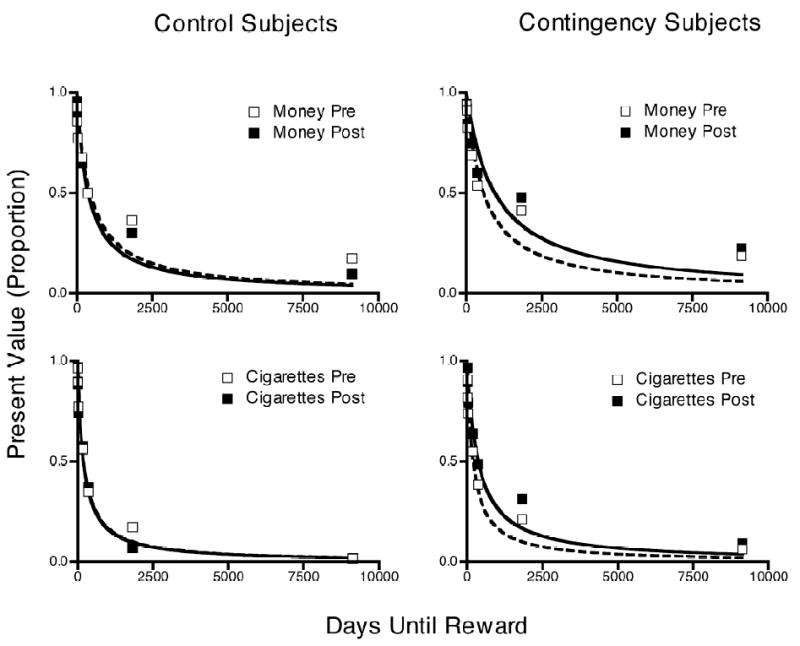
Indifference points are shown for hypothetical money (upper panels), and cigarettes (lower panels) for those who were (right panels) and were not (left panels) exposed to the contingency for CO < 12 ppm.
Pre- and posttreatment comparisons of discounting from participants in the control and contingency conditions were conducted to examine possible changes in discounting rates over time. We did this by analyzing estimated gpost – gpre values with a weighted least squares comparison, with treatment as the factor. The means from each condition were then compared with zero by using a t test (having 54 degrees of freedom). The control group did not significantly differ in their discounting of money between pre- and posttreatment, t(54) = 0.02, p = 0.98. Pre- and posttreatment of cigarette discounting in the control group was also not significantly different, t(54) = −0.57, p = 0.57. In contrast, a statistically significant decrease, t(54) = −2.20, p = 0.03, in discounting of money was observed in the contingency condition; discounting rate decreased for participants in the contingency condition in the posttreatment session. A decrease in the discounting of cigarettes was also observed for the contingency group from pre- to posttreatment, t(54) = −2.92, p = 0.01.
Finally, the variances of the discounting rates in each of the eight unique combinations of conditions (pre- vs. posttreatment, money vs. cigarettes, control vs. contingency group) were examined. The control group had a significantly higher variance in discounting of cigarettes than the contingent group prior to treatment, F(27, 27) = 3.62, p < 0.01. This significant difference is attributed to random chance according to the treatment assignment scheme. A likelihood ratio test was used to assess whether a group’s variability in discounting changed from pre- to posttreatment. For each group × commodity, a pre- and posttreatment repeated measures ANOVA was conducted. Twice the negative ratio of the residual loglikelihoods from these two models has an (approximate) chi-square distribution with 1 degree of freedom. The control group decreased variability in discounting of cigarettes posttest, χ2(1) = 5.85, p = 0.03, and the contingent group increased variability in discounting of cigarettes, χ2(1) = 7.70, p = 0.01, but no significant changes in the variability of the discounting of money was observed for either of the two groups.
Discussion
In this randomized controlled experiment, reductions in measures of CO (i.e., reductions in smoking) were reinforced in the contingency group, while the control group smoked in their usual fashion. Delay discounting for cigarettes and money was measured prior to and following the 5-day period during which reductions in CO were reinforced in the contingency group. First, we replicated prior findings that cigarette smokers discount cigarettes more than a comparable amount of money (Bickel et al., 1999). Overall, we observed a significant reduction in the discounting of money and cigarette rewards in the contingency group, with no change observed in the control group.
First, the present results replicate prior studies demonstrating that the drug of dependence produces greater discounting than a comparable amount of money. Even when discounting decreased in the experimental group that underwent the contingency management procedure, both commodities maintained their relative position in terms of degree of discounting. Prior studies have demonstrated that heroin-, alcohol-, and cigarette-dependent persons discount their drug of dependence more rapidly than money (Bickel et al., 1999; Petry 2001; Madden, Petry, Badger, &Bickel, 1997). Intriguingly, discounting appears to affect other commodities or events, such as money in the current study and health in other studies (e.g., Baker et al., 2003). An important question is whether the greater discounting observed with commodities other than money is limited to only those commodities functionally related in some way to the drug dependence or whether the effect is pervasive across all commodities (e.g., Odum & Rainaud, 2003).
Second, the results of the present experiment are consistent with the results of a prior cross-sectional study in which the discounting of ex- and current smokers was compared. That study demonstrated that persons who were ex-smokers for a year or longer discounted less than current smokers (Bickel et al., 1999; c.f., Petry, 2001; see Kirby & Petry, 2004, for an exception). The study of ex-smokers also showed that they discount money to the same extent as those who had never been smokers (Bickel et al., 1999). The present study suggests that the results from prior cross-sectional studies in which both current and ex-smokers were compared are due, at least in part, to changes in drug use and other related processes. That said, the present results do not rule out the possibility that persons who discount less will be more interested in or have more success at achieving abstinence. Nonetheless, the present results suggest that greater discounting is a reversible effect of drug use.
Third, an interesting result of the present study is that the discounting rate changed in merely 5 days. Such an observation suggests that discounting may provide a measure of local conditions of participants as opposed to, or in addition to, long-enduring behavioral traits. If the preceding statements are accurate, then they would suggest a point of divergence between discounting and personality measures of impulsivity. Moreover, if discounting did serve as a measure of local conditions, then perhaps discounting may be influenced by a variety of local factors, such as stress. For example, in two studies the effects of brief drug deprivation (e.g., opioid withdrawal or brief smoking abstinence) on discounting were examined. One showed that deprivation increased the temporal discounting of drug and money (Giordano et al., 2002), while the other showed that brief smoking abstinence increased the temporal discounting related to cigarettes but not to money (Mitchell, 2004). The increase in discounting that followed deprivation in these prior studies may appear to be inconsistent with the present study. Perhaps if discounting was measured during the 5-day interval when the contingency management procedure was imposed in the present study, then discounting may have initially increased and subsequently decreased in correspondence with changes in withdrawal. If this hypothesis is confirmed by future studies, it would suggest that discounting may be biphasic during drug discontinuation. The observations of Mitchell (2004) that brief cigarette deprivation affects only cigarette discounting could result from several procedural differences, such as the inclusion criteria that permitted subjects who smoked a fewer number of cigarettes per day and the smaller magnitudes of money that were discounted.
A number of limitations of the current study may affect the interpretation of the results. One limitation is that only the control group received money for participation, while the experimental group received additional money for smoking reduction and more frequent contact with the research laboratory and staff. An alternative explanation is that the additional monies received by the contingency group, rather than the reduction in smoking, produced the change in discounting for money. (Green, Myerson, Lichtman, Rosen, & Fry, 1996, found changes in discounting as a function of income.) Given no differences in the variances of money-discounting rates between the contingency and control groups posttreatment, we believe that money does not provide an adequate alternative explanation; greater variance in monies received by the contingency group condition (by those who met the contingency and those who did not) would result in higher variance in k values posttreatment relative to controls. In addition, the money interpretation would not explain changes in discounting of cigarette smoking (since both groups received cigarettes). The argument could also be made that the brief contact with the research staff, rather than the reduction in smoking, decreased discounting. We cannot definitively rule out this possibility, since to our knowledge, there are no published studies of the effect of social interaction on discounting. Nonetheless, subsequent studies would benefit from giving subjects in the control group the same contact with research staff and monetary payment of the same magnitude and in the same temporal pattern as the experimental group but independent of smoking reduction.
Another limitation of the present study is that since hypothetical results were employed, then the discounting results may be spurious. Such an explanation is unlikely, because we would not expect spurious data to be orderly as a function of treatment group assignment, nor would we expect the hyperbolic equation to fit spurious data. Also, studies have shown that comparable results are obtained when discounting of real and hypothetical money is assessed in both healthy volunteers and cigarette smokers (Baker et al., 2003; Johnson & Bickel, 2002; Johnson, Bickel, & Baker, 2007; Lagorio & Madden, 2005; Madden, Begotka, Raiff, & Kastern, 2003; Madden, Raiff, Lagorio, Begotka, Mueller, Hehli, et al., 2004). A third limitation is that the CO threshold used in this study required reduction in smoking but not abstinence. Therefore, the effects of abstinence on discounting remain to be determined. Finally, the low income of the subjects in the present study must be considered; similar results may not be observed with the present procedure for participants with greater income.
Questions that remain include whether the results described in the present study could be systematically replicated with other drug-dependent populations, whether comparable results could be obtained with treatments other than contingency management (i.e., medications), and whether the degree of discounting would increase after posttreatment relapse. Such studies will more completely describe the relation of delay discounting to cigarette smoking.
Expanded understanding of the direction of the relationship between cigarette smoking (and other forms of drug dependence) and impulsivity may have significant impact on our understanding of the behavioral consequences of drug use. If cigarette and drug use do increase impulsiveness or reduce the temporal horizon (or any of the constructs that temporal discounting is thought to index), it may promote a host of other behavioral problems, including further cigarette or drug use. If this relationship is bidirectional (as the current study suggests), it would imply that abstinence not only has the benefit of abstinence per se but may also lead to the reduction of other behavioral problems that cigarette and drug use promote.
Acknowledgments
This work was performed at the University of Vermont in Burlington and was supported by National Institute on Drug Abuse Grants RO1 DA 11692 and T32 DA 07242. The authors thank Benjamin Kowal for comments about an earlier draft.
Contributor Information
Richard Yi, University of Arkansas for Medical Sciences, Little Rock.
Matthew W. Johnson, Johns Hopkins University School of Medicine, Baltimore
Louis A. Giordano, Duke University Medical Center, Durham, NC
Reid D. Landes, University of Arkansas for Medical Sciences, Little Rock
Gary J. Badger, University of Vermont, Burlington
Warren K. Bickel, University of Arkansas for Medical Sciences, Little Rock
References
- ALLEN TJ, MOELLER G, RHOADES HM, CHEREK DR. Impulsivity and history of drug dependence. Drug and Alcohol Dependence. 1998;50:137–145. doi: 10.1016/s0376-8716(98)00023-4. [DOI] [PubMed] [Google Scholar]
- BAKER F, JOHNSON MW, BICKEL WK. Delay discounting in current and never-before cigarette smokers: Similarities and differences across commodity, sign, and magnitude. Journal of Abnormal Psychology. 2003;112:382–392. doi: 10.1037/0021-843x.112.3.382. [DOI] [PubMed] [Google Scholar]
- BICKEL WK, MARSCH LA. Towards a behavioral economic understanding of drug dependence: Delay discounting processes. Addiction. 2001;96:73–86. doi: 10.1046/j.1360-0443.2001.961736.x. [DOI] [PubMed] [Google Scholar]
- BICKEL WK, ODUM AL, MADDEN GL. Impulsivity and cigarette smoking: Delay discounting in current, never, and ex-smokers. Psychopharmacology. 1999;146:447–454. doi: 10.1007/pl00005490. [DOI] [PubMed] [Google Scholar]
- BRETTEVILLE-JENSEN AL. Addiction and discounting. Journal of Health and Economics. 1999;18:393–407. doi: 10.1016/s0167-6296(98)00057-5. [DOI] [PubMed] [Google Scholar]
- DRAPER NR, SMITH H. Applied regression analysis. 2. New York: Wiley; 1981. pp. 108–116. [Google Scholar]
- FAGERSTRÖM KO, SCHNEIDER NG. Measuring nicotine dependence: A review of the Fagerström Tolerance Questionnaire. Journal of Behavioral Medicine. 1989;12:159–182. doi: 10.1007/BF00846549. [DOI] [PubMed] [Google Scholar]
- FERSTER CB, SKINNER BF. Schedules of reinforcement. New York: Appleton-Century-Crofts; 1957. [Google Scholar]
- GIORDANO LA, BICKEL WK, LOEWENSTEIN G, JACOBS EA, MARSCH L, BADGER GJ. Mild opioid deprivation increases the degree that opioid-dependent outpatients discount delayed heroin and money. Psychopharmacology. 2002;163:174–182. doi: 10.1007/s00213-002-1159-2. [DOI] [PubMed] [Google Scholar]
- GREEN L, MYERSON J, LICHTMAN D, ROSEN S, FRY A. Temporal discounting in choice between delayed rewards: the role of age and income. Psychology of Aging. 1996;11:79–84. doi: 10.1037//0882-7974.11.1.79. [DOI] [PubMed] [Google Scholar]
- JARVIS MJ, TUNSTALL-PEDOE H, FEYERABEND C, VESEY C, SALOOJEE Y. Comparison of tests used to distinguish smokers from nonsmokers. American Journal of Public Health. 1987;77:1435–1438. doi: 10.2105/ajph.77.11.1435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- JAVORS MA, HATCH JP, LAMB RJ. Cut-off levels for breath carbon monoxide as a marker for cigarette smoking. Addiction. 2005;100:159–167. doi: 10.1111/j.1360-0443.2004.00957.x. [DOI] [PubMed] [Google Scholar]
- JOHNSON MW, BICKEL WK, BAKER F. Moderate drug use and delay discounting: a comparison of heavy, light, and never smokers. Experimental and Clinical Psychopharmacology. 2007;15:187–194. doi: 10.1037/1064-1297.15.2.187. [DOI] [PubMed] [Google Scholar]
- JOHNSON MW, BICKEL WK. Within-subject comparison of real and hypothetical money rewards in delay discounting. Journal of the Experimental Analysis of Behavior. 2002;77:129–146. doi: 10.1901/jeab.2002.77-129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- KIRBY KN, PETRY NM. Heroin and cocaine abusers have higher discount rates for delayed rewards than alcoholics or non-drug-using controls. Addiction. 2004;99:461–471. doi: 10.1111/j.1360-0443.2003.00669.x. [DOI] [PubMed] [Google Scholar]
- LAGORIO CH, MADDEN GJ. Delay discounting of real and hypothetical rewards III: Steady-state assessments, forced-choice trials, and all real rewards. Behavioural Processes. 2005;69:173–187. doi: 10.1016/j.beproc.2005.02.003. [DOI] [PubMed] [Google Scholar]
- LOGUE AW. Research on self-control: An integrating framework. Behavioural and Brain Sciences. 1988;11:665–709. [Google Scholar]
- MADDEN GJ, PETRY NM, BADGER GJ, BICKEL WK. Impulsive and self-control choices in opioid-dependent patients and non-drug-using control participants: Drug and monetary rewards. Experimental and Clinical Psychopharmacology. 1997;5:256–62. doi: 10.1037//1064-1297.5.3.256. [DOI] [PubMed] [Google Scholar]
- MADDEN GJ, BEGOTKA AM, RAIFF BR, KASTERN LL. Delay discounting of real and hypothetical rewards. Experimental and Clinical Psychopharmacology. 2003;11:139–145. doi: 10.1037/1064-1297.11.2.139. [DOI] [PubMed] [Google Scholar]
- MADDEN GJ, RAIFF BR, LAGORIO CH, BEGOTKA AM, MUELLER AM, HEHLI DJ, WEGENER AA. Delay discounting of potentially real and hypothetical rewards: II. Between- and within-subject comparisons. Experimental and Clinical Psychopharmacology. 2004;12:251–261. doi: 10.1037/1064-1297.12.4.251. [DOI] [PubMed] [Google Scholar]
- MAZUR J. An adjusting procedure for studying delayed reinforcement. In: Commons M, Mazur J, Nevin J, Rachlin H, editors. The effect of delay and of intervening events on reinforcement value. Hillsdale, NJ: Erlbaum; 1987. pp. 55–73. [Google Scholar]
- MITCHELL SH. Measures of impulsivity in cigarette smokers and non-smokers. Psychopharmacology. 1999;146:455–464. doi: 10.1007/pl00005491. [DOI] [PubMed] [Google Scholar]
- MITCHELL SH. Effects of short-term nicotine deprivation on decision-making: Delay, uncertainty, and effort discounting. Nicotine & Tobacco Research. 2004;6:819–828. doi: 10.1080/14622200412331296002. [DOI] [PubMed] [Google Scholar]
- MORABIA A, BERNSTEIN MS, CURTIN F, BERODE M. Validation of self-reported smoking status in simultaneous measurement of carbon monoxide and salivary thiocyanate. Preventive Medicine. 2001;32:82–88. doi: 10.1006/pmed.2000.0779. [DOI] [PubMed] [Google Scholar]
- ODUM AL, MADDEN GJ, BICKEL WK. Discounting of delayed health gains and losses by current, never and ex-smokers of cigarettes. Nicotine & Tobacco Research. 2002;4:295–303. doi: 10.1080/14622200210141257. [DOI] [PubMed] [Google Scholar]
- ODUM AL, RAINAUD CP. Discounting of delayed hypothetical money, alcohol, and food. Behavioural Processes. 2003;64:305–313. doi: 10.1016/s0376-6357(03)00145-1. [DOI] [PubMed] [Google Scholar]
- PETRY NM. Delay discounting of money and alcohol in actively using alcoholics, currently abstinent alcoholics, and controls. Psychopharmacology. 2001;154:243–250. doi: 10.1007/s002130000638. [DOI] [PubMed] [Google Scholar]
- RACHLIN H, RAINERI A, CROSS D. Subjective probability and delay. Journal of the Experimental Analysis of Behavior. 1991;55:233–244. doi: 10.1901/jeab.1991.55-233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- RICHARDS JB, ZHANG L, MITCHELL SH, DE WIT H. Delay or probability discounting in a model of impulsive behavior: effect of alcohol. Journal of the Experimental Analysis of Behavior. 1999;71:121–143. doi: 10.1901/jeab.1999.71-121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- ROLL JM, HIGGINS ST. A within-subject comparison of three different schedules of reinforcement of drug abstinence using cigarette smoking as an exemplar. Drug and Alcohol Dependence. 2000;58:103–109. doi: 10.1016/s0376-8716(99)00073-3. [DOI] [PubMed] [Google Scholar]