

Abstract
Objective
Transradial angiography has become popular among many cardiologists as a diagnostic and therapeutic tool. However, transradial cerebral angiography is not utilized to the same extent. The purpose of this study is to present our experience regarding the usefulness of transradial cerebral angiography, especially in elderly patients.
Methods
Between May 2011 and February 2012, a total of 126 cerebral angiographies were performed via a transradial approach in a single center. Of them, only 47 patients were over 60 years old. In our institution, we shifted the initial access from the right femoral artery to the right radial artery in all patients requiring cerebral angiography in 2011. We did not attempt radial access in 40 cases for variable reasons.
Results
The procedural success rate was 92.2%. We have four failures of transradial angiography; two because of loop formations of the radial and brachial artery and two due to multiple puncture failures. All supra-aortic vessels were successfully catheterized. However, the selective catheterization rates of the left side distal vessels were lower, as success rates were 89.7% for the right internal carotid artery and 75% for the left internal carotid artery. Procedure-related vascular complications, such as puncture site hematoma, hand ischemia, pseudoaneurysm, arteriovenous fistula and arterial dissection were not observed in our series. However, intraprocedural thrombosis developed in one patient, which was resolved completely by intraarterial thrombolytic agents.
Conclusion
With advancing patient's age, we believe that transradial cerebral angiography is a useful tool to decrease patient's discomfort and more effectively manage the vessel tortuosity.
Keywords: Angiography, Cerebral angiography, Radial artery, Transradial
INTRODUCTION
Due to progress in cerebrovascular imaging methods, such as magnetic resonance (MR) angiography and three-dimensional CT angiography, there is increased interest in cerebrovascular disease in ageing society. Many cerebrovascular diseases are worked up through health screening, which prevent cerebrovascular events. However, cerebral catheter angiography remains the gold standard method for examining the vasculature of patients with cerebrovascular disease. In most institutions, the right femoral artery is usually selected as the main vascular access for performing cerebral angiography, because of the clinicians' familiarity and its convenience. Transfemoral angiography has some limitations. Many patients suffer from hematomas or bruising in the groin. Additionally, pseudoaneurysms or arteriovenous fistulae of the puncture site are rare but do occur. It cannot be used when patients have extensive atherosclerotic disease or atypical anatomy in their aortic arch or brachiocephalic vessel, femoral artery occlusion or abnormality. To avoid these problems and limitations, we performed transradial access for the preceding year.
The purpose of this study is to describe the efficacy of transradial angiography by a single operator's experience for one year, especially in elderly patients.
MATERIALS AND METHODS
Patient selection
Between March 2011 and February 2012, 244 patients underwent selective cerebral angiography with digital subtraction angiography in our institution. For 126 patients (51.64%), the procedure was performed via a transradial approach for the evaluation of cerebrovascular disease. These patients ranged in age from 17 to 78 years (mean age, 56.2 years) and included 73 women and 53 men. There were 47 patients over the age of 60; 25 women and 22 men. Additionally, 91 of the total 244 patients receiving a cerebral angiography were over the sixty, 47 underwent transradial access and 44 underwent transfemoral access. Patients requiring interventional procedures were excluded. After a one-year neurointerventional learning period with 322 cerebral angiographic cases in another institution, we shifted the initial access from the right femoral artery to the right radial artery in all patients requiring cerebral angiography. The indications for cerebral angiography are listed in Table 1 for patients over the age of 60. We did not attempt radial access in 40 of these patients for various reasons (Table 2). Our institutional review board approved these informed consents.
Table 1.
Indications for transradial cerebral angiography in patients with age >60 years
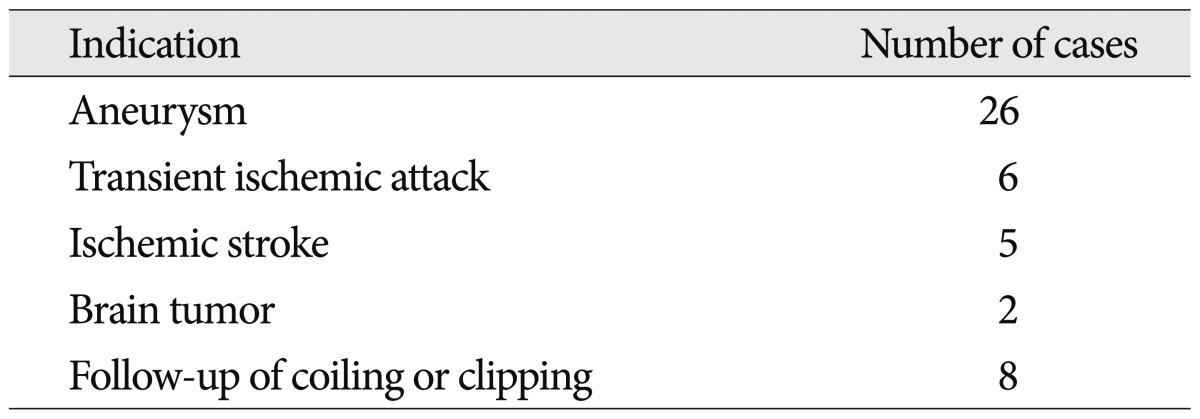
Table 2.
The reasons for initial transfemoral access in patients with age >60 years
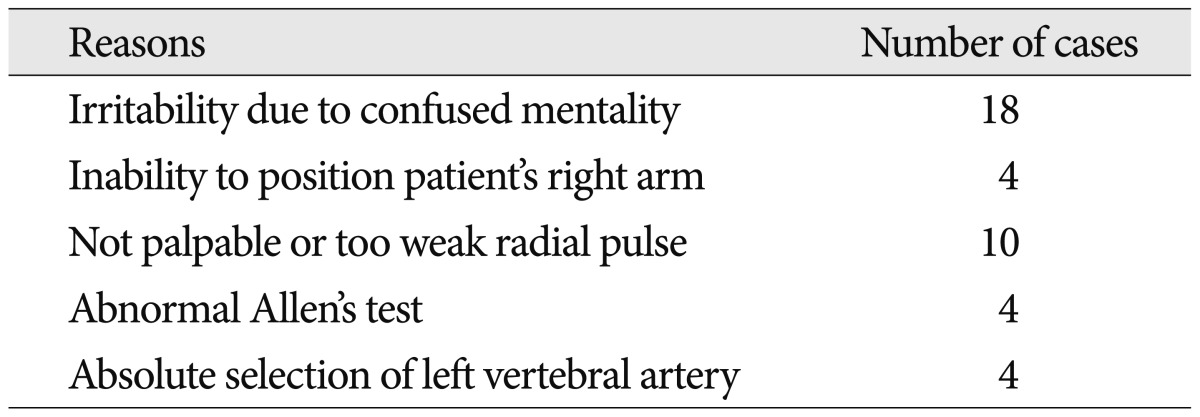
There were four cases excluded due to failure of transradial access; two loop formations of radial artery and two multiple puncture failures
Instruments and techniques
Patients were brought to the angiographic suite. All procedures were performed for diagnostic purposes. We performed all the transradial approaches via the right side. If the right side was not available, we did not proceed with the transradial approach because performing this procedure via the left radial artery was very inconvenient. In these cases, we performed a right transfemoral approach. All patients underwent a modified Allen's test of the right wrist to evaluate satisfactory collateral perfusion prior to the procedure. If the test was abnormal, we did not proceed with radial artery access. After ulnar artery patency was proven via modified Allen's test, patients were prepared and draped with the right radial artery site exposure at the wrist and the right arm abducted at a 70-degree angle. The right inguinal area was also draped as well, for conversion of the access route from the wrist to the groin if necessary. A small amount of 2% lidocaine was infiltrated into the subcutaneous tissue on the radial artery around the styloid process of the radius, and the artery was punctured at the point of maximum pulsation using a 20-gauge needle with a modified Seldinger technique. A 5-French introducer sheath (Terumo Radifocus, Tokyo, Japan) was then placed within the artery. To prevent vasospasm of the artery, a diluted solution of nitroglycerine (200 µg/mL; 0.25 mL), verapamil (2.0 mg), heparin (5000 IU/mL) was injected intra-arterially through the side port of the introducer, which was then continuously flushed with pressurized (300 mm Hg), heparinized saline (5000 IU per 1000 mL of normal saline) during the procedure. A 5-French Simmons type 2 catheter (Terumo Radifocus, Tokyo, Japan) was inserted and forearm angiography performed through the catheter to confirm there was satisfactory collateral perfusion. Under fluoroscopy monitoring, a 5-French Simmons 2 catheter was advanced over a 0.035-inch hydrophilic guidewire (Terumo Radifocus, Tokyo, Japan) through the radial artery to the brachial artery, then through the axillary artery into the subclavian artery in all cases. Guidewire was subsequently advanced to the ascending aorta and turned back at the aortic valve for the reconstitution of the natural Simmons configuration of the catheter. After the catheter was reconstituted, the catheter tip was controlled to select the orifice of the target artery [the innominate artery, left common carotid artery (CCA) or the left subclavian artery], and then advanced to the distal selection [the internal carotid artery (ICA) or vertebral artery]. After the procedure, the catheter and sheath were removed, and a superficial pressure dressing with a radial artery hemostatic device (Hangshou Alicon Pharm Co., LTD, Zhejian, China) was applied to the radial artery puncture site. Patients were observed for three hours before discharge. During this observation period, their activity was not limited to bed rest.
RESULTS
In patients over the age of 60, radial access was successful in 47 of 51 cases, a success rate of 92.2%. Transfemoral approach was performed in the four patients with failed radial artery access. This was attributed to failure of the radial puncture, loop formation or tortuosity at the proximal end of the radial artery in two patients, and severe vasospasm of the radial artery following multiple puncture trials in two patients (Fig. 1). All supra-aortic vessels were successfully catheterized. However, selective catheterization rates of the left-sided distal vessels were lower, with success rates of 89.7% (26/29) for the right ICA and 75% (27/36) for the left ICA. Patients were excluded when it was deemed impossible or dangerous to catheterize the ICA because of severe stenosis or atheromatous plaques. We did not attempt to select the vertebral artery routinely, if there was not found the legions at previous CT angiography or MR angiography. Two procedures using the same radial artery were performed in two patients (4.3%). Among these patients, radial artery occlusion or stenosis was not demonstrated on follow-up cerebral angiography. In all patients in whom the transradial angiography was successful, the diagnostic adequacy and quality of images were satisfactory.
Fig. 1.

Loop formations as a cause of transradial approach failure (black arrows). These conditions make it difficult to introduce the guidewire and catheter because of loop formation of the brachial (A) and radial (B) arteries. Transradial approach failed in these cases.
Pain in the forearm or arm developed in three patients during the procedures, but it was usually mild and transient. Vasospasm of the radial artery was noted in two cases. Spasms were effectively resolved with the combined solution of nitroglycerin, verapamil, and heparin. Procedure-related vascular complications, such as puncture site hematoma, hand ischemia, pseudoaneurysm, arteriovenous fistula and arterial dissection, were not seen in our series. No patients had functional disability of the hand, and no complaints of discomfort were reported on the questionnaire. However, intraprocedural thrombosis developed in one patient and aggravation of a pre-existing neurologic deficit was noted (Fig. 2). Chemical thrombolysis was performed through the transradial route and the thrombus was removed completely. The patient's symptom was improved after one day without further sequelae.
Fig. 2.

Acute thrombosis developed during transradial cerebral angiography of the right middle cerebral artery (A). And then, it resolved after intraarterial thrombolytic agents (B).
DISCUSSION
The transradial approach was introduced for the first time in 1998 in coronary angiography2). It was contributed to reduce puncture site complication and the discomfort of the patients. Transradial approach has become popular among a majority of interventional cardiologists as a diagnostic and therapeutic tool in a number of centers worldwide because of its low puncture site complication rate, as compared with the transfemoral approach, for patients undergoing anticoagulation therapy8-11). The transradial approach in cerebral angiography and neurointervention was introduced in 200014). Some authors expected that the transradial approach could be a gold standard for cerebral angiography17), although the transfemoral approach is usually favored in almost centers because of familiarity and convenience.
The femoral artery is the most common puncture site used for cerebral angiography, because most angiographers and neurointerventionalists are comfortable using this access for the entire cerebral vascular system. However, there are some limitations. Transfemoral approach cannot be used when patients have extensive atherosclerotic disease in their aortic arch, atypical anatomy of their aortic or brachiocephalic vessels, dissection of the thoracic artery, iliofemoral occlusive disease, or groin infection1,3,7). Additionally, this procedure can lead to several complications, such as retroperitoneal hematoma, pseudoaneurysm formation, arteriovenous fistula formation, femoral nerve injury, lower limb ischemia, and pulmonary embolism7,12,13,15,18). One of the major limitations of the transfemoral approach is the requirement for 4 to 6 hours of leg immobilization and bed rest to prevent bleeding complications at the femoral access site13). At times, duration of the leg immobilization was greatly reduced by application of percutaneous closure devices. However, these devices were expensive.
Transradial approach has the most important advantage of easy hemostasis. Compared with a groin hematoma formation rate with transradial approach reported as high as 10%16). Transfemoral approach may cause more suffering for the patients, particularly for those with advanced age, degenerative spine or spinal lesions, or benign prostate hypertrophy, because these conditions require complete bed rest for at least several hours following femoral artery puncture19). Furthermore, after the transfemoral approach, patients are usually kept in the hospital overnight for observation. In contrast, transradial approach does not require bed rest and allows the patient to be ambulatory immediately without the restriction of arm movement after procedure. In our institution, after transfemoral approach, we perform manual compression for 15 minutes without the use of additional percutaneous groin closure devices in the angiographic suite. However, transradial approach does not take the time for the compression. It is not necessary to compress the puncture site manually, as a simple compression device is sufficient to achieve hemostasis without special precautions. We generally observe patients for six hours with leg immobilization after transfemoral angiography. It is quite uncomfortable for patients and may lead to anxiety toward future angiographic trials. However, transradial angiography does not require prolonged observation. It takes 3 hours for observing patients and allows cerebral angiography to be easily performed on out-patient basis, useful for the image follow-up of patients after neurointerventional procedures.
The transradial approach is especially useful for patients with obesity or severe atherosclerotic change of bilateral femoral arteries, as the radial artery is an easier and safer access route15). In these cases, femoral artery puncture may often fail due to its deep location and weak pulsation. However, radial artery is superficially located on the underlying firm tendon, relatively fixed, easily compressible, and, most important, not an end artery. Since no major nerves or veins run in the vicinity of the radial artery over the radial styloid, neuropathies or arteriovenous fistulas are less likely to occur15).
Transradial cerebral angiography has some advantages after the administration of anticoagulants or with effective antiplatelet therapy13,15,17). In the elderly, as the rate of atherosclerotic cerebrovascular and coronary diseases increase, anticoagulation or antiplatelet therapies are more common. These conditions are a contraindication for femoral approach, secondary to the potential for neurologic compromise caused by a large hematoma17). It is usually necessary to discontinue the anticoagulant or antithrombotic agents before the procedure to reduce the risk of serious hemorrhagic complications. Additionally, it may be difficult and time consuming to restart and readjust the level of anticoagulation after angiography, if this has been stopped for the angiogram. However, transradial approach does not require these agents to be discontinued. 17 (36.2%) of the 47 patients in our series received anticoagulant and/or antiplatelet therapy perioperatively in our series, no major hemorrhagic complications experienced, such as significant puncture site hematoma, pseudoaneurysm, or arteriovenous fistula formation. Therefore, it is reasonable to expect that anticoagulant and antiplatelet therapies need not be discontinued for cerebral angiography via transradial approach. In addition, it may actually reduce the intraprocedural thromboembolic complications if these agents are continued or added. We also recommend the use of pressurized, heparinized saline for the continuous flushing of the introduce sheath in order to prevent thrombosis.
With advancing patient age, vascular tortuosity and atheromatous change are increasing. Transradial approach is very useful in patients with significant tortuosity or ectatic changes of the aortic arch, and in patients with acute right vertebral artery course from the subclavian artery12). In some patients with very tortuous supra-aortic branches or bovine type left CCA, it is necessary to exchange Simmons or other specialized catheters for transfemoral access. However, transradial approach allow easy catheterization without exchanging the catheter. Additionally, it is more suitable in the right vertebral and right carotid systems. At times, the right vertebral artery is extremely difficult to catheterize from a transfemoral approach. In this condition, the right vertebral artery is easily catheterized from the transradial approach. Stability of guiding catheters in the right vertebral and carotid systems is outstanding from a transradial approach17). Catheter stability is excellent because the catheter system is confined to vessels with relatively small diameters, whereas guiding-catheter instability from a transfemoral approach often occurs because of transverse ectatic and large-diameter aortic arches17).
Transradial cerebral angiography has some limitations. The success rate of selective catheterization is relatively low, especially for the left vertebral and internal carotid artery12). However, it is not a severe problem in vascular evaluation, because in most cases the target vessels were successfully visualized with the left common carotid artery injection and the left subclavian artery and/or the right vertebral artery injection. In our institution, to avoid vessel wall damage in the vertebral artery, we placed the catheter tip just to the orifice or the proximal portion of the vertebral artery. Otherwise, we prefer the transfemoral approach if the left vertebral artery is absolutely necessary to evaluate.
As a transradial approach is technically somewhat difficult and more challenging, it has a steep and significant learning curve to increase the success rate. It is difficult to negotiate the wire into the aortic arch, because the vessels originating from the arch become tortuous with advancing age. Additionally, potential trauma to the radial artery is more likely to occur in elderly patients, in whom the radial artery may be quite tortuous13). The success rate of transradial cerebral angiography is reported to be 92.7-99%6,10,13,15,19). Hildick-Smith et al.5) have reported that the success rate of a transradial approach ranged from 88% for beginners to 94% for experienced specialists. In our series, the success rate was 92.2% in elderly patients (>60 years old). We failed in 4 patients; two had loop formations of the radial artery, and two experienced severe vasospasm due to multiple puncture failures (Fig. 1). Some authors worry about procedure-related thromboembolism with a reversed-angle catheter such as Simmons12). They suggest that the whirling motion of the bulky catheter within a tortuous atheromatous aorta is dangerous. We had one patient who experienced intraprocedural thrombosis. However, this complication rate is comparable with that of transfemoral access4,12). It is important that there is gentle catheter manipulation in the aortic arch to reduce the chance of disturbing atheromatous plaques.
CONCLUSION
Transradial cerebral angiography is a useful routine or alternative method for patients in whom transfemoral cerebral angiography is less favorable. With advancing patient age, transradial angiography is helpful to overcome vessel tortuosity and patient discomfort.
Acknowledgements
I thank our members of the cerebral angiographic suite, Young-Chool Min and Young-Tak Jung for the procedural assistant, and Yoon-Kyung Ha for data record and collection. This study was supported by a grant from Kosin University College of Medicine in 2012.
References
- 1.Bendok BR, Przybylo JH, Parkinson R, Hu Y, Awad IA, Batjer HH. Neuroendovascular interventions for intracranial posterior circulation disease via the transradial approach : technical case report. Neurosurgery. 2005;56:E626. doi: 10.1227/01.NEU.0000154820.28342.38. discussion E626. [DOI] [PubMed] [Google Scholar]
- 2.Campeau L. Percutaneous radial artery approach for coronary angiography. Cathet Cardiovasc Diagn. 1989;16:3–7. doi: 10.1002/ccd.1810160103. [DOI] [PubMed] [Google Scholar]
- 3.Fessler RD, Wakhloo AK, Lanzino G, Guterman LR, Hopkins LN. Transradial approach for vertebral artery stenting : technical case report. Neurosurgery. 2000;46:1524–1527. doi: 10.1097/00006123-200006000-00044. discussion 1527-1528. [DOI] [PubMed] [Google Scholar]
- 4.Heiserman JE, Dean BL, Hodak JA, Flom RA, Bird CR, Drayer BP, et al. Neurologic complications of cerebral angiography. AJNR Am J Neuroradiol. 1994;15:1401–1407. discussion 1408-1411. [PMC free article] [PubMed] [Google Scholar]
- 5.Hildick-Smith DJ, Walsh JT, Lowe MD, Shapiro LM, Petch MC. Transradial coronary angiography in patients with contraindications to the femoral approach : an analysis of 500 cases. Catheter Cardiovasc Interv. 2004;61:60–66. doi: 10.1002/ccd.10708. [DOI] [PubMed] [Google Scholar]
- 6.Iwasaki S, Yokoyama K, Takayama K, Ueda K, Sueyosi S, Nagasawa M, et al. The transradial approach for selective carotid and vertebral angiography. Acta Radiol. 2002;43:549–555. doi: 10.1080/j.1600-0455.2002.430601.x. [DOI] [PubMed] [Google Scholar]
- 7.Jo KW, Park SM, Kim SD, Kim SR, Baik MW, Kim YW. Is Transradial Cerebral Angiography Feasible and Safe? A Single Center's Experience. J Korean Neurosurg Soc. 2010;47:332–337. doi: 10.3340/jkns.2010.47.5.332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kiemeneij F, Laarman GJ. Transradial artery Palmaz-Schatz coronary stent implantation : results of a single-center feasibility study. Am Heart J. 1995;130:14–21. doi: 10.1016/0002-8703(95)90229-5. [DOI] [PubMed] [Google Scholar]
- 9.Kiemeneij F, Laarman GJ, Odekerken D, Slagboom T, van der Wieken R. A randomized comparison of percutaneous transluminal coronary angioplasty by the radial, brachial and femoral approaches : the access study. J Am Coll Cardiol. 1997;29:1269–1275. doi: 10.1016/s0735-1097(97)00064-8. [DOI] [PubMed] [Google Scholar]
- 10.Kim JH, Park YS, Chung CG, Park KS, Chung DJ, Kim HJ. Feasibility and utility of transradial cerebral angiography : experience during the learning period. Korean J Radiol. 2006;7:7–13. doi: 10.3348/kjr.2006.7.1.7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Laarman G, Muthusamy TS, Swart H, Westendorp I, Kiemeneij F, Slagboom T, et al. Direct coronary stent implantation : safety, feasibility, and predictors of success of the strategy of direct coronary stent implantation. Catheter Cardiovasc Interv. 2001;52:443–448. doi: 10.1002/ccd.1099. [DOI] [PubMed] [Google Scholar]
- 12.Lee DH, Ahn JH, Jeong SS, Eo KS, Park MS. Routine transradial access for conventional cerebral angiography : a single operator's experience of its feasibility and safety. Br J Radiol. 2004;77:831–838. doi: 10.1259/bjr/89933527. [DOI] [PubMed] [Google Scholar]
- 13.Levy EI, Boulos AS, Fessler RD, Bendok BR, Ringer AJ, Kim SH, et al. Transradial cerebral angiography : an alternative route. Neurosurgery. 2002;51:335–340. discussion 340-342. [PubMed] [Google Scholar]
- 14.Matsumoto Y, Hokama M, Nagashima H, Orz Y, Toriyama T, Hongo K, et al. Transradial approach for selective cerebral angiography : technical note. Neurol Res. 2000;22:605–608. doi: 10.1080/01616412.2000.11740727. [DOI] [PubMed] [Google Scholar]
- 15.Matsumoto Y, Hongo K, Toriyama T, Nagashima H, Kobayashi S. Transradial approach for diagnostic selective cerebral angiography : results of a consecutive series of 166 cases. AJNR Am J Neuroradiol. 2001;22:704–708. [PMC free article] [PubMed] [Google Scholar]
- 16.Moran CJ, Milburn JM, Cross DT, 3rd, Derdeyn CP, Dobbie TK, Littenberg B. Randomized controlled trial of sheaths in diagnostic neuroangiography. Radiology. 2001;218:183–187. doi: 10.1148/radiology.218.1.r01ja05183. [DOI] [PubMed] [Google Scholar]
- 17.Nohara AM, Kallmes DF. Transradial cerebral angiography : technique and outcomes. AJNR Am J Neuroradiol. 2003;24:1247–1250. [PMC free article] [PubMed] [Google Scholar]
- 18.Park SH, Park JC, Hwang JH, Hwang SK, Hamm IS. Role of three-dimensional computed tomography angiography in the follow-up of patients with aneurysm clips. J Korean Neurosurg Soc. 2006;39:427–431. [Google Scholar]
- 19.Wu CJ, Hung WC, Chen SM, Yang CH, Chen CJ, Cheng CI, et al. Feasibility and safety of transradial artery approach for selective cerebral angiography. Catheter Cardiovasc Interv. 2005;66:21–26. doi: 10.1002/ccd.20396. [DOI] [PubMed] [Google Scholar]