

Abstract
Objective:
Analysis of shaping ability of four different rotary endodontic instruments using spiral computed tomography (CT).
Materials and Methods:
Eighty freshly extracted human mandibular first molars were used in the present study. Samples were randomly divided into four experimental groups with twenty samples in each group. Images of mesiobuccal canal of each sample were obtained pre- and post-operatively using spiral CT. All samples were prepared using their respective endodontic file systems (group I - ProTaper, group II - K3, group III - RaCe, and group IV - Mtwo). Image analyses were done using image analysis software for evaluation of canal transportation and centering ability. Data was then statistically analyzed using analysis of variance.
Results:
There was no statistically significance in transportation in their intergroup difference at any of the three locations (coronal, middle, and apical third). In centering ability there was no statistically significance in the coronal and middle third of the intergroup. However, there was a statistically significance of (P = 0.044) at the apical third between all the groups.
Conclusion:
Canals prepared with ProTaper had more canal transportation at all the three levels of root canal (coronal, middle, and apical third). Canals prepared with Mtwo were well centered at coronal and middle third whereas with RaCe canals were centered only at the apical third. All instruments showed some degree of canal aberrations in terms of shaping ability.
Keywords: K3, Mtwo, ProTaper, RaCe, shaping ability, spiral computed tomography
INTRODUCTION
The main objective of the instrumentation phase of root canal therapy is to remove all pulpal tissue and debris from the canal and to prepare the canal three dimensionally for the desired filling material. Sufficient enlargement to remove contaminated dentin while preparing the apical portion should be round in cross-section and a smooth tapering preparation is a must for close adaptation of the master cone to the canal walls is recommended.[1] Schilder[2] in 1974 stated cleaning and shaping as the foundation for successful endodontic therapy.
However, shaping of curved canals has been offset by a tendency for all preparation techniques to deviate the prepared canal from its original axis. Deviation from the original curvature can lead to excessive or inappropriate dentine removal, straightening of the canal and creation of a ledge in the dentinal wall, a biomechanical defect known as elbow, which forms the coronal to the elliptical-shaped apical seal, canals with hourglass appearance in cross-section, which requires stripping and over-preparation that weakens the tooth, resulting in fracture of the root.[3]
Several instrument systems have been introduced in the past with different features. ProTaper rotary instruments (Dentsply Maillefer, Ballagigues, Switzerland) features a variable taper over the length of its cutting blades and also a convex, triangular cross-section, a changing helical angle and pitch over the cutting blades and a non-cutting, modified guiding tip. It consists of three shaping and finishing instruments.[4] The K3 (Sybron Endo, Orange, CA) with its innovative design, and the ability to prepare the canal without threading, offers minimal resistance to torsional and cyclic fatigue. It has a wide range of sizes that allow optimal flexibility.[5] RaCe (FKG Dentaire, Switzerland), a fixed taper rotary endodontic file system which has a triangular cross section and comes with two alternating cutting edges enabling it with optimum efficiency and circumventing the screw-in effect.[5] Mtwo (VDW, Munich, Germany), an endodontic rotary file system incorporates a variable pitch and steep helical angle comes in various fixed tapers. Its S-shaped cross section with no radial lands and minimal core width renders it with an optimal cutting and shaping efficiency.[6]
For assessment of canal instrumentation, methods such as scanning electron microscope, radiographic evaluation, photographic assessment and computer manipulation for comparative analysis have been used in the past. The methods are invasive in nature; hence accurate repositioning of pre- and post-instrumented specimens is difficult. They are labor intensive, and has the disadvantage of loss of the specimen.[7]
Computed tomography (CT), a non-destructive technology has been advocated for pre-and post-instrumentation evaluation of canal. It can render cross-sectional (cut plane) and 3D images that are highly accurate and quantifiable.[8] Comparisons using CT have provided repeatable results and also have allowed non-invasive experimentation of various aspects of endodontic instrumentation. At any level, the amount and direction of canal transportation can be viewed without loss of specimen.[8,9]
The purpose of this ex vivo study was to compare and evaluate the shaping ability of four different rotary endodontic file systems using CT.
MATERIALS AND METHODS
A total of 80 extracted mandibular first molars with mesiobuccal root curvatures ranging between 20° and 40° having no cracks or anomalies were collected and stored in formalin. The storage and handling of the teeth were performed as per Occupational Safety and Health Administration (OSHA) and Centers for Disease Control and Prevention (CDC) guidelines. The mesiobuccal canal of all the samples was standardized to 9 mm length by de-coronation using a diamond disc.
The prepared samples were randomly divided into four experimental groups (group I - ProTaper, group II - K3, group III - RaCe and group IV - Mtwo) with twenty samples in each group.
Scanning and imaging
All the groups were scanned using Spiral CT (Siemens Emotion 6 slice CT scanner) pre-operatively before instrumentation. The CT scans were done using the inner ear protocol supplied by the CT scanner, at 130 KV and 130 mA, 512 × 512 pixels matrix, 1-mm-thick axial sections, 32 cm display field of view, and beam incidence at the central portion on the device used to fix the specimens. Three levels each at 3 mm were chosen for evaluation in the CT. The images were stored in the computer's hard disk for further comparison between pre- instrumentation and post-instrumentation data by using DiCom software.
Root canal instrumentation
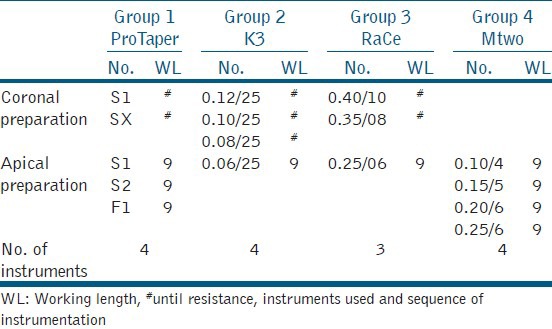
Mesiobuccal canal of all the samples were prepared using their respective endodontic rotary file as described in Table 1.
Table 1.
Instruments used and sequence of instrumentation
Evaluation
The shaping ability of the instruments were assessed for cross-sectional (transportation and centering ability) changes using the computer program UTHSCSA ImageTool Version 3.0 in all the three levels of each sample.
Evaluation of canal transportation
To compare the degree of canal transportation, a technique developed by Bergmans et al.[10] was used [Figures 1 and 2].
Figure 1.
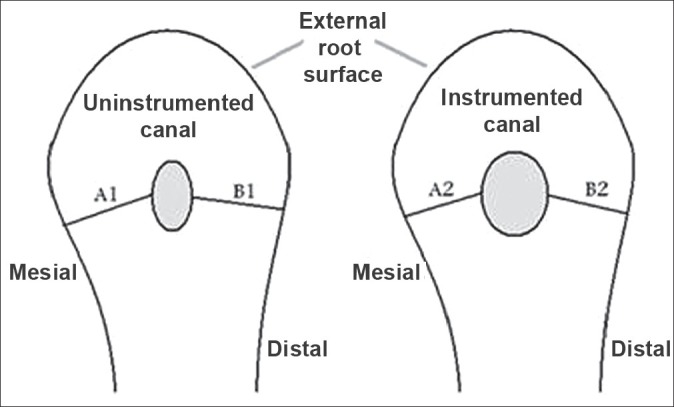
The amount of canal transportation was determined by measuring the shortest distance from the edge of un-instrumented canal to the periphery of the root (mesial and distal) and then comparing this with the same measurements obtained from the instrumented images
Figure 2.
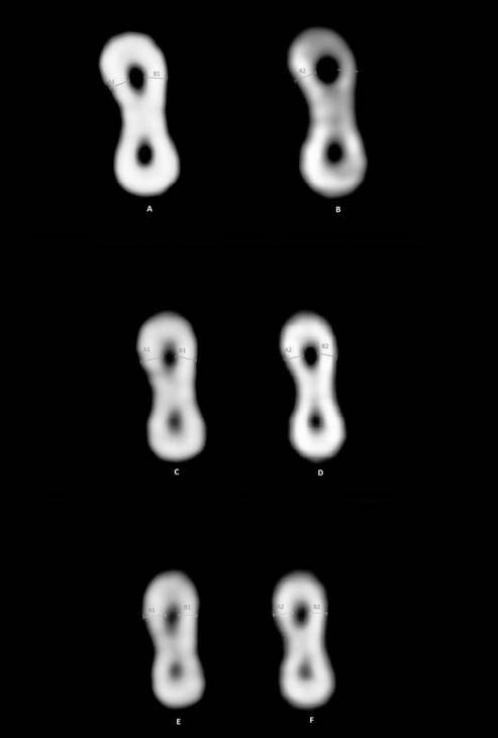
Pre- and post-operative computed tomography images of coronal, middle, and apical third
Transportation in each part of all samples in all the groups was calculated using the following formula:
{(A1–A2)−(B1–B2)}
According to this formula, a result of ‘0’ indicates no canal transportation. Results other than ‘0’ means transportation has occurred in the canal.
Evaluation of centering ability
According to Gambill et al.[7] “the mean centering ratio” indicates the ability of the instrument to stay centered in the canal.
This ratio was calculated in each part of all samples in all the groups using the following ratio:
(A1 − A2)/(B1 − B2)
Or
(B1 − B2)/A1 − A2)
If these numbers are not equal, the lower figure is considered the numerator of the ratio. According to this formula, a result of ‘1’ indicates perfect centering.
Analysis of data
All data were recorded and stored in a personal computer. The data were analyzed using analysis of variance (ANOVA) (two-way ANOVA). The post-hoc Tukey HSD test was used for group-wise comparison. The statistical analysis was done with Statistical Package for Social Sciences Version 15.0 (SPSS Inc, USA) statistical analysis software.
RESULTS
Transportation
Mean transportation at coronal, middle and apical levels in four groups under study are shown in Table 2. At coronal level, maximum mean value was obtained for ProTaper (0.21 ± 0.17) while minimum value was obtained for K3 (0.15 ± 0.11).
Table 2.
Mean transportation at coronal, middle, and apical levels in four groups under study (mm)
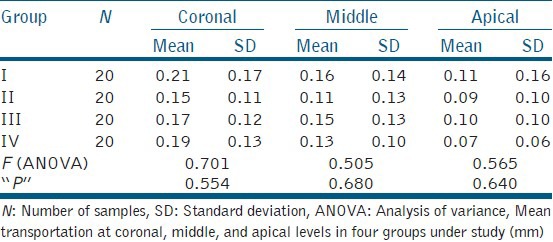
At middle level, maximum mean value was obtained for ProTaper (0.16 ± 0.14) while minimum value was obtained for K3 (0.11 ± 0.13 mm).
At apical level, maximum mean value was obtained for ProTaper (0.11 ± 0.16) whereas, minimum value was obtained for Mtwo (0.07 ± 0.06).
ANOVA did not reveal a statistically significant intergroup difference at any of the three locations.
Centering ability
Centering ability (ratio) for all the four groups under study is shown in Table 3. At coronal level, maximum mean value was obtained for ProTaper (0.59 ± 0.32) while minimum value was obtained for Mtwo (0.46 ± 0.28).
Table 3.
Mean centering (ratio) at coronal, middle and apical levels in four groups under study
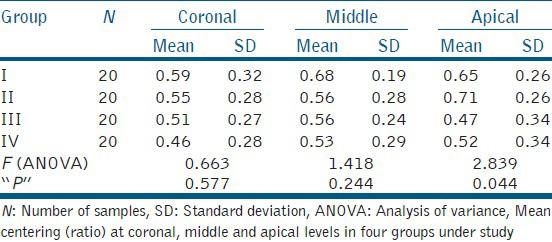
At middle level, maximum mean value was obtained for ProTaper (0.68 ± 0.19) while minimum was obtained for Mtwo (0.53 ± 0.29).
At apical level, maximum mean value was obtained for K3 (0.71 ± 0.26) whereas minimum value was obtained for RaCe (0.47 ± 0.34).
ANOVA did not reveal a statistically significant intergroup difference at coronal and middle thirds, however, at apical third the intergroup difference was statistically significant (P = 0.044) between all the groups.
DISCUSSION
Nickel titanium rotary instrumentation was introduced in the early 1990s, since then many different instrument systems have been manufactured. NiTi alloys overall are softer than stainless steel, are not heat treatable, have a low modulus of elasticity (about one-fourth to one-fifth that of stainless steel) but a greater strength, are tougher and more resilient, and show shape memory and superelasticity. NiTi instruments have superior ability to remain centered within the canal during instrumentation compared to stainless steel files thus minimizing the straightening of the canal.[11] These properties are the main reasons why NiTi alloys have succeeded in endodontics and some other dental disciplines.[12]
In the present study, canals prepared with ProTaper showed maximum value for root canal transportation at all the three levels which may be attributed to the progressive taper along the cutting surface and reduction in instrument flexibility. The results are obtained in conformity to Javaheri and Javaheri,[13] who found protaper to produce more apical transportation than any other instrument. Guelzow et al.[14] compared the effects of six rotary NiTi systems (FlexMaster, System GT, Hero 642, K3, ProTaper, RaCe) and hand filing for root canal preparation. They found ProTaper to show the highest degree of straightening. The results are also in accordance to Bonaccorso et al.[15] who found ProTaper instruments to cause more pronounced canal transportation among ProTaper, Mtwo, BioRaCe, and BioRaCe + S-Apex instruments.
Minimum canal transportation was observed with K3 in the coronal and middle thirds, its unique cross section design, which has a positive angle of inclination, relief at the posterior extremity of the blade, U-shaped file design with three radial lands and the relatively higher number of instruments used in the shaping sequences may be responsible for the above observation.[16] Ersev et al.[17] evaluated the shaping efficacy of five NiTi rotary instruments with different cross-sectional designs, they found K3 to be a better choice in preparing curved canals.
Al-Sudani and Al-Shahrani,[18] compared the canal centering ability of ProFile, K3, and RaCe nickel titanium rotary systems and found the ProFile system produced significantly least transportation followed by the K3 system, and the RaCe system produced significantly a higher transportation. In the present study, Mtwo showed lowest value for canal transportation, Mtwo instruments with double cutting-edge geometry have unequal cross-section areas, which increases their flexibility.[19,20] The results are in conformity to Yang et al.[21] who also found Mtwo to produce lesser canal transportation than ProTaper.
In the analysis of centering ability, low value indicated that the preparation was centered in the canal,[22] the results of the present study showed Mtwo to be better centered in the coronal and middle third while ProTaper showed least centered preparation at the above mentioned levels. These differences could be attributed to different instrumentation techniques. All other systems instrument the canals with crown down technique, but Mtwo prepare the canals with step back technique. Other reasons for this difference might be, that Mtwo sequence has fewer instruments and has a brushing action on the canal walls, the observations are in confirmation to Veltri et al.[22] and Schafer et al.[23] The least centered preparation with ProTaper could be due to its reduced flexibility, increased tip stiffness and progressive taper of the instrument as compared to fixed tapers of others. The results are in accordance to Gergi et al.[24] and Schafer and Vlassis.[25]
In the apical third, RaCe prepared better centered canals while K3 showed least centering ability. RaCe with a short, twisted, alternating cutting edge and the smallest taper at the apical part may be a contributing factor, the results are in conformity to studies done by Paque et al.[26] and Pasternak-Junior et al.[27] The reason behind K3 showing least centering ability might be due to its 45° positive rake angle, instrument having positive rake angle will work like a shaver on the dentin surface, the cross section area of K3 is nearly twice that of RaCe with the same tip size and taper.[28] The results are in accordance to Venkateshbabu et al.[29] and Sudani and Shahrani.[18]
CONCLUSION
Within the limitation of this study, canals prepared with ProTaper had more canal transportation at all the three levels of root canal. Better centered canals were prepared with Mtwo at the coronal and middle third, canals prepared with RaCe were better centered at the apical third. All instruments showed some degree of aberrations in terms of shaping ability.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Jungmann CL, Uchin RA, Bucher JF. Effect of instrumentation on the shape of the root canal. J Endod. 1975;1:66–9. doi: 10.1016/S0099-2399(75)80083-5. [DOI] [PubMed] [Google Scholar]
- 2.Schilder H. Cleaning and shaping the root canal. Dent Clin North Am. 1974;18:269–96. [PubMed] [Google Scholar]
- 3.Kandaswamy D, Venkateshbabu N, Porkodi I, Pradeep G. Canal-centering ability: An endodontic challenge. J Conserv Dent. 2009;12:3–9. doi: 10.4103/0972-0707.53334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ruddle CJ. The ProTaper technique. Endod Top. 2005;10:187–90. [Google Scholar]
- 5.Gianluca G. The K3 rotary nickel titanium instrument system. Endod Top. 2005;10:179–82. [Google Scholar]
- 6.Bonaccorso A, Cantatore G, Condorelli GG, Schäfer E, Tripi TR. Shaping ability of four nickel-titanium rotary instruments in simulated S-shaped canals. J Endod. 2009;35:883–6. doi: 10.1016/j.joen.2009.03.007. [DOI] [PubMed] [Google Scholar]
- 7.Gambill JM, Alder M, del Rio CE. Comparison of nickel-titanium and stainless steel hand-file instrumentation using computed tomography. J Endod. 1996;22:369–75. doi: 10.1016/S0099-2399(96)80221-4. [DOI] [PubMed] [Google Scholar]
- 8.Gluskin AH, Brown DC, Buchanan LS. A reconstructed computerized tomographic comparison of Ni-Ti rotary GT files versus traditional instruments in canals shaped by novice operators. Int Endod J. 2001;34:476–84. doi: 10.1046/j.1365-2591.2001.00422.x. [DOI] [PubMed] [Google Scholar]
- 9.Garip Y, Günday M. The use of computed tomography when comparing nickel-titanium and stainless steel files during preparation of simulated curved canals. Int Endod J. 2001;34:452–7. doi: 10.1046/j.1365-2591.2001.00416.x. [DOI] [PubMed] [Google Scholar]
- 10.Bergmans L, Van Cleynenbreugel J, Beullens M, Wevers M, Van Meerbeek B, Lambrechts P. Progressive versus constant tapered shaft design using NiTi rotary instruments. Int Endod J. 2003;36:288–95. doi: 10.1046/j.1365-2591.2003.00650.x. [DOI] [PubMed] [Google Scholar]
- 11.Khurana P, Nainan MT, Sodhi KK, Padda BK. Change of working length in curved molar root canals after preparation with different rotary nickel-titanium instruments. J Conserv Dent. 2011;14:264–8. doi: 10.4103/0972-0707.85809. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Baumann MA. Nickel-titanium: Options and challenges. Dent Clin North Am. 2004;48:55–67. doi: 10.1016/j.cden.2003.11.001. [DOI] [PubMed] [Google Scholar]
- 13.Turpin YL, Chagneau F, Vulcain JM. Impact of two theoretical cross-sections on torsional and bending stresses of nickel-titanium root canal instrument models. J Endod. 2000;26:414–7. doi: 10.1097/00004770-200007000-00009. [DOI] [PubMed] [Google Scholar]
- 14.Guelzow A, Stamm O, Martus P, Kielbassa AM. Comparative study of six rotary nickel-titanium systems and hand instrumentation for root canal preparation. Int Endod J. 2005;38:743–52. doi: 10.1111/j.1365-2591.2005.01010.x. [DOI] [PubMed] [Google Scholar]
- 15.Bonaccorso A, Cantatore G, Condorelli GG, Schäfer E, Tripi TR. Shaping ability of four nickel-titanium rotary instruments in simulated S-shaped canals. J Endod. 2009;35:883–6. doi: 10.1016/j.joen.2009.03.007. [DOI] [PubMed] [Google Scholar]
- 16.Cecchin D, de Sousa-Neto MD, Pécora JD, Gariba-Silva R. Cutting efficiency of four different rotary nickel: Titanium instruments. J Conserv Dent. 2011;14:117–9. doi: 10.4103/0972-0707.82605. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Ersev H, Yilmaz B, Ciftçioğlu E, Ozkarsli SF. A comparison of the shaping effects of 5 nickel-titanium rotary instruments in simulated S-shaped canals. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;109:e86–93. doi: 10.1016/j.tripleo.2009.12.033. [DOI] [PubMed] [Google Scholar]
- 18.Al-Sudani D, Al-Shahrani S. A comparison of the canal centering ability of ProFile, K3, and RaCe Nickel Titanium rotary systems. J Endod. 2006;32:1198–201. doi: 10.1016/j.joen.2006.07.017. [DOI] [PubMed] [Google Scholar]
- 19.Dobó-Nagy C, Serbán T, Szabó J, Nagy G, Madléna M. A comparison of the shaping characteristics of two nickel-titanium endodontic hand instruments. Int Endod J. 2002;35:283–8. doi: 10.1046/j.1365-2591.2002.00492.x. [DOI] [PubMed] [Google Scholar]
- 20.Yum J, Cheung GS, Park JK, Hur B, Kim HC. Torsional strength and toughness of nickel-titanium rotary files. J Endod. 2011;37:382–6. doi: 10.1016/j.joen.2010.11.028. [DOI] [PubMed] [Google Scholar]
- 21.Yang G, Yuan G, Yun X, Zhou X, Liu B, Wu H. Effects of two nickel-titanium instrument systems, Mtwo versus ProTaper universal, on root canal geometry assessed by micro-computed tomography. J Endod. 2011;37:1412–6. doi: 10.1016/j.joen.2011.06.024. [DOI] [PubMed] [Google Scholar]
- 22.Veltri M, Mollo A, Mantovani L, Pini P, Balleri P, Grandini S. A comparative study of Endoflare-Hero Shaper and Mtwo NiTi instruments in the preparation of curved root canals. Int Endod J. 2005;38:610–6. doi: 10.1111/j.1365-2591.2005.00989.x. [DOI] [PubMed] [Google Scholar]
- 23.Schäfer E, Erler M, Dammaschke T. Comparative study on the shaping ability and cleaning efficiency of rotary Mtwo instruments. Part 1. Shaping ability in simulated curved canals. Int Endod J. 2006;39:196–202. doi: 10.1111/j.1365-2591.2006.01074.x. [DOI] [PubMed] [Google Scholar]
- 24.Gergi R, Rjeily JA, Sader J, Naaman A. Comparison of canal transportation and centering ability of twisted files, Pathfile-ProTaper system, and stainless steel hand K-files by using computed tomography. J Endod. 2010;36:904–7. doi: 10.1016/j.joen.2009.12.038. [DOI] [PubMed] [Google Scholar]
- 25.Schäfer E, Vlassis M. Comparative investigation of two rotary nickel-titanium instruments: ProTaper versus RaCe. Part 1. Shaping ability in simulated curved canals. Int Endod J. 2004;37:229–38. doi: 10.1111/j.0143-2885.2004.00786.x. [DOI] [PubMed] [Google Scholar]
- 26.Paqué F, Musch U, Hülsmann M. Comparison of root canal preparation using RaCe and ProTaper rotary Ni-Ti instruments. Int Endod J. 2005;38:8–16. doi: 10.1111/j.1365-2591.2004.00889.x. [DOI] [PubMed] [Google Scholar]
- 27.Pasternak-Júnior B, Sousa-Neto MD, Silva RG. Canal transportation and centring ability of RaCe rotary instruments. Int Endod J. 2009;42:499–506. doi: 10.1111/j.1365-2591.2008.01536.x. [DOI] [PubMed] [Google Scholar]
- 28.Schäfer E, Dzepina A, Danesh G. Bending properties of rotary nickel-titanium instruments. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;96:757–63. doi: 10.1016/s1079-2104(03)00358-5. [DOI] [PubMed] [Google Scholar]
- 29.Venkateshbabu N, Emmanuel S, Santosh GK, Kandaswamy D. Comparison of the canal centring ability of K3, Liberator and EZ Fill Safesiders by using spiral computed tomography. Aust Endod J. 2012;38:55–9. doi: 10.1111/j.1747-4477.2009.00210.x. [DOI] [PubMed] [Google Scholar]