

Abstract
Aim:
To compare the polymerization efficacy of micro-hybrid and nanocomposites cured with Quartz-tungsten halogen (QTH) and light emitting diode (LED) light curing units (LCUs). The effectiveness of pulse cure mode in LED LCU was also investigated.
Materials and Methods:
Both micro-hybrid and nanocomposite specimens were cured using four different curing protocols giving a total of eight experimental groups. Ten cylindrical specimens were prepared for each group, and light cured for 40 s on the top surface, thus giving a total of eighty specimens. Vicker hardness measurements were carried out on the top and bottom surfaces after 24 h and hardness ratio was calculated.
Results:
For both micro-hybrid and nanocomposites, highest mean VHN was observed for the group cured with QTH LCU, and the lowest was observed for the group cured with second LED LCU in standard mode but the difference was significant only in case of nanocomposite.
Conclusion:
Curing nanocomposites with QTH LCU results in better micro hardness. Pulse cure mode does not effectively increase polymerization efficacy than the standard mode of curing.
Keywords: Curing lights, hardness, nanocomposite
INTRODUCTION
Clinical longevity of light cure resin composites used for restoration of both anterior and posterior teeth has been studied extensively.[1] Adequate curing of resin composites is important as it influences its mechanical properties, prevents bulk, or marginal fracture, adverse tissue reactions, and secondary caries. Traditionally, halogen based curing lamps, which use filters to restrict the emitted light to blue region of the spectrum for polymerization have been used to activate the photo initiator system in the composites.[2] However, they have several drawbacks such as overheating of the incandescence lamp, limited effective lifetime of the halogen bulbs, and degradation of internal components (bulb, reflector, and filter) overtime.[2,3] To overcome these drawbacks, blue light emitting diode (LED), light curing units (LCU) have been developed. These are solid state semiconductor devices that convert electrical energy directly to light. LED's have lifetimes of more than 10,000 h and undergo little degradation of light output over time.[4] In order to minimize polymerization shrinkage of composites without affecting the degree of conversion, various polymerization modes have been formulated, such as soft start, pulse delay, pulse cure, and ramp mode.[5]
A continued development in composite resins resulted in materials with reduced particle size and increased filler loading, significantly improving the universal applicability of light-cured composite resins.[6,7] Micro-hybrid composites are a combination of micro fill and larger filler particles with an average size of 0.01-0.1 μm. These have the advantage of improved physical properties, high percent fill and excellent aesthetics. The main drawback of this group, as determined by larger particle size, is the difficulty in maintaining long-term high polish.[8] To overcome this, nano-filled composites, which have nanomeric particles and nanoclusters in a conventional resin matrix were introduced.[7]
Several studies have compared the efficacy of quartz-tungsten halogen (QTH) LCU with LED LCU using micro fill, hybrid, and micro-hybrid composite resins.[4,9,10,11] The curing efficacy of recently developed nanocomposites, which have different optical properties have not been studied extensively with different curing modes of LED units. Hence, this study was undertaken to compare the efficacy of polymerization of micro-hybrid and nanocomposites cured with QTH, and LED LCUs by hardness testing method. The effectiveness of cure of pulse cure mode in LED LCU was also investigated. The null hypothesis tested was that there is no difference in the Vicker hardness of micro-hybrid and nanocomposite cured with QTH LCU, standard regimens of two LED LCUs, and pulse cure mode of LED LCU at top and bottom surfaces of composite specimens respectively. In addition, the depth of cure of the composites cured with QTH and LED LCU was determined.
MATERIALS AND METHODS
Two light cured resin based composites, nano-composite (Z350, 3M™ ESPE™ dental products, St. Paul, USA; A2 shade), and micro-hybrid composite (Z100, 3M ESPE dental products, St. Paul, USA; A2 shade), were used in this study. These were cured with QTH LCU (Elipar 2500, 3M ESPE dental products, St. Paul, MN, USA), and 2 LED LCUs (Smartlite™ PS, Pen Style High Power LED Curing Light, Dentsply Caulk, Dentsply, Milford, and Ulight™ PB-070 LED Curing Light, Fine Vision Electronics Co. Ltd. [FVE, Taiwan]; designated as first LED and second LED respectively). The two LED LCUs differed in their spectrum range (450-490 nm and 440-480 nm respectively) and curing modes. The first LED was curable only in standard mode whereas the second LED was curable in fast, ramp, and pulse mode as well as standard mode. Each composite type was cured using four different curing protocols giving a total of eight experimental groups:
Group 1: Nanocomposite cured with QTH LCU
Group 2: Nanocomposite cured with first LED LCU in standard mode
Group 3: Nanocomposite cured with second LED LCU in standard mode
Group 4: Nanocomposite cured with second LED LCU in pulse cure mode
Group 5: Micro-hybrid composite cured with QTH LCU
Group 6: Micro-hybrid composite cured with first LED LCU in standard mode
Group 7: Micro-hybrid composite cured with second LED LCU in standard mode
Group 8: Micro-hybrid composite cured with second LED LCU in pulse cure mode
Method for assessing the effectiveness of cure was in accordance with that used by Yap.[12] Ten disk shaped specimens in each group were formed, giving a total sample size of eighty. The discs were prepared using the Teflon mould (Dentsply, Milford) measuring 5 mm in diameter and 2 mm in thickness.
The moulds were placed on flat glass plates on top of acetate strips and then filled with resin based composites using cement carrier and condenser. The resin was covered with another acetate strip and gently pressed with another glass plate against the mould to extrude excess material and to ensure a level of the plane on the top and bottom surfaces. The excess material was removed using an explorer. New, clean acetate strips was used for each specimen.
All the specimens were then irradiated by touching the LCU guide on the top acetate strip for 40 s using the respective LCUs. The LED's were charged according to manufacturer's recommendations, and placed back in their battery chargers after each specimen was polymerized. The light intensity of all the curing lights were checked with a radiometer (Demetron 100, Demetron Research Corp, USA.), prior to use, to ensure consistency in intensity output from the light source. All the LCUs used in the study had intensity readings above 300 mW/cm2, which is the minimum required intensity for complete polymerization.[13]
The top surface was identified with an indelible marker. The specimens were then stored in a light proof container in distilled water at 37±C for 24 h prior to microhardness testing. The specimens were stored in eight different coded containers. The specimens were blotted dry prior to microhardness testing.
The Vickers hardness measurements were carried out under a load of 50 g for 15 s using a Vicker Hardness Tester (Model – Micro Vickers (MV) 1-PC (Personal computer based) (FIE) Fuel Instruments and Engineers Private Limited™. All the measurements were carried out by a single trained independent examiner. The mean Vickers hardness number (VHN) of the top and bottom surfaces was calculated. To determine the depth of cure, the hardness ratio was calculated by dividing the bottom surface VHN by the top surface VHN. Data was analyzed using SPSS (Statistical Package for Social Sciences) for Windows release 11.5 (SPSS, Chicago, IL, USA). One-way ANOVA was used to find the differences between the groups and Tukey Honestly significant difference post hoc test, for intergroup comparisons.
RESULTS
Table 1 shows the mean VHN values and hardness ratio of all the groups. The highest mean hardness value of both the top and bottom surface was observed for Group 1 and the lowest mean was observed for Group 3. One-way ANOVA revealed significant difference in the mean hardness values of the top surface (P = 0.002), but no significant difference was seen in the bottom surface. When comparing the mean values of the hardness ratio, it was seen that all the groups scored higher than 0.80 indicating adequate depth of cure, and the difference between the hardness ratios were not significant.
Table 1.
Mean and standard deviation of Vicker hardness measurements and hardness ratio
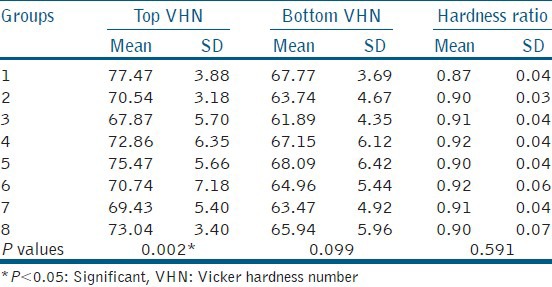
For both nanocomposites, (Group 1-4) and micro-hybrid composite resins (Group 5-8), the highest mean hardness values for both the top and bottom surfaces were for the ones cured with QTH LCU and the lowest mean hardness values were observed for the ones cured with second LED LCU using standard mode. One-way ANOVA showed that the mean VHN of both the top and bottom surfaces of nanocomposite specimens cured with QTH LCU was significantly higher (P = 0.001 and 0.028 respectively), but not for micro-hybrid composite.
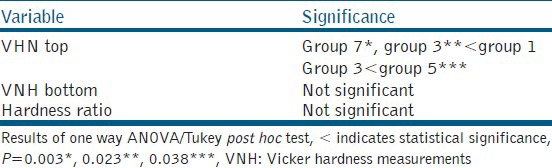
Table 2 shows the intergroup comparison of all the eight groups. There was a statistically significant difference between the groups cured with QTH LCU and the second LED LCU in standard mode irrespective of the composite resin type used. No statistical significant difference was found among the other groups.
Table 2.
Intergroup comparison of mean Vicker hardness measurements values
DISCUSSION
Several methodologies have been proposed to evaluate the polymerization efficacy of LCUs. Hardness testing, an indirect method, is a good indicator of the degree of conversion, and VHN exhibits a good correlation with infrared spectroscopy, a direct method.[3] In this study, Vickers hardness test was used to characterize the hardness of materials.
Various factors affect polymerization and depth of cure of resin composites. These are the effectiveness of light transmission (light tips being free from scratches and debris), thickness, and shade of restorative material, exposure time, distance of the light source from the restorative material, and light intensity.[14] To minimize the effects of colorants on light polymerization, A2 shade of both the composite resins was used. As light intensity decreases with increasing distance from the light cure tip, the light cure tip was kept touching the acetate strip to standardize the procedure.[15] Curing time was limited to 40 s as per the manufacturer's recommendations.
In this study, both top and bottom hardness values were obtained as the effectiveness of cure at the top surface does not ensure proper polymerization throughout the restoration. Light intensity is greatly reduced as light passes through the bulk of the material due to scattering of light by the filler particles and the resin matrix. As the bottom surface is more critically affected by the light intensity, it is considered as a better gauge of the effectiveness of cure of composite.[5] The bottom surfaces of all the specimens had lesser VHN than the top surface, which means that the degree of curing decreases with depth. The difference in the mean hardness ratio was not significant, indicating no significant difference in the mean hardness values of top and bottom surfaces. Thus, it can be inferred that the specimens had undergone an almost uniform degree of polymerization from top to bottom. This can be due to the 2 mm thickness of the specimens, which has been determined to be of an adequate depth for proper curing.[16] Ideally, the hardness ratio should be one if polymerization is completely effective, as the hardness of the bottom surface should be the same as the top surface. Taking into account light scattering and absorption within composite, the hardness gradient should not exceed 10-20% or hardness ratio should be 0.8 or greater for composites to be adequately polymerized.[17] All light curing mode combinations fulfilled this criteria.
Curing nanocomposite with QTH LCU resulted in significantly higher top hardness indicating QTH cures nanocomposite better as compared to LED LCUs. Even in case of micro-hybrid composite specimens, curing with QTH LCU resulted in higher hardness values, though the difference was not statistically significant. Thus, the hypothesis that there is no difference between VHN of micro-hybrid, and nanocomposites cured with various curing protocols were proved to be null and void. Light intensity readings of all the LCUs were standardized to be above 300 W/cm2, as decreased light intensity is shown to affect the mechanical properties such as compressive strength.[18] The LCUs used in this study varied in their power density (400 mW/cm2, 950 mW/cm2 and 1000 mW/cm2), but their energy density was above 16 J/cm2. At this level, the difference in the power density does not influence the polymerization kinetics.[19] The difference between the hardness values may be explained by the differences in the ability of LED and QTH to excite the photoinitiators present in the materials. Most resin based materials have camphoroquinone as the initiator of curing, which is sensitive to light at the blue region of the visible spectrum. However, camphoroquinone has some limitations; hence, some materials contain other initiators of cure that are not excited within the wavelength range covered by LED lamps. The bis-acyl-phosphine oxide and the 1-phenyl-1, 2-propanodione, for example, are initiators with absorption peaks at 380 nm and 410 nm, respectively, which are not effectively polymerized by LED LCUs due to its narrow spectrum range.[9] The LCUs used in this study had spectrum range of 400-500 nm for QTH LCU, 450-490 nm for first LED LCU and 440-480 nm for second LED LCU. Thus the better curability of composite resins with QTH LCU could be due to its wider spectrum range. In a study done by Peris et al., where the micro hardness of micro fill and micro-hybrid composite resins cured with different curing units was evaluated, it was found that the QTH gave the highest hardness values than the LEDs.[2] Similar results have been obtained in studies carried out by Dunn and Bush,[4] Cefaly et al.[9] and Oberholzer et al.[10] where the micro hardness values of micro fill and micro-hybrid composite resins cured with QTH was greater than that by LEDs.
Furthermore, it was found that amongst all the groups, the highest mean value for the top surface was for nanocomposite (Filtek Z350) specimens cured with QTH LCU, the difference being statistically significant. In a study conducted by Topcu et al. also, nanocomposite material showed the highest hardness values in all polymerization types at the top and bottom surfaces.[20] This could be, because, the particle size of nanofillers are below the wavelength range of visible light and thus, they do not scatter or absorb visible light. The extremely small size of nanofillers allows the particles to fit into spaces between other particles and effectively increases the overall filler level. Nanofillers also significantly reduce the effect of polymerization shrinkage and dramatically improve physical properties.[21] Hubbezoglu et al. did a study comparing surface micro hardness of four different resin composites cured using a halogen light, an LED and a plasma arc unit. It was found that the nanocomposite gave the highest hardness values, with LED LCU yielding highest hardness for nanocomposites followed by hybrid resin composites.[22] In a study carried out by Soh et al. where they compared the effectiveness of cure of two LED LCUs to conventional, high intensity and very high intensity halogen lights, it was found that the effectiveness of composite cure with LED LCU is product dependent, due to variations in design and the size of the LED used.[3] In this study also, it was found that QTH LCU and first LED LCU were comparable, however, second LED LCU with standard mode gave statistically significant difference when compared with the QTH LCU.
When comparing the different modes in the same LCU, it was found that both the composite resins cured with second LED LCU in pulse cure mode (Groups 4 and 8) cured better than the ones cured in standard mode (Groups 3 and 7) though not statistically significant, which is in accordance with Neo et al.[5] Contradictory findings have been observed in other studies such as by Soh et al. where the standard modes gave significantly higher hardness values than the other curing modes when composite resin cured with different curing regimens were subjected to micro hardness test.[3] In a study done by Hegde et al.[23] the intermittent method of cure with QTH had the higher Knoop Hardness Number Knoop hardness number (KHN) than continuous mode of cure with both QTH and LED. This could be because hardness measurements were made 24 h after removal of the light source in the present study as compared to other studies where it was done immediately. Composites cured with different curing modes continue to polymerize but to different extents after the light source is removed. Pulse curing slows down the polymerization reaction, and this may be transferred to the post-irradiation polymerization of composites.[17]
One disadvantage of this study was use of teflon moulds, which tend to give higher micro hardness values than that carried out on natural teeth. Furthermore, this was an in vitro study, which tends to overestimate the micro hardness values hence results should be attributed cautiously to clinical conditions.
CONCLUSION
Under the conditions of this in vitro study, the following conclusions were made:
Effectiveness of LED LCUs as compared to QTH LCU is dependent on the type of product as well as the type of composite resin.
Curing nano composites with QTH LCU results in better surface hardness at both the top and bottom surfaces.
For micro hybrid composites, QTH LCU and LED LCUs result in comparable surface hardness at both top and bottom surfaces.
Curing with both the QTH and LED LCUs results in adequate depth of cure for both nano and microhybrid composite resins as the mean hardness ratio of all the groups were comparable.
Pulse cure mode in LED LCU does not effectively increase micro hardness than the standard mode of curing.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Burgess JO, Walker R, Davidson JM. Posterior resin-based composite: Review of the literature. Pediatr Dent. 2002;24:465–79. [PubMed] [Google Scholar]
- 2.Peris AR, Mitsui FH, Amaral CM, Ambrosano GM, Pimenta LA. The effect of composite type on microhardness when using quartz-tungsten-halogen (QTH) or LED lights. Oper Dent. 2005;30:649–54. [PubMed] [Google Scholar]
- 3.Soh MS, Yap AU, Siow KS. Effectiveness of composite cure associated with different curing modes of LED lights. Oper Dent. 2003;28:371–7. [PubMed] [Google Scholar]
- 4.Dunn WJ, Bush AC. A comparison of polymerization by light-emitting diode and halogen-based light-curing units. J Am Dent Assoc. 2002;133:335–41. doi: 10.14219/jada.archive.2002.0173. [DOI] [PubMed] [Google Scholar]
- 5.Neo BJ, Soh MS, Teo JW, Yap AU. Effectiveness of composite cure associated with different light-curing regimes. Oper Dent. 2005;30:671–5. [PubMed] [Google Scholar]
- 6.Terry DA. Direct applications of a nanocomposite resin system: Part 1-The evolution of contemporary composite materials. Pract Proced Aesthet Dent. 2004;16:417–22. [PubMed] [Google Scholar]
- 7.Mota EG, Oshima HM, Burnett LH, Jr, Pires LA, Rosa RS. Evaluation of diametral tensile strength and Knoop microhardness of five nanofilled composites in dentin and enamel shades. Stomatologija. 2006;8:67–9. [PubMed] [Google Scholar]
- 8.Wakefield CW, Kofford KR. Advances in restorative materials. Dent Clin North Am. 2001;45:7–29. [PubMed] [Google Scholar]
- 9.Cefaly DF, Ferrarezi GA, Tapety CM, Lauris JR, Navarro MF. Microhardness of resin-based materials polymerized with LED and halogen curing units. Braz Dent J. 2005;16:98–102. doi: 10.1590/s0103-64402005000200002. [DOI] [PubMed] [Google Scholar]
- 10.Oberholzer TG, Schünemann M, Kidd M. Effect of LED curing on microleakage and microhardness of Class V resin-based composite restorations. Int Dent J. 2004;54:15–20. doi: 10.1111/j.1875-595x.2004.tb00247.x. [DOI] [PubMed] [Google Scholar]
- 11.Korapati RH, Rajkumar K, Lakshminarayanan L. A Comparative evaluation of depth of cure of a posterior composite cured with light emitting diodes and halogen light cure unit. J Conserv Dent. 2004;7:58–62. [Google Scholar]
- 12.Yap AU. Effectiveness of polymerization in composite restoratives claiming bulk placement: Impact of cavity depth and exposure time. Oper Dent. 2000;25:113–20. [PubMed] [Google Scholar]
- 13.Tate WH, Porter KH, Dosch RO. Successful photocuring: Don’t restore without it. Oper Dent. 1999;24:109–14. [PubMed] [Google Scholar]
- 14.Knezević A, Tarle Z, Meniga A, Sutalo J, Pichler G, Ristić M. Degree of conversion and temperature rise during polymerization of composite resin samples with blue diodes. J Oral Rehabil. 2001;28:586–91. doi: 10.1046/j.1365-2842.2001.00709.x. [DOI] [PubMed] [Google Scholar]
- 15.Bennett AW, Watts DC. Performance of two blue light-emitting-diode dental light curing units with distance and irradiation-time. Dent Mater. 2004;20:72–9. doi: 10.1016/s0109-5641(03)00070-8. [DOI] [PubMed] [Google Scholar]
- 16.Aguiar FH, Braceiro A, Lima DA, Ambrosano GM, Lovadino JR. Effect of light curing modes and light curing time on the microhardness of a hybrid composite resin. J Contemp Dent Pract. 2007;8:1–8. [PubMed] [Google Scholar]
- 17.Yap AU, Soh MS. Curing efficacy of a new generation high-power LED lamp. Oper Dent. 2005;30:758–63. [PubMed] [Google Scholar]
- 18.Menon P, Jonathan R, Lakshmi Narayanan LL. Intensity of the light cure units: A survey in the city of Chennai. J Conserv Dent. 2003;6:103–6. [Google Scholar]
- 19.Gritsch K, Souvannasot S, Schembri C, Farge P, Grosgogeat B. Influence of light energy and power density on the microhardness of two nanohybrid composites. Eur J Oral Sci. 2008;116:77–82. doi: 10.1111/j.1600-0722.2007.00506.x. [DOI] [PubMed] [Google Scholar]
- 20.Topcu FT, Erdemir U, Sahinkesen G, Yildiz E, Uslan I, Acikel C. Evaluation of microhardness, surface roughness, and wear behavior of different types of resin composites polymerized with two different light sources. J Biomed Mater Res B Appl Biomater. 2010;92:470–8. doi: 10.1002/jbm.b.31540. [DOI] [PubMed] [Google Scholar]
- 21.Bayne SC, Heymann HO, Swift EJ., Jr Update on dental composite restorations. J Am Dent Assoc. 1994;125:687–701. doi: 10.14219/jada.archive.1994.0113. [DOI] [PubMed] [Google Scholar]
- 22.Hubbezoğlu I, Bolayir G, Doğan OM, Doğan A, Ozer A, Bek B. Microhardness evaluation of resin composites polymerized by three different light sources. Dent Mater J. 2007;26:845–53. [PubMed] [Google Scholar]
- 23.Hegde MN, Hegde P, Malhan B. Evaluation of depth of cure and knoop hardness in a dental composite, photo-activated using different methods. J Conserv Dent. 2008;11:76–81. doi: 10.4103/0972-0707.44055. [DOI] [PMC free article] [PubMed] [Google Scholar]