

Abstract
Three cases of a block to forearm rotation after a distal radius fracture were presented. The unique feature is that the surgeon should be diligent in seeking and rectifying causes of distal radioulnar joint (DRUJ) instability and rotation loss after fracture treatment.
Keywords: distal radius fracture, DRUJ, TFCC, ulnar styloid fracture, volar locking plate
Case 1: DRUJ Instability Secondary to a Combined Foveal and Distal Radioulnar Ligament Tear
A 58-year old patient sustained an intraarticular distal radius fracture with a 15° dorsal angulation and an intact ulna, AO type C1 (Fig. 1). Her fracture was treated in plaster for 5 weeks. When rehabilitation started, her ulna would subluxate in a volar direction after 20° of supination from neutral. At 65°, further rotation was not possible. In addition, she could not fully flex her little finger into her palm because of impingement from the volarly subluxated ulnar head. Using Mino's1 radioulnar line on axial computed tomography (CT) scans, it was observed that over 50% of her ulna was volar to the sigmoid notch in supination (Fig. 2). Under anesthesia, the examination confirmed that there was volar subluxation of the ulna in all positions of rotation. Distal radioulnar joint (DRUJ) arthroscopy using a 1.9-mm scope (Smith & Nephew, Andover, Massachusetts) confirmed a foveal tear of the triangular fibrocartilage complex (TFCC). Furthermore, upon exploration of the DRUJ through a dorsal incision through the extensor carpi ulnaris (ECU) subsheath, it was discovered that the TFCC was torn off from the dorsal wrist capsule. This allowed subluxation of the ulna out of the sigmoid notch. Employing Nakamura's technique, two diverging 1.2-mm drill holes were made in her ulna toward the fovea, and repair was effected with 3–0 Ethibond (Ethicon, Somerville, New Jersey) sutures introduced through two transosseous tunnels.2 This procedure reduced the ulna back into the sigmoid notch, and full rotation was restored (Video 1). The patient was placed in an above-elbow splint for 2 weeks followed by a wrist brace for 3 weeks. Hand therapy commenced immediately after surgery. She regained full flexion of her little finger immediately and full DRUJ rotation by 6 weeks. Reduction of the ulna into the sigmoid notch removed the obstruction to the flexor tendon excursion.
Fig. 1.

Case 1: No apparent DRUJ incongruity after 6 weeks of plaster immobilization
Fig. 2.

Case 1: CT confirming ulnar volar subluxation.
Video 1
Note the patient's left wrist cannot supinate fully compared with the right. As it approaches ∼60° of supination from neutral, the left ulna drops in a volar direction compared with the right. This in turn blocks further supination.
Note that the patient is unable to flex her left little finger fully at the metacarpophalangeal (MCP) joint.
Note portals for DRUJ arthroscopy, just distal to the ulna. Using a 1.9-mm scope, the joint can be seen. Here, the undersurface of the TFCC is frayed and is detached from the fovea.
A longitudinal flap is raised to expose the DRUJ. Branches of the ulnar nerve are carefully identified and preserved. The ECU tendon is exposed; through its subsheath, the capsule of the DRUJ is incised; and the fovea at the base of the ulnar styloid is identified. Two parallel 1.2-mm drill holes were made. Using 21-gauge needles carrying 3–0 nylon looped upon itself, the sutures are placed through the bone tunnels, and into the torn edge of the TFCC. The nylon loops are then used as shuttle to bring a double strand of 3–0 Ethibond sutures and out through the shaft of the ulnar neck cortex. The TFCC is then reduced into position, and the sutures are tied to secure it back into the fovea.
Online content including video sequences viewable at: www.thieme-connect.com/ejournals/html/doi/10.1055/s-0033-1342966.
Case 2: Malunion of a Basi–Ulnar Styloid Fracture as a Block to Rotation
A 33-year-old patient sustained a distal radius fracture, AO type C2 (Fig. 3). There was 50° of dorsal tilt of the distal fragment with marked cortical comminution and an ulna plus variance. The radius fracture was stabilized with a volar locking plate (Aculoc, Acumed, Hillsboro, Oregon). The basi-styloid base fracture was fixed with the Acutwist pin (Acumed, Hillsboro, Oregon) and reinforced with a tension band using polyethylene suture (Maxbraid, Biomet, Warsaw, Indiana) (Fig. 4). At the patient's first therapy session after 5 weeks in a splint, it was noted that she had a complete block of forearm rotation. In addition, there was no dorsal or volar translation at the DRUJ. Lateral radiographs and CT scans confirmed a volar dislocation of the ulna at the DRUJ (Fig. 5). An examination under anesthesia confirmed the findings. An attempted arthroscopic release of the radiocarpal joint was without success. Upon exploration of the DRUJ through a dorsal incision, the tension band, along with the dorsal capsule, was found to be firmly wound around the fixation pin. This forced the ulna to adopt a volar position outside the sigmoid notch. Once the fixation was removed, the ulna immediately reduced, and full rotation was restored.
Fig. 3.

Case 2: Fracture of distal radius with displaced ulnar styloid avulsion.
Fig. 4.
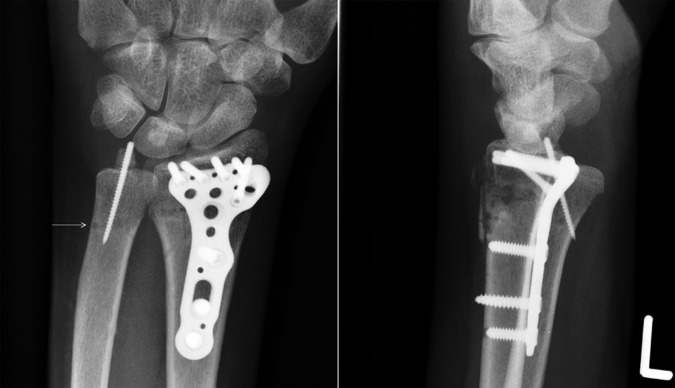
Case 2: Postoperative radiographs showing ulnar subluxation.
Fig. 5.

Case 2: CT confirming ulnar subluxation at DRUJ.
Case 3: Entrapment of ECU Tendon
A 38-year-old patient sustained an AO type C3 fracture of her distal radius with an ulnar styloid fracture that had migrated radially over the center of the distal ulna (Fig. 6). Her fractured radius was stabilized with a volar locking plate (Aculoc) without fixation of the ulnar styloid. At the first postoperative therapy visit, it was observed that her wrist was locked in neutral position. Radiographs confirmed an anatomical reduction of the distal radius fracture (Fig. 7). CT scans of her wrist showed dorsal translation of the ulna in relation to the sigmoid notch (Fig. 8). Arthroscopy at 7 weeks confirmed a tear of the TFCC. An arthroscopic lysis of adhesions was ineffective in restoring motion. Through a dorsal approach, the ECU tendon was found to have subluxated volarly into the DRUJ, thus blocking reduction of the ulna into the sigmoid notch. Once the tendon was replaced into its groove, full rotation of the DRUJ was restored (Fig. 9).
Fig. 6.

Case 3: Distal radius fracture with avulsion of ulnar styloid base. Note radial displacement of the styloid fragment.
Fig. 7.

Case 3: No apparent subluxation of DRUJ on plain radiographs.
Fig. 8.

Case 3: CT detected dorsal ulnar subluxation.
Fig. 9.

Case 3: After ECU release, DRUJ rotation restored.
Discussion
These three cases highlight the need for the treating surgeon to examine the DRUJ after surgery to ensure DRUJ stability and unrestricted forearm rotation.
Footnotes
Conflict of interest None
References
- 1.Mino D E, Palmer A K, Levinsohn E M. Radiography and computerized tomography in the diagnosis of incongruity of the distal radio-ulnar joint. A prospective study. J Bone Joint Surg Am. 1985;67(2):247–252. [PubMed] [Google Scholar]
- 2.Nakamura T, Nakao Y, Ikegami H, Sato K, Takayama S. Open repair of the ulnar disruption of the triangular fibrocartilage complex with double three-dimensional mattress suturing technique. Tech Hand Up Extrem Surg. 2004;8(2):116–123. doi: 10.1097/01.bth.0000126573.05697.29. [DOI] [PubMed] [Google Scholar]