

Abstract
From a kinetic point of view, the wrist is considered stable when it is capable of resisting load without suffering injury. Several prerequisites are necessary for the wrist to be kinetically stable: bone morphology, normal articulating surfaces, ligaments, the sensorimotor system, the muscles crossing the wrist, and all nerves connecting to ligaments and muscles. Failure of any one of these factors may result in carpal instability. The terms “scapholunate (SL) dissociation” and “SL instability” refer to one of the most frequent types of wrist instability, resulting from rupture or attenuation of the SL supporting ligaments. From a radiologic point of view, SL instability may be dynamic or static. Unlike static instabilities, which tend to be painful and dysfunctional, a good proportion of dynamic SL instabilities remain asymptomatic and stable for prolonged periods of time. Such a lack of symptoms suggests that a ligament rupture, in itself, is not enough for a joint to become unstable. Certainly, the process of achieving stability is multifactorial and involves normal joint surfaces, ligaments, muscles, and a complex network of neural connections linking all these elements. In this article, we will review the neuromuscular stabilization of the SL joint and the proprioceptive mechanisms that contribute to the dynamic carpal stabilization.
Keywords: instability, muscular control, proprioception, scapholunate, wrist
From a kinetic point of view, the wrist is considered stable when it is capable of resisting load without suffering injury.1 A stable wrist does not yield under physiologic stress. When subjected to a deforming force, a stable wrist adjusts its internal alignment and becomes a solid block through which forces can be dissipated; once the force has dissipated, the bones revert to their original position. Several prerequisites are necessary for the wrist to be kinetically stable: The bones and articular surfaces must have a normal shape with intact ligaments, the sensorimotor system2,3 needs to be finely tuned with intact proprioceptors, and the muscles crossing the wrist need to be capable of reacting quickly and efficiently when a warning message is received from the sensorimotor system. Failure of any one of these factors may result in carpal instability.
The terms “scapholunate (SL) dissociation” and “SL instability” are commonly used to describe one of the most frequent types of wrist instability, resulting from a rupture or attenuation of the SL supporting ligaments.4 From a radiologic point of view, SL instability may be dynamic or static. Dynamic SL instability is diagnosed when the diastasis between scaphoid and lunate can be observed only with motion studies or grip views, whereas a static instability is diagnosed when there is an abnormally increased diastasis between the scaphoid and lunate on static anteroposterior (AP) X-ray views. SL instability may be asymptomatic.5 Such a lack of symptoms suggests that an SL ligament rupture or attenuation by itself may not result in wrist pain, since neuromuscular stabilization of the SL joint may be a factor.
The Role of Ligaments in the Stabilization of the Carpus
When the wrist is loaded along the longitudinal axis of the forearm (axial loading), the distal row migrates proximally, inducing compressive forces across the midcarpal joint.6 The obliquely oriented scaphoid reacts to such forces by rotating on the oblique radioscaphocapitate ligament into flexion and pronation. The more the scaphoid flexes and pronates, the more the scaphotrapeziotrapezoid (STT) ligament pulls the trapezium in the palmar direction, forcing the distal row to pronate about the lunocapitate ball-and-socket articulation. If the distal row pronates, the hamate displaces dorsally, inducing an extension moment to the triquetrum via the palmar triquetrum-capitohamate ligaments. The lunate, therefore, is subjected to two opposite moments: the extension moment by the triquetrum, and the scaphoid flexion moment. If the interosseous ligaments binding the three proximal row bones are intact, the two opposite moments counteract each other and a stable equilibrium is achieved.
From this perspective, the carpus has been represented as a ring consisting of four elements (distal row, scaphoid, lunate, and triquetrum) connected by four ligamentous links (Fig. 1a).7 Rupture or attenuation of any one of these four connections would disrupt the ring, inducing one type of instability or another depending upon which link has failed. If it is the SL link that has failed, the ring will break apart, with the scaphoid collapsing into flexion and pronation and the lunate following the triquetrum into extension, resulting in a dorsal intercalated segment instability (DISI) (Fig. 1b).
Fig. 1.

(a) The carpus has been likened to a ring consisting of four elements connected by four ligamentous links. (b) In SL instability the scaphoid collapses into flexion and pronation, and the lunate follows the triquetrum into extension, resulting in DISI.
Although useful to explain certain aspects of carpal pathomechanics, the “ring” theory has an important drawback: It is based on the assumption that ligaments are able to resist high levels of tension, and this, according to recent investigations, is not accurate.8 The average yield strength of the dorsal SL ligament is only 260 newtons, certainly not strong enough to be the key stabilizer of a substantial load-bearing joint. Indeed, the bulk of the wrist-stabilizing duty must be taken up by the muscles. This does not mean, however, that ligaments are not important, just the contrary: Ligaments are the first line of defense against any destabilizing agent. When a disturbing force risks injuring the joint, the ligaments are the first to react by holding bones together while providing the proprioceptive information that the sensorimotor system will need to activate an adequate muscular response. This will be the subject of the following section.
The Sensory and Proprioceptive Function of the Scapholunate Ligament
Several ligaments connect the scaphoid to the neighboring bones: the anterolateral radioscaphoid ligament, the palmar radioscaphocapitate ligament, the radioscapholunate (ligament of Testut), the three portions of the SL interosseous ligament (palmar, proximal, and dorsal), the dorsal scaphotriquetral ligament, the palmar scaphocapitate ligament, the anterolateral STT ligament, and the corresponding capsules (Fig. 2). All ligaments provide proprioceptive information, but the most active in this regard is the SL interosseous ligament.
Fig. 2.

Elements involved in dynamic carpal stability and pathways of proprioceptive informatio.
Extrinsic and Intrinsic Innervation of the SL Ligament
The SL interosseus ligament receives its innervation from terminal branches of the posterior interosseous nerve (PIN) and, through the ligament of Testut, the anterior interosseous nerve (AIN). The consistency of this innervation to the SL ligament led us to suspect that the intrinsic innervation in a similar fashion must be consistent. Through a series of immunohistochemical studies on the innervation pattern of the SL interosseous ligament, we now know that this ligament complex is among the most richly innervated ligaments of the wrist, with consistent findings of sensory nerve endings in both the dorsal and volar portions of the ligament.9,10,11 The primary sensory nerve ending found in the SL interosseous ligament is the Ruffini ending.9,10 This is a slowly adapting, low-threshold receptor, constantly active during joint motion,11 and particularly reactive to axial loading and tensile strain in the ligament, but not to perpendicular compressive joint forces (Fig. 3). The Ruffini ending is therefore ideal as a monitor in the SL interosseous ligament, as it signals during excessive joint position and rotation, which are the positions in which the ligament runs a risk of being torn.
Fig. 3.
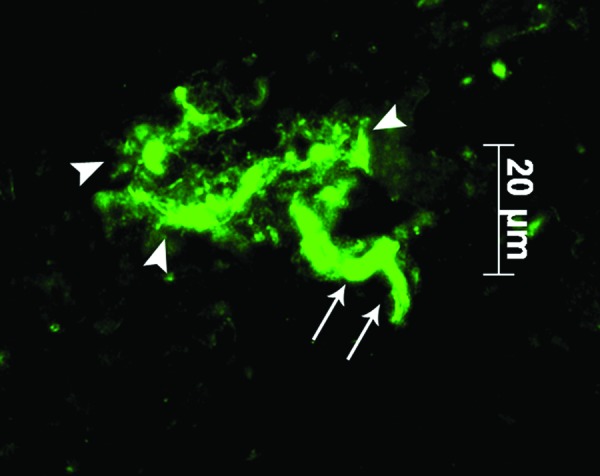
Ruffini ending as seen in a Protein Gene Product 9.5 immunofluorescence stain. The afferent axon is seen (arrows), which branches out into the ligament (arrowheads) to allow monitoring of changes in ligament tensile strain, thus signaling during extremes of joint motion and rotation.
The Scapholunate Proprioceptive Pathways
It has been postulated that an innervated ligament has a proprioceptive function through afferent signals to muscles controlling any particular joint. These ligamentomuscular reflexes12 have been demonstrated in the knee,13 the ankle,14 the shoulder,15 and, most recently, the wrist.16 These ligamentomuscular reflexes belong to the unconscious proprioception sense, or the neuromuscular sense, which includes the anticipatory control of muscles around a joint through so-called feed-forward control, as well as the ability to maintain joint stability and equilibrium unconsciously.17,18
Every wrist motion produces a specific relative motion of the proximal carpal row, which is reflected in various strains among its intrinsic ligaments. The mechanoreceptors embedded into these ligaments (SL and lunotriquetral) transform mechanical signals into afferent proprioceptive stimuli. A recent in vivo study examined the sensory action potentials (SAP) in the median nerve in five patients with preganglionic global root avulsion during the initial stage of carpal arthrodesis surgery. The SL ligament was found to generate proprioceptive stimuli at every wrist position, which was reduced in intensity after division.19
Studies on in vivo wrist joint proprioception using electromyography (EMG)16 and SAP19 have shown that the wrist has distinct patterns of reflex activation following disturbance of the SL ligament. Within 20 milliseconds of joint perturbation, antagonist muscles are activated, indicating fast joint-protective reflexes through monosynaptic spinal control.16 In a position of wrist ulnar deviation, in which the SL interosseous ligament is maximally extended and at risk of being injured, the primary reflex was an inhibition of the extensor carpi ulnaris (ECU). This was, in fact, the only wrist position in which a muscle was distinctly inhibited, suggesting an important protective joint reflex between the SL interosseous ligament and the ECU.
Hagert and Persson studied the wrist proprioceptive reflexes in eight volunteers by stimulating the SL interosseous ligament through a fine wire electrode while EMG activity was recorded from the extensor carpi radialis brevis (ECRB), ECU, flexor carpi radialis (FCR), and flexor carpi ulnaris (FCU), with the wrist in extension, flexion, radial deviation, and ulnar deviation. The PIN was then anesthetized and the experiment was repeated. Dramatic alterations in reflex patterns were observed in wrist flexion, radial deviation, and ulnar deviation following desensitization of the PIN, with an average of 72% reduction in excitatory reactions. In ulnar deviation, the inhibitory reactions of the ECU were entirely eliminated. In wrist extension, no differences in the reflex patterns were observed.20 These studies suggest that denervation of the AINor PIN21,22 affects the unconscious neuromuscular control of the wrist joint.
Role of Muscles in the Stabilization of the Wrist
Distal to the radiocarpal joint, most wrist motor tendons have an oblique course toward their distal insertion. The abductor pollicis longus (APL), for instance, runs from a dorsal position at the level of the first extensor compartment to an anterolateral position at the base of the first metacarpal. The ECU, by contrast, has an opposite oblique direction, from the dorsum of the ulna to the anteromedial corner of the fifth metacarpal. They are both dorsal at the level of the distal radius but diverge distally toward either the medial or lateral corners of the wrist. When these muscles contract, aside from an axial centripetal force to the wrist, they generate a pronation or supination moment to the distal row depending on the obliquity of their distal insertion: The medially inserted tendons induce intracarpal pronation, while the laterally inserted tendons pull the wrist into supination (Fig. 4). We have recently shown in a cadaver model that the APL, the extensor carpi radialis longus (ECRL), and the FCU are intracarpal supinators and protect the carpus from excessive pronation, while the FCR and the ECU are distal row pronators.23,24,25 The balance between these stabilizes the carpus.
Fig. 4.

Wrist motor tendons diverge distally toward their insertions in the bases of the metacarpals. When these muscles contract, they generate a pronation or supination moment to the distal row depending on the obliquity of their distal insertion: in the dorsum of the wrist, medially inserted tendons (ECU) induce intracarpal pronation, while the laterally inserted tendons (APL, ECRL) pull the wrist into supination.
It is important to emphasize that the terms “pronation” and “supination” are used here to describe not a forearm rotation but an axial rotation of the distal row relative to the radius. The distal row rotates internally (supination) or externally (pronation) until the midcarpal crossing ligaments become taut, at which point both distal and proximal rows, solidly engaged, supinate or pronate together until the radiocarpal ligaments stop that rotational motion.
We also analyzed the muscular effects on the three-dimensional alignment of specific carpal bones in normal cadaver wrists as well as in wrists with a complete SL dissociation.23,24,25 In such cases, the scaphoid behaves as if it were a distal-row bone when loaded. When the ECU muscle contracts, both the distal row and the scaphoid rotate into extreme pronation. The lunate, by contrast, stays behind in a relatively ulnar translocated position, resulting in a large scapholunate gap. If the supinator muscles (ECRL, APL, and FCU) contract, the scaphoid is pulled by the STT ligament into extension and supination, which reduces the scapholunate gap, and the scaphoid proximal pole also drops back to its normal reduced position in the scaphoid fossa. Indeed, the muscles that generate intracarpal supination are “SL-friendly muscles” that protect the scaphoid from being dragged into a subluxed position away from the lunate. The ECU, by contrast, is an “SL-unfriendly muscle,” whose contraction increases both the gap and the SL malalignment. This was substantiated by Hagert et al, who demonstrated that a stimulation of the SL interosseous ligament resulted in a contraction of all of the supinator muscles to protect the joint against injury, while the ECU was inhibited.16
The role of the FCR muscle as a potential scaphoid stabilizer has been controversial.26,27 In the cadaver it has been demonstrated that the tendon always causes scaphoid flexion, regardless of the position of the wrist. Furthermore, under FCR loading, both the distal row and the triquetrum consistently flex and pronate, but the scaphoid supinates.24 If the scaphoid supinates while the triquetrum pronates, the dorsal SL ligament is likely to decrease in tension. The FCR, therefore, is also an SL-friendly muscle, together with the ECRL, APL, and FCU.
Clinical Implications and Proprioceptive Rehabilitation of the SL Interosseous Ligament
In the wrist, posttraumatic osteoarthritis (OA) is most frequently seen as a result of injury to the SL interosseous ligament. As discussed, an injury to the SL interosseous ligament, with presence of mechanoreceptors and ligamentomuscular reflexes, will entail a disturbance of proprioception.15 It has been postulated that the ligamentomuscular reflexes may have a role in protecting a joint from excessive excursion and from excessive loading, which might have a protective effect on the development of posttraumatic OA.28,29 We believe that denervation procedures should be performed with caution, especially in wrists where the proprioceptive function may already be compromised, such as with advanced wrist osteoarthritis, and should be generally avoided in minor procedures, such as with removal of ganglion cysts.30 As such, we have described nerve-sparing approaches to both the dorsal and volar aspect of the radiocarpal joint.30
Conscious training of muscles that protect the carpus from further malalignment and subsequently protect the SL joint is one future direction that we are exploring.31
Conflict of interest None
Note
The work was performed in the laboratory of biomechanics in the Department of Anatomy, University of Barcelona, Barcelona, Spain and Department of Clinical Science and Education, Karolinska Institutet, Stockholm, Sweden.
References
- 1.The Anatomy and Biomechanics Committee of the International Federation of Societies for Surgery of the Hand . Definition of carpal instability. J Hand Surg Am. 1999;24(4):866–867. [PubMed] [Google Scholar]
- 2.Riemann B L, Lephart S M. The sensorimotor system, part I: the physiologic basis of functional joint stability. J Athl Train. 2002;37(1):71–79. [PMC free article] [PubMed] [Google Scholar]
- 3.Riemann B L, Lephart S M. The sensorimotor system, part II: the role of proprioception in motor control and functional joint stability. J Athl Train. 2002;37(1):80–84. [PMC free article] [PubMed] [Google Scholar]
- 4.Garcia-Elias M. New York, NY: Churchill Livingstone; 2011. Carpal instability; pp. 465–521. [Google Scholar]
- 5.Picha B M, Konstantakos E K, Gordon D A. Incidence of bilateral scapholunate dissociation in symptomatic and asymptomatic wrists. J Hand Surg Am. 2012;37(6):1130–1135. doi: 10.1016/j.jhsa.2012.03.020. [DOI] [PubMed] [Google Scholar]
- 6.Garcia-Elias M. Kinetic analysis of carpal stability during grip. Hand Clin. 1997;13(1):151–158. [PubMed] [Google Scholar]
- 7.Lichtman D M, Wroten E S. Understanding midcarpal instability. J Hand Surg Am. 2006;31(3):491–498. doi: 10.1016/j.jhsa.2005.12.014. [DOI] [PubMed] [Google Scholar]
- 8.Berger R A. The ligaments of the wrist. A current overview of anatomy with considerations of their potential functions. Hand Clin. 1997;13(1):63–82. [PubMed] [Google Scholar]
- 9.Hagert E, Forsgren S, Ljung B O. Differences in the presence of mechanoreceptors and nerve structures between wrist ligaments may imply differential roles in wrist stabilization. J Orthop Res. 2005;23(4):757–763. doi: 10.1016/j.orthres.2005.01.011. [DOI] [PubMed] [Google Scholar]
- 10.Hagert E, Garcia-Elias M, Forsgren S, Ljung B O. Immunohistochemical analysis of wrist ligament innervation in relation to their structural composition. J Hand Surg Am. 2007;32(1):30–36. doi: 10.1016/j.jhsa.2006.10.005. [DOI] [PubMed] [Google Scholar]
- 11.Mataliotakis G, Doukas M, Kostas I, Lykissas M, Batistatou A, Beris A. Sensory innervation of the subregions of the scapholunate interosseous ligament in relation to their structural composition. J Hand Surg Am. 2009;34(8):1413–1421. doi: 10.1016/j.jhsa.2009.05.007. [DOI] [PubMed] [Google Scholar]
- 12.Hagert E. Stockholm, Sweden: Dept of Clinical Science and Education, Section of Hand Surgery, Karolinska Institutet; 2008. Wrist Ligaments—Innervation Patterns and Ligamento-Muscular Reflexes [dissertation] [Google Scholar]
- 13.Krogsgaard M R, Dyhre-Poulsen P, Fischer-Rasmussen T. Cruciate ligament reflexes. J Electromyogr Kinesiol. 2002;12(3):177–182. doi: 10.1016/s1050-6411(02)00018-4. [DOI] [PubMed] [Google Scholar]
- 14.Konradsen L, Ravn J B, Sørensen A I. Proprioception at the ankle: the effect of anaesthetic blockade of ligament receptors. J Bone Joint Surg Br. 1993;75(3):433–436. doi: 10.1302/0301-620X.75B3.8496215. [DOI] [PubMed] [Google Scholar]
- 15.Diederichsen L P, Nørregaard J, Krogsgaard M, Fischer-Rasmussen T, Dyhre-Poulsen P. Reflexes in the shoulder muscles elicited from the human coracoacromial ligament. J Orthop Res. 2004;22(5):976–983. doi: 10.1016/j.orthres.2003.12.019. [DOI] [PubMed] [Google Scholar]
- 16.Hagert E, Persson J K, Werner M, Ljung B O. Evidence of wrist proprioceptive reflexes elicited after stimulation of the scapholunate interosseous ligament. J Hand Surg Am. 2009;34(4):642–651. doi: 10.1016/j.jhsa.2008.12.001. [DOI] [PubMed] [Google Scholar]
- 17.Lephart S M, Riemann B L, Fu F H. Champaign, IL: Human Kinetics; 2000. Introduction to the sensorimotor system; pp. xvii–xxiv. [Google Scholar]
- 18.Sjölander P, Johansson H, Djupsjöbacka M. Spinal and supraspinal effects of activity in ligament afferents. J Electromyogr Kinesiol. 2002;12(3):167–176. doi: 10.1016/s1050-6411(02)00017-2. [DOI] [PubMed] [Google Scholar]
- 19.Vekris M D, Mataliotakis G I, Beris A E. The scapholunate interosseous ligament afferent proprioceptive pathway: a human in vivo experimental study. J Hand Surg Am. 2011;36(1):37–46. doi: 10.1016/j.jhsa.2010.10.002. [DOI] [PubMed] [Google Scholar]
- 20.Hagert E, Persson J K. Desensitizing the posterior interosseous nerve alters wrist proprioceptive reflexes. J Hand Surg Am. 2010;35(7):1059–1066. doi: 10.1016/j.jhsa.2010.03.031. [DOI] [PubMed] [Google Scholar]
- 21.Gay A, Harbst K, Hansen D K, Laskowski E R, Berger R A, Kaufman K R. Effect of partial wrist denervation on wrist kinesthesia: wrist denervation does not impair proprioception. J Hand Surg Am. 2011;36(11):1774–1779. doi: 10.1016/j.jhsa.2011.07.027. [DOI] [PubMed] [Google Scholar]
- 22.Patterson R W, Van Niel M, Shimko P, Pace C, Seitz W H Jr. Proprioception of the wrist following posterior interosseous sensory neurectomy. J Hand Surg Am. 2010;35(1):52–56. doi: 10.1016/j.jhsa.2009.10.014. [DOI] [PubMed] [Google Scholar]
- 23.Salva-Coll G, Garcia-Elias M, Leon-Lopez M T, Llusá-Perez M, Rodríguez-Baeza A. Effects of forearm muscles on carpal stability. J Hand Surg Eur Vol. 2011;36(7):553–559. doi: 10.1177/1753193411407671. [DOI] [PubMed] [Google Scholar]
- 24.Salvà-Coll G, Garcia-Elias M, Llusá-Pérez M, Rodríguez-Baeza A. The role of the flexor carpi radialis muscle in scapholunate instability. J Hand Surg Am. 2011;36(1):31–36. doi: 10.1016/j.jhsa.2010.09.023. [DOI] [PubMed] [Google Scholar]
- 25.Salva-Coll G, Garcia-Elias M, Leon-Lopez M M, Llusá-Perez M, Rodríguez-Baeza A. Role of the extensor carpi ulnaris and its sheath on dynamic carpal stability. J Hand Surg Eur Vol. 2012;37(6):544–548. doi: 10.1177/1753193411430921. [DOI] [PubMed] [Google Scholar]
- 26.Jantea C L, An K N, Linscheid R L, Coonney W P. New York, NY: Plenum Press; 1994. The role of the scapho-trapezial-trapezoidal ligament complex on scaphoid kinematics; pp. 345–361. [Google Scholar]
- 27.Kobayashi M, Garcia-Elias M, Nagy L. et al. Axial loading induces rotation of the proximal carpal row bones around unique screw-displacement axes. J Biomech. 1997;30(11–12):1165–1167. doi: 10.1016/s0021-9290(97)00080-8. [DOI] [PubMed] [Google Scholar]
- 28.O'Connor B L, Brandt K D. Neurogenic factors in the etiopathogenesis of osteoarthritis. Rheum Dis Clin North Am. 1993;19(3):581–605. [PubMed] [Google Scholar]
- 29.O'Connor B L, Vilensky J A. Peripheral and central nervous system mechanisms of joint protection. Am J Orthop. 2003;32(7):330–336. [PubMed] [Google Scholar]
- 30.Hagert E, Ferreres A, Garcia-Elias M. Nerve-sparing dorsal and volar approaches to the radiocarpal joint. J Hand Surg Am. 2010;35(7):1070–1074. doi: 10.1016/j.jhsa.2010.03.032. [DOI] [PubMed] [Google Scholar]
- 31.Hagert E Proprioception of the wrist joint: a review of current concepts and possible implications on the rehabilitation of the wrist J Hand Ther 20102312–16., quiz 17 [DOI] [PubMed] [Google Scholar]