

Abstract
Purpose
This study was designed to evaluate the efficacy of a fat clearing technique for accurate nodal staging of rectal cancer patients after preoperative chemoradiotherapy (CRT).
Methods
A total of 19 patients with rectal cancer within 10 cm from anal verge were divided into two groups: non-CRT group (n = 10) and CRT group (n = 9). For pathologic assessment, lymph node (LN) harvest was performed using conventional manual dissection followed by a fat clearing technique.
Results
A median of 3.0 additional LNs in non-CRT group and 3.8 LNs in CRT group were identified by the fat clearing technique. When subanalysis was performed in patients with fewer than 12 retrieved LNs, a median of 4.0 extra LNs in non-CRT group and 3.5 extra LNs in CRT group were identified after the fat clearing technique. None of additionally identified nodes were metastatic. In both groups, the median size of retrieved LNs following the fat clearing technique was smaller than that obtained by manual dissection (2.0 mm vs. 3.0 mm, P < 0.001).
Conclusion
The fat clearing technique allowed detection of additional LNs that were missed by the manual method, but these detected LNs were not proven to be metastatic.
Keywords: Fat clearing technique, Preoperative chemoradiotherapy, Rectal neoplasms
INTRODUCTION
Preoperative chemoradiotherapy (CRT) followed by total mesorectal excision has become a standard way of management of advanced rectal cancer. Both the oncologic outcomes and the chance of sphincter preservation surgery have been improved with this approach [1-4]. The presence of metastasis in regional lymph nodes is known to be the most potent prognostic factor after preoperative CRT [4-6]. Examination of an adequate number of lymph nodes is a crucial step to prevent understaging. It has been reported that preoperative CRT reduces the number of harvested lymph nodes in rectal cancer specimens [7-9] and the incidence of fewer than 12 examined lymph nodes was more frequent after preoperative CRT. Reduction of lymph node size might be the main reason for the decreased number of harvested lymph nodes in the irradiated specimens worked up with conventional manual dissection [6,10,11].
The fat clearing technique has been suggested to facilitate identification of lymph nodes in mesorectum of specimens. Several investigators have reported that the number of lymph nodes examined per specimen is increased when using the fat clearing technique compared with the manual method, with reported increases from 6.1 to 18.9 [12], 3.1 to 10.6 [13] and even from 21.2 to 73.3 lymph nodes [14]. However, despite a strong expectation that retrieval of more lymph nodes will enhance the accuracy of staging after preoperative CRT, there are few studies that validate the clinical efficacy of the fat clearing technique.
The aim of this study was to evaluate the efficacy of the fat clearing technique for accurate nodal staging after preoperative CRT in rectal cancer patients.
METHODS
Study population
A total of 19 patients who were diagnosed with primary rectal cancer between June 2008 and December 2009 were enrolled in this prospective pilot study. All patients had histologically proven adenocarcinoma of the rectum with the tumor located within 10 cm from the anal verge. The following patients were excluded; 1) patients with past history of abdominal or pelvic surgery and/or irradiation, 2) patients with recurrent cancer, 3) patients who were administrated immunosuppressants including steroids, 4) patients with tumor confined to the mucosal layer, 5) patients who underwent endoscopic resection of a primary tumor in the rectum.
Among the 19 patients eligible for this study, 10 patients without preoperative CRT were categorized into non-CRT group and nine patients with preoperative CRT were classified as CRT group.
Preoperative CRT was performed with a 5-fluorouracil (5-FU)-based regimen and concurrent pelvic radiation. The total radiation dose was 5,040 cGy with 25 fractions of 180 cGy/day, 5 days per week, over 5 weeks using the four-field box technique. A total of 4,500 cGy was given to the pelvis followed by an additional 540 cGy to the tumor bed. 5-FU was given intravenously at a dose of 425 mg/m2/day during the first and fifth weeks of radiotherapy.
All patients underwent traditional total mesorectal excision with lymph node dissection 6 to 8 weeks after chemoradiation. Two colorectal surgeons with experiences over 300 cases of rectal cancer were participated in this study. Both laparoscopic and open surgical approaches of rectal cancer were included. The extracted specimens were staged by experienced pathologists according to the American Joint Committee on Cancer 7th system.
Fat clearing technique
For pathologic assessment, lymph node harvest was performed by two steps. First, all specimens were processed by conventional manual dissection for regional lymph node assessment after fixation in 10% formalin for 24 hours. For subsequent fat clearing, the remaining tissue was placed in a clearing solution (99.9% alcohol) for 24 hours, embedded in 99% acetone for 24 hours, and immersed in xylene for an additional 24 hours.
Sections (3-mm thickness) of all dissected lymph nodes were made from paraffin-embedded blocks and stained with hematoxylin and eosin. After the fat clearing technique, the lymph nodes were detected as chalk white foci against the background of yellow fat tissue [15]. Microscopic examination was performed by pathologists and the number and size of all retrieved lymph nodes were measured.
Statistical analysis
All statistical analysis was performed using the IBM SPSS ver. 18.0 (IBM Co., Armonk, NY, USA). Categorical variables were analyzed using chi-square test or Fisher exact test, and continuous variables were analyzed using Mann-Whitney U test. A value of P < 0.05 was considered statistically significant.
RESULTS
The characteristics of each group are shown in Table 1. There was no statistically significant difference between the two groups.
Table 1.
Patient demographics
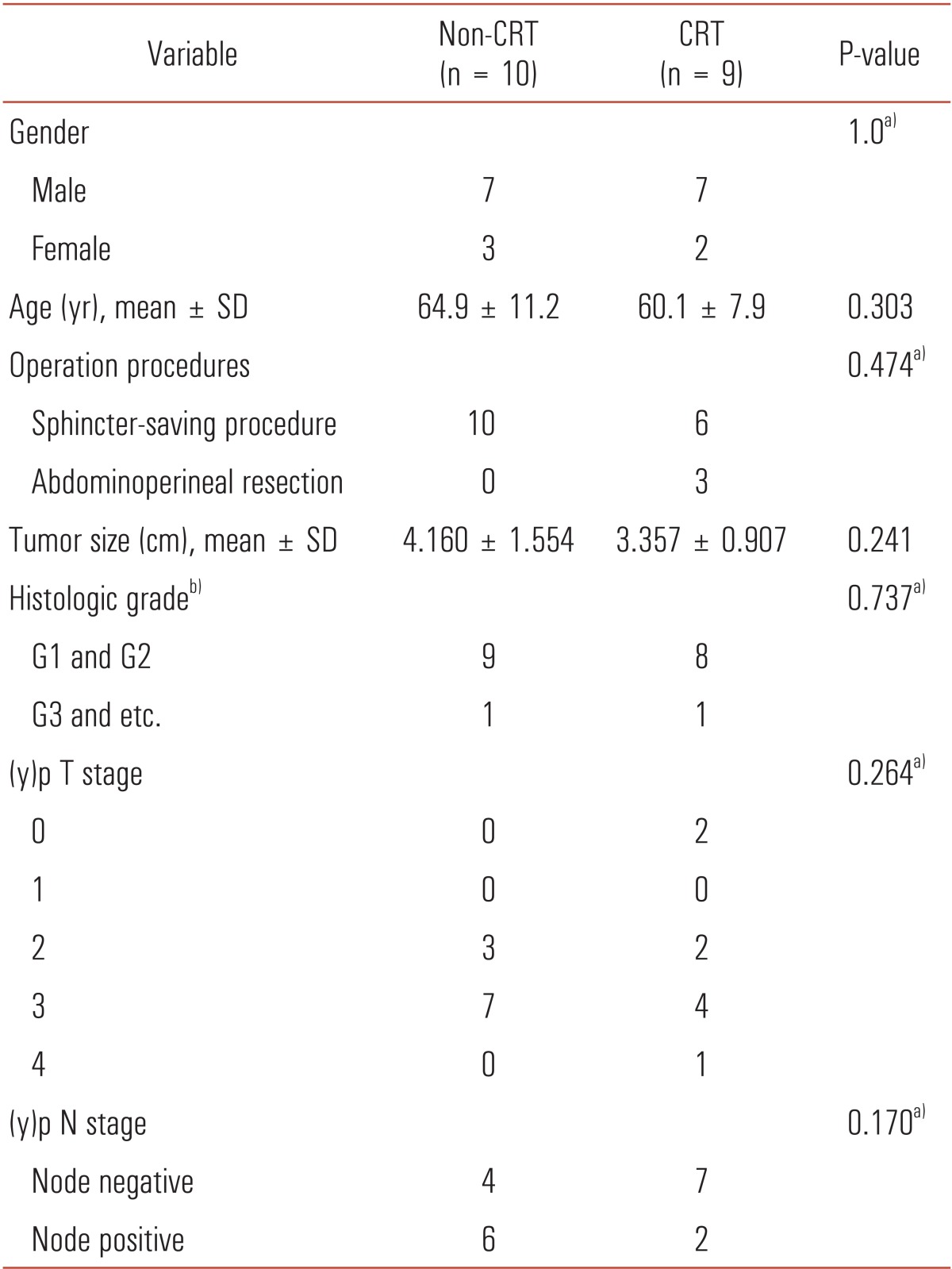
CRT, chemoradiotherapy; SD, standard deviation.
a)Fisher exact test. b)Histologic grade. G1, well differentiated; G2, moderately differentiated; G3, poorly differentiated; etc., mucinous or signet ring cell.
Retrieved lymph node size and number after manual dissection and fat clearing technique
A total of 138 and 132 lymph nodes were obtained in non-CRT and CRT group respectively by manual dissection. In non-CRT group, 14 of 138 lymph nodes were proven to be metastatic lymph nodes, compared with 6 of 132 lymph nodes in CRT group. The median number of total retrieved lymph nodes by manual dissection was 13.5 in non-CRT group and 14.0 in CRT group (P = 0.971). The median number of metastatic lymph nodes was 1.0 in non-CRT group and 0 in CRT group (P = 0.182) (Table 2).
Table 2.
Comparison of metastatic and retrieved LNs between the two groups
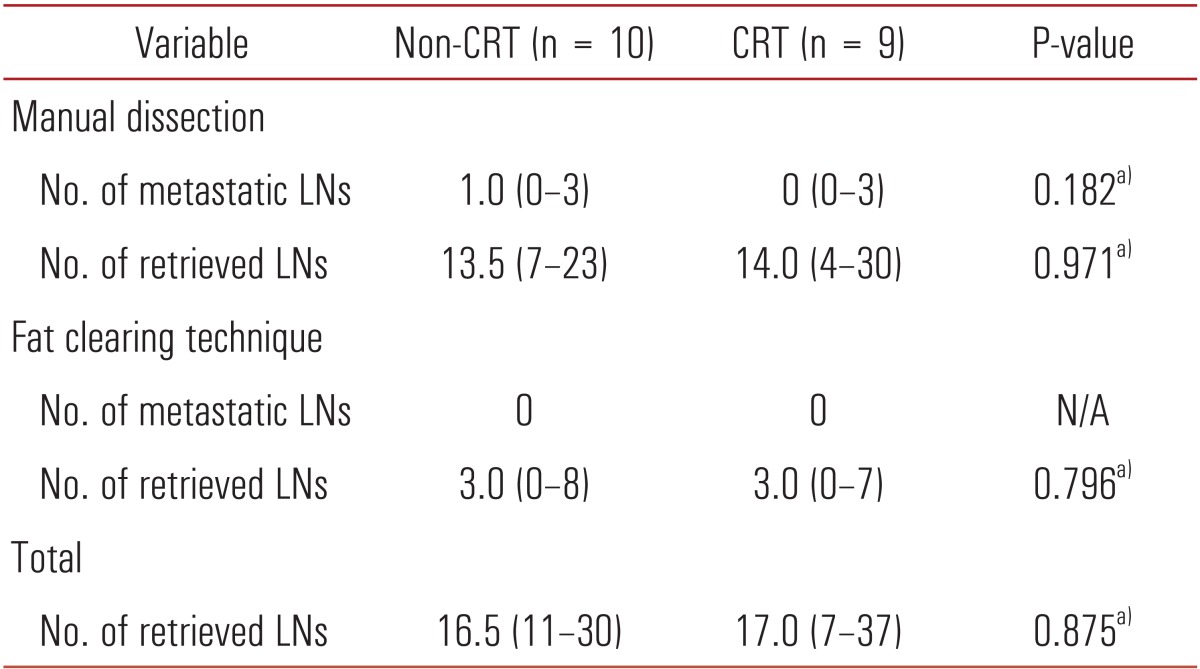
Values are presented as median (interquartile range).
LNs, lymph nodes; CRT, chemoradiotherapy.
a)Mann-Whitney U test.
After the fat clearing technique, a total of 36 additional lymph nodes, corresponding to a median value of 3.0, were retrieved in non-CRT group and a total of 35 additional lymph nodes (median, 3.0) were harvested in CRT group. However, there were no metastatic lymph nodes among these additional retrieved nodes.
When performing manual dissection only, three patients in non-CRT group and four patients in CRT group had fewer than 12 retrieved lymph nodes. In patients with fewer than 12 retrieved lymph nodes, a median of 4.0 additional lymph nodes were detected after the fat clearing technique in non-CRT group and a median 3.5 additional lymph nodes were harvested in CRT group. However, there were no metastatic lymph nodes among the additional harvested lymph nodes. In patients who had more than 12 lymph nodes removed, a median of 3.0 additional lymph nodes were retrieved after the fat clearing technique in both groups (Table 3). Regardless of the recommended retrieval of 12 lymph nodes, there was no statistically significant difference in additional lymph nodes retrieved using the fat clearing technique between the two groups.
Table 3.
Comparison of retrieved LNs between patients with <12 LNs and ≥12 LNs
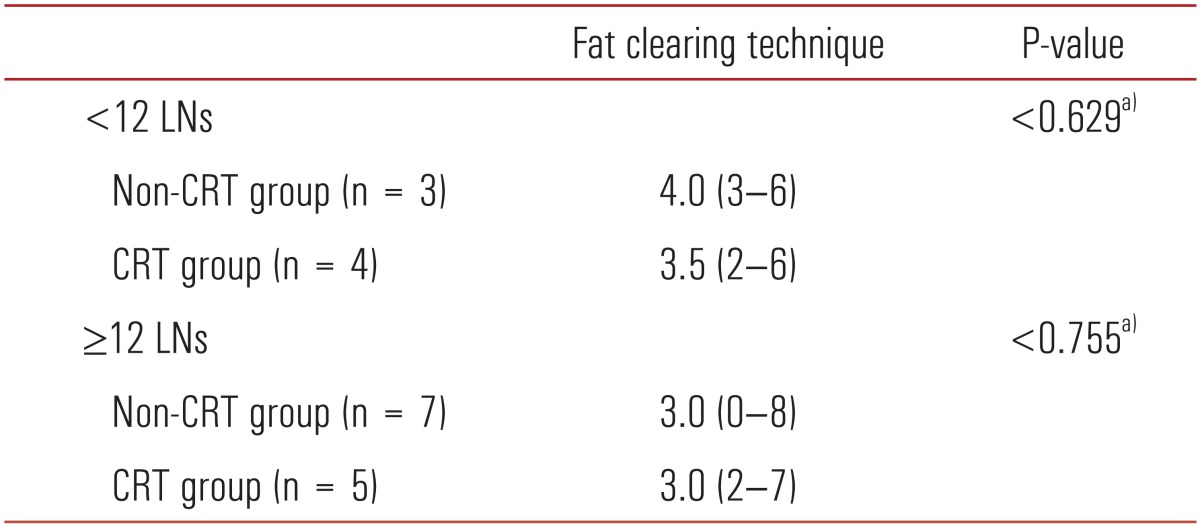
Values are presented as median (interquartile range).
LNs, lymph nodes; CRT, chemoradiotherapy.
a)Mann-Whitney U test.
In both non-CRT and CRT group, the median size of retrieved lymph nodes by manual dissection was larger than that of nodes obtained using the fat clearing technique (3.0 mm vs. 2.0 mm, P < 0.001 for both groups) (Fig. 1).
Fig. 1.

Median size of retrieved lymph nodes with or without fat clearing technique in (A) non-CRT group, and in (B) CRT group. CRT, chemoradiotherapy.
DISCUSSION
This study revealed that the fat clearing technique was useful for detecting small lymph nodes that were missed by the manual dissection technique. However, retrieval of more lymph nodes by the fat clearing technique was not related to migration to advanced stage disease.
In management of locally advanced rectal cancer, preoperative CRT has been regarded as a standard treatment based on proven benefit [2,16]. However, preoperative CRT is associated with decreased number of examined lymph nodes [8,17-19]. This has the potential risk of understaging, which may result in an inappropriate decision for postoperative adjuvant therapy or inaccurate prediction of the patient's prognosis. The main reason of decreased number in harvested lymph nodes after preoperative CRT is the decreased size of lymph nodes [8,17]. Irradiation of lymphoid tissue causes complete atrophy, lymphocyte depletion, or mesenteric fibrosis, which ultimately leads to size reduction of lymph nodes [6-8,20].
For the reason, several efforts have been tried to increase the number of harvested lymph nodes, even there is no standard guideline regarding adequate number of examined lymph nodes after preoperative CRT. Since it was first described by Gilchrist and David in 1942, additional retrieval of lymph nodes with the fat clearing technique has been reported to range from 7 to over 50 extra lymph nodes [12-14]. In addition, fat clearing technique makes it possible to identify lymph nodes smaller than 4 mm in maximum diameter [21,22].
Although the fat clearing technique has been proposed as a useful tool for accurate nodal staging in rectal cancer, there has been little effort to apply this technique in patients who undergo preoperative CRT. Wang et al. [6] reported that the fat clearing technique resulted in an increase in overall total number of dissected lymph nodes and the number of positive lymph nodes in a neoadjuvant group. They found an increase in retrieved lymph nodes from 5.2 to 20.4 in the neoadjuvant group and an increase in the number of metastatic lymph nodes from 0.4 to 1.2.
Based on recent analysis of Surveillance, Epidemiology, and End Results (SEER) database, the mean lymph node harvest was reported as 10.2 in stage II and 12.9 in stage III rectal cancer [23]. Especially, mean 10.1 lymph nodes were harvested in patients without radiation, whereas mean 8.3 lymph nodes were retrieved in patients after preoperative CRT. In the current study, a median 14.0 lymph nodes per patient were harvested from the resected specimen after preoperative CRT by the traditional manual method and an additional median 3.0 lymph nodes were obtained by the fat clearing technique. Compared with previous results, the number of retrieved lymph nodes by manual dissection was higher, whereas that of additional lymph nodes harvested after the fat clearing technique in our study was relatively low. However, previous studies that reported upstaging after the fat clearing technique [6,12,21,24], did not mention the size of retrieved lymph nodes, which paradoxically can interfere with the quality of traditional manual dissection. In our study, the median size of lymph nodes retrieved by manual dissection in patients who received preoperative CRT was 3.0 mm. This small size might reflect the fact that one certified pathologist who specialized in colorectal disease performed precise pathologic assessment by manual dissection and may explain the relatively small additional benefit of fat clearing.
Despite the efficacy of the fat clearing technique in retrieving an adequate number of lymph nodes, clinical impact of this method has been controversial. With consideration of time-consuming procedure, there is no consensus that the fat clearing technique is superior over manual dissection and precise manual dissection by a specialized pathologist is expected to provide adequate detection of metastatic lymph nodes.
In addition, the clinical significance of small lymph nodes should be considered. We found that the median size of lymph nodes in patients with preoperative CRT after the fat clearing technique was significantly smaller than that of lymph nodes retrieved by manual dissection. This means that additional lymph nodes that were missed in the manual dissection technique due to their small size can be harvested by the application of the fat clearing technique. However, there is a linear relationship between node size and detection of metastases [25] and the majority of missed lymph nodes were smaller than 2 mm in this study, it appears that the traditional manual method can identify metastatic lymph nodes well enough to establish accurate nodal staging. It is possible that small metastatic lymph nodes might be sterilized by preoperative radiation and, as a result, comparatively larger metastatic lymph nodes would be left even after preoperative CRT. Nevertheless, these findings should be validated with further large-scale studies.
In conclusion, our data demonstrated that the fat clearing technique allowed detection of additional lymph nodes that were missed by the manual method, but these detected lymph nodes were not proven to be metastatic. Therefore, the fat clearing technique did not show clinical efficacy to migration to the advanced postoperative stage after preoperative CRT.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Folkesson J, Birgisson H, Pahlman L, Cedermark B, Glimelius B, Gunnarsson U. Swedish Rectal Cancer Trial: long lasting benefits from radiotherapy on survival and local recurrence rate. J Clin Oncol. 2005;23:5644–5650. doi: 10.1200/JCO.2005.08.144. [DOI] [PubMed] [Google Scholar]
- 2.Kapiteijn E, Marijnen CA, Nagtegaal ID, Putter H, Steup WH, Wiggers T, et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer. N Engl J Med. 2001;345:638–646. doi: 10.1056/NEJMoa010580. [DOI] [PubMed] [Google Scholar]
- 3.Kim DW, Lim SB, Kim DY, Kim TH, Jung KH, Kim DH, et al. Pre-operative chemo-radiotherapy improves the sphincter preservation rate in patients with rectal cancer located within 3 cm of the anal verge. Eur J Surg Oncol. 2006;32:162–167. doi: 10.1016/j.ejso.2005.10.002. [DOI] [PubMed] [Google Scholar]
- 4.Lim SB, Yu CS, Hong YS, Kim TW, Kim JH, Kim JC. Long-term outcomes in patients with locally advanced rectal cancer treated with preoperative chemoradiation followed by curative surgical resection. J Surg Oncol. 2012;106:659–666. doi: 10.1002/jso.23181. [DOI] [PubMed] [Google Scholar]
- 5.Rodel C, Martus P, Papadoupolos T, Fuzesi L, Klimpfinger M, Fietkau R, et al. Prognostic significance of tumor regression after preoperative chemoradiotherapy for rectal cancer. J Clin Oncol. 2005;23:8688–8696. doi: 10.1200/JCO.2005.02.1329. [DOI] [PubMed] [Google Scholar]
- 6.Wang H, Safar B, Wexner SD, Denoya P, Berho M. The clinical significance of fat clearance lymph node harvest for invasive rectal adenocarcinoma following neoadjuvant therapy. Dis Colon Rectum. 2009;52:1767–1773. doi: 10.1007/DCR.0b013e3181b14eaf. [DOI] [PubMed] [Google Scholar]
- 7.Morcos B, Baker B, Al Masri M, Haddad H, Hashem S. Lymph node yield in rectal cancer surgery: effect of preoperative chemoradiotherapy. Eur J Surg Oncol. 2010;36:345–349. doi: 10.1016/j.ejso.2009.12.006. [DOI] [PubMed] [Google Scholar]
- 8.Baxter NN, Morris AM, Rothenberger DA, Tepper JE. Impact of preoperative radiation for rectal cancer on subsequent lymph node evaluation: a population-based analysis. Int J Radiat Oncol Biol Phys. 2005;61:426–431. doi: 10.1016/j.ijrobp.2004.06.259. [DOI] [PubMed] [Google Scholar]
- 9.Marijnen CA, Nagtegaal ID, Klein Kranenbarg E, Hermans J, van de Velde CJ, Leer JW, et al. No downstaging after short-term preoperative radiotherapy in rectal cancer patients. J Clin Oncol. 2001;19:1976–1984. doi: 10.1200/JCO.2001.19.7.1976. [DOI] [PubMed] [Google Scholar]
- 10.Wijesuriya RE, Deen KI, Hewavisenthi J, Balawardana J, Perera M. Neoadjuvant therapy for rectal cancer down-stages the tumor but reduces lymph node harvest significantly. Surg Today. 2005;35:442–445. doi: 10.1007/s00595-004-2956-5. [DOI] [PubMed] [Google Scholar]
- 11.Koh DM, Chau I, Tait D, Wotherspoon A, Cunningham D, Brown G. Evaluating mesorectal lymph nodes in rectal cancer before and after neoadjuvant chemoradiation using thin-section T2-weighted magnetic resonance imaging. Int J Radiat Oncol Biol Phys. 2008;71:456–461. doi: 10.1016/j.ijrobp.2007.10.016. [DOI] [PubMed] [Google Scholar]
- 12.Cawthorn SJ, Gibbs NM, Marks CG. Clearance technique for the detection of lymph nodes in colorectal cancer. Br J Surg. 1986;73:58–60. doi: 10.1002/bjs.1800730124. [DOI] [PubMed] [Google Scholar]
- 13.Choi CH, Kim WD, Lee SJ, Park WY. Clinical predictive factors of pathologic tumor response after preoperative chemoradiotherapy in rectal cancer. Radiat Oncol J. 2012;30:99–107. doi: 10.3857/roj.2012.30.3.99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Maloney KF, Heller D, Baergen RN. Types of maternal hypertensive disease and their association with pathologic lesions and clinical factors. Fetal Pediatr Pathol. 2012;31:319–323. doi: 10.3109/15513815.2012.659391. [DOI] [PubMed] [Google Scholar]
- 15.Yao YF, Wang L, Liu YQ, Li JY, Gu J. Lymph node distribution and pattern of metastases in the mesorectum following total mesorectal excision using the modified fat clearing technique. J Clin Pathol. 2011;64:1073–1077. doi: 10.1136/jclinpath-2011-200190. [DOI] [PubMed] [Google Scholar]
- 16.Sauer R, Becker H, Hohenberger W, Rodel C, Wittekind C, Fietkau R, et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med. 2004;351:1731–1740. doi: 10.1056/NEJMoa040694. [DOI] [PubMed] [Google Scholar]
- 17.Scott N, Thorne C, Jayne D. Lymph node retrieval after neoadjuvant radiotherapy for rectal adenocarcinoma. J Clin Pathol. 2004;57:335–336. doi: 10.1136/jcp.2003.013441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Luna-Perez P, Rodriguez-Ramirez S, Alvarado I, Gutierrez de la Barrera M, Labastida S. Prognostic significance of retrieved lymph nodes per specimen in resected rectal adenocarcinoma after preoperative chemoradiation therapy. Arch Med Res. 2003;34:281–286. doi: 10.1016/s0188-4409(03)00041-9. [DOI] [PubMed] [Google Scholar]
- 19.Wichmann MW, Muller C, Meyer G, Strauss T, Hornung HM, Lau-Werner U, et al. Effect of preoperative radiochemotherapy on lymph node retrieval after resection of rectal cancer. Arch Surg. 2002;137:206–210. doi: 10.1001/archsurg.137.2.206. [DOI] [PubMed] [Google Scholar]
- 20.Thorn CC, Woodcock NP, Scott N, Verbeke C, Scott SB, Ambrose NS. What factors affect lymph node yield in surgery for rectal cancer? Colorectal Dis. 2004;6:356–361. doi: 10.1111/j.1463-1318.2004.00670.x. [DOI] [PubMed] [Google Scholar]
- 21.Hida J, Mori N, Kubo R, Matsuda T, Morikawa E, Kitaoka M, et al. Metastases from carcinoma of the colon and rectum detected in small lymph nodes by the clearing method. J Am Coll Surg. 1994;178:223–228. [PubMed] [Google Scholar]
- 22.Hida J, Yasutomi M, Fujimoto K, Ieda S, Machidera N, Kubo R, et al. Analysis of regional lymph node metastases from rectal carcinoma by the clearing method. Justification of the use of sigmoid in J-pouch construction after low anterior resection. Dis Colon Rectum. 1996;39:1282–1285. doi: 10.1007/BF02055123. [DOI] [PubMed] [Google Scholar]
- 23.Chou JF, Row D, Gonen M, Liu YH, Schrag D, Weiser MR. Clinical and pathologic factors that predict lymph node yield from surgical specimens in colorectal cancer: a population-based study. Cancer. 2010;116:2560–2570. doi: 10.1002/cncr.25032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Hernanz F, Garcia-Somacarrera E, Fernandez F. The assessment of lymph nodes missed in mesenteric tissue after standard dissection of colorectal cancer specimens. Colorectal Dis. 2010;12(7 Online):e57–e60. doi: 10.1111/j.1463-1318.2009.01987.x. [DOI] [PubMed] [Google Scholar]
- 25.Murphy J, Pocard M, Jass JR, O'Sullivan GC, Lee G, Talbot IC. Number and size of lymph nodes recovered from dukes B rectal cancers: correlation with prognosis and histologic antitumor immune response. Dis Colon Rectum. 2007;50:1526–1534. doi: 10.1007/s10350-007-9024-3. [DOI] [PubMed] [Google Scholar]