

Abstract
Far infrared (FIR) radiation (λ = 3–100 μm) is a subdivision of the electromagnetic spectrum that has been investigated for biological effects. The goal of this review is to cover the use of a further sub-division (3– 12 μm) of this waveband, that has been observed in both in vitro and in vivo studies, to stimulate cells and tissue, and is considered a promising treatment modality for certain medical conditions. Technological advances have provided new techniques for delivering FIR radiation to the human body. Specialty lamps and saunas, delivering pure FIR radiation (eliminating completely the near and mid infrared bands), have became safe, effective, and widely used sources to generate therapeutic effects. Fibers impregnated with FIR emitting ceramic nanoparticles and woven into fabrics, are being used as garments and wraps to generate FIR radiation, and attain health benefits from its effects.
Keywords: far infrared radiation, radiant heat, blackbody radiation, biogenetic rays, FIR emitting ceramics and fibers, infrared sauna
1 Introduction
All living organisms are subjected to the natural electromagnetic radiation reaching the earth from the sun. Living organisms experience the beneficial as well as adverse effects of it at all levels, starting from sub-cellular organelles and ending with the whole body. Thermal radiation (or infrared) is a band of energy in the complete electromagnetic spectrum and it has been used effectively for millennia to treat/ease certain maladies and discomforts. Heated saunas are only one of the avenues (and perhaps the oldest) to deliver the radiation in a controlled environment and within a convenient treatment time. With the development of better technology to deliver pure far infrared radiation (FIR), the benefits from its effects have widened. Nowadays, specialty FIR emitting heat lamps and garments made up of filaments (fibers) impregnated with FIR emitting nanoparticles are becoming used to deliver these thermal radiation effects. In this paper we explore the use of FIR as a promising treatment modality for certain medical conditions. We cover both traditional applications and novel applications, and survey the latest technological advancements and most recent scientific studies in the field.
1.1 What is FIR radiation?
With respect to the complete electromagnetic radiation spectrum, the infrared radiation (IR) band covers the wavelength range of 750 nm–100 μm, frequency range of 400 THz–3 THz, and photon energy range of 12.4 meV– 1.7 eV. It lies between the long wavelength red edge of the visible and the short edge of the terahertz (starting at 3 THz) spectral bands (Figure 1).
Figure 1.
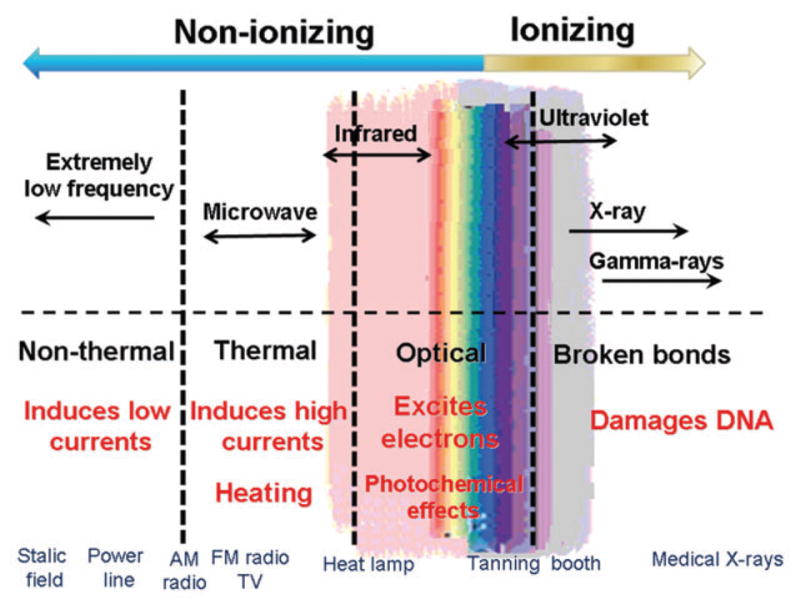
The spectrum of electromagnetic radiation and some biological changes it may induce.
The classification of the International Commission on Illumination (CIE) has three sub-divisions for the IR radiation as given in Table 1. An alternative classification provided in ISO 20473 standard for the sub-division of the IR ranges is given in Table 2.
Table 1.
CIE classification of IR radiation.
| Name/abbreviation | Wavelength | Photon energy (THz) |
|---|---|---|
| Near infrared/IR-A | 0.7– 1.4 μm (700– 1400 nm) | 215– 430 |
| Mid infrared/IR-B | 1.4– 3.0 μm (1400– 3000 nm) | 100– 215 |
| Farinfrared/IR-C | 3.0– 100 μm (3000 nm– 0.1 mm) | 3– 100 |
Table 2.
ISO 20473 standard for sub-division of the IR.
| Name/abbreviation | Wavelength (μm) |
|---|---|
| Near IR, NIR | 0.78 – 3 |
| Mid IR, MIR | 3.0 – 50 |
| Far IR, FIR | 50 – 1000 |
In the IR radiation bands, only FIR transfers energy purely in the form of heat which can be perceived by the thermoreceptors in human skin as radiant heat [1]. Not only is FIR absorbed by the human body but it is also emitted by the body in the form of black body radiation (3–50 μm with an output peak at 9.4 μm).
The term “black body” was first used by Gustav Kirchoff in 1860. In essence, all matter absorbs electromagnetic radiation to some degree and an object that absorbs all radiation falling on it (at all wavelengths and frequencies) is called a black body, i.e., a perfect absorber. When a black body is at a uniform temperature state, it emits back this absorbed energy, and it is termed as “ black body radiation ”. This is a type of radiation and has continuous frequency/intensity which depends only on the black body’s temperature, and the type of spectrum it generates is called the Planck spectrum. In this type of spectrum, spectral peaks at characteristic frequencies are shifted to higher values (shorter wavelengths) with increasing temperature values. For instance, at room temperature most of the emission of the black body is in the infrared region of the electromagnetic spectrum. At a typical environmental background temperature, which is around 300 K, the peak emission is at about 9.7 μm (and the curve covers the FIR region as well); at around 1800 K (temperature of molten steel), the peak is shifted to 1.6 μm; at around 6000 K (surface temperature of the sun), the peak is shifting even further, 0.48 μm, which now is in the visible (blue) region of the spectrum. Peak shifts of some representative black body temperatures and the range of electromagnetic radiation they fall into are given in Figure 2A, B. This type of shift in the emission peaks of the black bodies (to shorter wavelengths at higher temperatures) is governed by Wien’s displacement law.
Figure 2.

(A) Planck’s law. Dependence of spectral radiant emittance (ωλ) for perfect blackbodies as a function of wavelength (λ). (B) Wien’s displacement law. The wavelength of maximal radiant exitance (λmax) as a function of the absolute temperature (T) for a perfect black body (dashed line) and different bodies.
1.2 Biological effects of FIR
FIR application in medicine requires understanding and knowledge of the interactions of electromagnetic radiation at FIR range with biological structures (including cells, cell membranes, cell fluids – especially water, DNA/proteins) and functioning of the living systems in general. At the cellular level, the underlying biophysical mechanisms of the interaction of electromagnetic radiation with living cells can be framed in terms of altered cell membrane potentials and altered mitochondrial metabolism [2]. FIR energy (photons with quantum energy levels of 12.4 meV –1.7 eV) is absorbed by vibrational levels of bonds in molecules. There are six vibrational modes covering symmetric and antisymmetric stretching, scissoring, rocking, wagging and twisting. Considering the high concentration of water in biological systems, association of water molecules with ions (solvation effect), the dielectric properties of the water and the large dipole moment that this effect generates, this will be a dominant factor in biological solutions. It is known that at lower frequencies water molecules are able to rotate freely in an oscillating electric field with little or almost no energy loss. However, if the frequency of the electric field reaches 108 Hz levels, the rotational mode becomes hindered (due to “dielectric friction ” effect) and the absorbed energy starts dissipating by collision or nearest neighbor interactions in the media [2]. The dielectric relaxation of water at 310 K is around 25 GHz where the rotational response of the dipoles to the electromagnetic field is spread over a broad frequency range.
In living systems, in addition to the water molecules association with the electromagnetic field and effects of that, one has to consider the “meso-structure” effect where proteins and charged groups (located at specific sites on the proteins) are crucial for the overall biological activity. These specifically located charged groups associate with the water molecules and by doing this influence the dielectric behavior of the whole molecular-assembly, which in turn effects its biologic functioning. Thus, the dielectric properties of tissues (even at cellular level) depend on and vary with the water content. In addition, the relaxation of these molecular “meso-structures” can show variations with frequency. For these reasons, water content is a critical factor in the interaction between FIR and living organisms.
In this regard, the dynamics of water-clusters has attracted considerable interest since there is a noticeable difference with respect to the dynamics of bulk-liquid-water, and this may have significant implications in biological environments. Local changes in the molecular environment (caused by solvation or confinement) are shown to affect substantially the translational and vibrational modes in FIR frequency range. It is found that water cluster size and temperature affect the FIR absorption spectrum significantly [3].
2 Medical applications of FIR
For FIR used as a therapeutic modality the alternative terms “biogenetic radiation” and “biogenetic rays” have been coined and widely used in the popular literature. FIR wavelength is too long to be perceived by the eyes, however, the body experiences its energy as a gentle radiant heat which can penetrate up to 1.5 inches (almost 4 cm) beneath the skin. FIR energy is sufficient to exert rotational and vibrational modes of motion in bonds forming the molecules (including the water molecules) as well as resonate with cellular frequencies. Resulting epidermal temperature is higher when the skin is irradiated with FIR than if similar thermal loads from shorter wavelengths are used. The prolonged erythermal response due to FIR exposure has been proposed to be due to increased epidermal temperatures associated with it, but levels of FIR that do not produce any detectable skin heating can also have biological effects.
2.1 Biomedical laboratory studies using FIR sources
2.1.1 FIR heat lamps
There have been many attempts to use FIR as a therapeutic intervention where devices known as “infrared heat lamps” that emit more or less FIR are been used. Unfortunately, “ pure ” FIR emitting lamps are expensive, and thus, in some instances lamps that have “mixed” emission, i.e., emit in shorter (mid infrared, MIR; near infrared, NIR and even visible light) wavelength ranges are been used. A common type of specialized infrared heat lamp emits 2–25 μm radiation. IR saunas are often used and the most effective types have ceramic FIR emitting panels that remain cool to the touch. However, most IR saunas on the market do not use the expensive FIR panels, which can be touched since they remain always cold.
There have been a few laboratory studies that have reported the biological effects of FIR. A recent important paper describes the in vitro use of an FIR generator (WS TY-301R®; M/s WS Far Infrared Medical Technology Co., Ltd., Taipei, Taiwan; see Figure 3) as a radiation source to irradiate human umbilical vein endothelial cells (HUVECs) [4]. In the study, FIR exposure (a low non-thermal irradiance) of 0.13 mW/cm2 for 30 min inhibited proliferation and the vascular endothelial growth factor (VEGF)-induced phosphorylation of extracellular signal-regulated kinases in HUVECs. Furthermore, FIR exposure induced the phosphorylation of endothelial nitric oxide synthase (eNOS) and nitric oxide (NO) generation in VEGF-treated HUVECs. Both VEGF-induced NO and reactive oxygen species (ROS) generation was involved in the inhibitory effect of FIR. Nitrotyrosine formation increased significantly in HUVECs treated with VEGF and FIR together. Inhibition of phosphoinositide 3-kinase (PI3K) by wortmannin abolished both the FIR-induced phosphorylation of eNOS and serine/threonine-specific protein kinase in HUVECs. In addition to that, FIR exposure upregulated the expression of PI3K p85 at the transcriptional level. It was observed that FIR exposure induced the nuclear translocation of promyelocytic leukemia zinc finger protein in the cells. These data provide information on how FIR exposure could affect microcirculation, independent from thermal effects. The same group had previously shown that non-thermal FIR therapy increased skin blood flow in rats [5]. Toyokawa et al. [6] used home-made ceramic FIR emitters to stimulate full thickness excisional skin wound healing in rats. After constant exposure to FIR, wound healing was significantly quickened and transforming growth factor (TGF)-beta1 expressing myofibroblasts and collagen content were increased.
Figure 3.

Medical FIR sources. (A) WS TY-301R® and (B, C) WS TY-101N® FIR lamps (both by WS Far Infrared Medical Technology Co., Ltd., Taipei, Taiwan).
Along the same lines, Akasaki et al. [7] studied in vivo the effects of repeated FIR irradiation on angiogenesis in a mouse model of hindlimb ischemia. Following reports that FIR therapy upregulated the expression of arterial eNOS in hamsters (and it is known that NO constitutively produced by eNOS plays an important role in angiogenesis) they took a step further to investigate whether the FIR therapy increases angiogenesis in mice with the hindlimb ischemia. In their study, unilateral hindlimb ischemia was induced in apolipoprotein E-deficient mice and the group to receive the FIR irradiation was placed in a FIR dry sauna at 41°C for 15 min and then at 34°C for 20 min once daily, with total duration of the experiment of 5 weeks. Laser-Doppler perfusion imaging demonstrated that at the ischemic limb, blood perfusion ratio in the irradiated group increased significantly in comparison with the control group (0.79±0.04 vs. 0.54±0.08, p<0.001). Also, in the treated group, significantly greater capillary density was observed (757±123 per mm2 vs. 416±20 per mm2, p<0.01). Western blotting showed that thermal therapy has increased markedly the hindlimb eNOS expression. Furthermore, to study possible involvement of eNOS in thermally induced angiogenesis, the same FIR therapy was given to mice with hindlimb ischemia with or without N(G)-nitro-L-arginine methyl ester (L-NAME) administration for the duration of 5 weeks. It was observed that L-NAME treatment eliminated angiogenesis induced using the FIR thermal therapy and that the therapy did not increase angiogenesis in eNOS-deficient mice. The study led to the conclusion that angiogenesis can be induced via eNOS using FIR thermal therapy in mice with hindlimb ischemia.
Ishibashi et al. [8] did an in vitro study with five human cancer cell lines (A431, vulva; HSC3, tongue; Sa3, gingival; A549, lung; and MCF7, breast) to assess the effects of FIR irradiation. For that purpose, they used a tissue culture incubator with an imbedded FIR lamp that could continuously irradiate cells with FIR (lamp operating wavelength range being 4–20 μm with an emission peak height at 7 –12 μm). The overall observation was that the FIR effect varied in these five cancer cell line types, as can be expected. The study results showed that basal expression level of heat shock protein (HSP) 70A mRNA was higher in A431 and MCF7 cell lines in comparison with the FIR-sensitive HSC3, Sa3, and A549 cell lines. The study showed that the over expression of HSP70 inhibited FIR-induced growth arrest in HSC3 cells, and that HSP70 siRNA inhibited the proliferation of A431 cells after FIR treatment. A summary of the results of this study indicated that the proliferation-suppressing effect of FIR, in some cancer cell lines, is controlled by the basal expression level of the HSP70A. These findings suggest that FIR irradiation may be used as an effective medical treatment avenue for some cancer cells which have low levels of HSP70.
2.1.2 FIR emitting ceramics and fabrics
FIR emitting ceramics have been known for some time [9, 10]. All ceramics have the property of emitting IR radiation depending on their temperature. In the age of gas lighting, ceramic mantles were heated by gas flames to emit both IR and visible radiation depending on the temperature attained. The exact chemical composition of the ceramic material governs the relationship between the temperature and the amount of IR radiation. The radiated energy follows the Stefan-Boltzmann law which says that the total energy radiated per unit of surface area per unit of time is directly proportional to the fourth power of the black body’s absolute temperature. The wavelength range also depends strictly on the temperature according to Wien’s displacement law [11].
The boron-silicate mineral, tourmaline (known as a gemstone in its crystalline form) when milled into fine powders also emits FIR [12] and the characteristics of the FIR emission depend on the particle size. Preparations containing tourmaline powder have been applied to the skin with the aim of affecting the blood flow [13]. In a similar manner discs of FIR emitting ceramics have been attached to the skin with the intent of producing a beneficial effect (see later).
Small particles (nanoparticles and microparticles) of FIR-emitting ceramic material have been incorporated into fibers that are then woven into fabrics. These fabrics can be manufactured into various garments that can be worn on different parts of the body.
When FIR emitting ceramics or fabrics are employed as therapeutic devices, it is pertinent to analyze the thermodynamics of the process. The first law of thermodynamics states that energy can neither be created nor destroyed. Heat (molecular vibrational energy) is transferred from one body to another in three forms: radiation, convection and conduction. Thus, it is clear that the principle source of energy needed to power the FIR emission from the garments comes from the human body, since it is at a significantly higher temperature than the surrounding air. So energy from the human body is transferred to these ceramic particles, which are acting as “perfect absorbers”, maintain their temperature at sufficiently high levels and then emit FIR back to the body. It is plausible that FIR emitted from the skin is absorbed by the ceramic particles, which then re-emit the same FIR back to the skin. Although this may appear to be an energy neutral process and to cancel itself out, this is not in fact the case because the FIR emitting material will prevent the loss of FIR that would otherwise have escaped through normal clothing. However the same effect could have been achieved with a FIR reflective foil suit or suchlike. Other sources of heat that can transfer energy from the body to the ceramic particles with a net gain of FIR are either convection, conduction, or both. The balance between conduction and convection will depend on how close the contact is between the garment and the skin. If the garment is skin tight, then conduction may be important, while if it is loose fitting then convection (heating up a layer of air between the skin and the garment) may be important.
Ting-Kai Leung and colleagues have studied the effect of FIR-emitting ceramic powders in a range of biological studies [14 –19]. In one set of studies, they cultured murine myoblast cells (C2C12) with bags of ceramic powder under the culture plates and found that FIR irradiation improved cell viability and prevented lactate dehydrogenase release under hydrogen peroxide (H2O2)-mediated oxidative stress, and also elevated the intracellular levels of NO and calmodulin [14]. In the study, they used electro-stimulation of amphibian skeletal muscle and found that FIR emitting ceramics delayed the onset of fatigue, induced by muscle contractions [14]. In another set of studies, they showed that ceramic-emitted FIR (cFIR) could increase the generation of intracellular NO in breast cancer cells [15] and inhibit growth of murine melanoma cells [16]. Similarly, they found that cFIR increased calmodulin and NO production in RAW 264.7 macrophages [17]. cFIR also has been shown to increase the viability of murine macrophages with different concentrations of H2O2 [15]. In this study [15] it was shown that cFIR significantly inhibited intracellular peroxide levels and lipopolysaccharide (LPS)-induced peroxide production by macrophages. In the same study, it was also demonstrated that cFIR blocked ROS-mediated cytotoxicity (shown by measurements of cytochrome c and the ratio of NADP+/NADPH) [15].
The same research group went on to study a rabbit model of rheumatoid arthritis in which rabbits received intra-articular injections of LPS to induce inflammation that mimics the rheumatoid arthritis [18]. Fluorodeoxyglucose(18F) coupled with positron emission tomography (FDG-PET) scans were used to monitor the inflammation in 16 h and 7 days after the LPS injection. Rabbits to be treated with cFIR were placed in a cage surrounded by paper sheets impregnated with a thin layer of the ceramic powder, while the control group was surrounded by the same sheet without the material. Comparison of the final and initial uptakes of FDG isotopes in the LPS-injected left knee-joints of the rabbits indicated larger decreases in the cFIR exposed group than in the control group indicating that FIR reduced inflammation.
In their most recent study the Leung group studied the repair effect of cFIR in human breast epithelial cells (MCF-10A) after H2O2 and after ionizing radiation from an X-ray source [19]. Their results show that in both, H2O2 toxicity and radiation exposure models, the cFIR treated cells demonstrated significantly higher cell survival rates than the control groups. In view of the experimental results and taking into account the relationship between indirect ionizing radiation and the oxidative stress-induced cell damage, and accumulation of free radicals, they proposed that the ionizing radiation protective ability of cFIR occurs predominantly through an antioxidant mechanism. They are suggesting that cFIR provides cells with a defensive mechanism during the irradiation process and promotes cell repair during post exposure period through hydrogen peroxide scavenging and COX-2 inhibiting activities.
2.2 Means that are used to deliver the FIR radiation
We analyzed the peer-reviewed applications of therapeutic FIR delivery systems and realized that there are three main techniques for FIR radiation delivery: i) FIR saunas, ii) FIR ray devices and iii) FIR emitting ceramics and fabrics.
2.2.1 FIR saunas
In these cabins, the heating elements are typically heated to about 300– 400° C and the emission is in the FIR range, that is, the heat exchange between the body and the environment is almost purely radiative (radiant heating) with cabin air temperature being at around 40°C or less (Figure 4). Heating of the skin with FIR warming cabins is faster (in comparison with the conventional saunas) but higher irradiance of the skin must be applied in order to produce noticeable sweating. These cabins are frequently used in Japan where the practice is called “Waon therapy” [20, 21]. Waon therapy has been used extensively in Japan [22] and Korea [23] for cardiovascular conditions and diseases, particularly chronic heart failure [24, 25] and peripheral arterial disease [26, 27]. FIR sauna therapy has been used to improve cardiac and vascular function and reduce oxidative stress in patients with chronic heart failure [28]. Beever [29] asked whether FIR saunas could have a beneficial effect on quality of life in those patients with type II diabetes. The study consisted of 20 min, three times weekly infrared sauna sessions, over a period of 3 months. Physical health, general health, social functioning indices, and visual analogue scales (VAS) measurements for stress and fatigue all improved in the treatment group. A study of patients with rheumatoid arthritis and ankylosing spondylitis showed a reduction in pain, stiffness, and fatigue during infrared sauna therapy [30].
Figure 4.
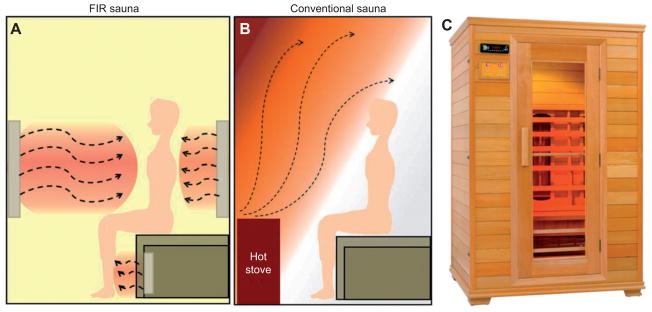
FIR sauna. (A, B) Comparison of FIR sauna with conventional heated sauna. (C) Cabin incorporating FIR emitting “cold” unit(s) (Anhui Hi-Tech Electronic Commerce Co., Ltd., Hefei, China).
2.2.2 FIR ray devices
Common devices are WS TY-101N® and WS TY-301R® (made by WS Far Infrared Medical Technology Co., Ltd., Taipei, Taiwan; see Figure 3). A report from Hu and Li [31] describes the treatment of allergic rhinitis. A WS TY-101N® FIR emitter was placed 30 cm from the patient’s nasal region. The treatment was performed for 40 min every morning for 7 days. Every day, patients recorded their symptoms in a diary before and during treatment. Each symptom of rhinitis was rated on a 4-point scale (0–3) according to severity. During the period of FIR therapy, the symptoms of eye itching, nasal itching, nasal stuffiness, rhinorrhea, and sneezing were all significantly improved. Smell impairment was improved after the last treatment. Lin et al. [32] used a WS TY-101N® FIR emitter to treat vascular access malfunction with an inadequate access flow (Qa) in hemodialysis (HD) patients. This randomized trial demonstrated that FIR therapy could improve access flow and potency of the native arteriovenous fistula (AVF) in a total of 145 HD patients (73 in the control group and 72 in the FIR-treated group). FIR was used for 40 min, and hemodynamic parameters were measured by the HD02 monitor (M/s Transonic System Inc.), during the hemodialysis. In comparison with control subjects, patients who received FIR therapy for 1 year had a lower incidence (12.5 vs. 30.1%; p<0.01) and relative incidence (one episode per 67.7 vs. one episode per 26.7 patient-months; p = 0.03) of AVF malfunction. Hausswirth et al. [33] showed that FIR therapy reduced symptoms of exercise-induced muscle damage in athletes after a simulated trail running race.
2.2.3 FIR emitting ceramics and fabrics
Discs and garments manufactured of FIR emitting ceramic material have been applied to the human body (Figure 5). For instance, a blanket containing discs has been reported to improve quality of sleep [34] and single discs were applied to the breasts of women who encountered difficulty in producing sufficient breast milk during lactation [35]. Gloves have been made out of FIR emitting fabrics and there have been reports that these gloves can be used to treat arthritis of the hands and Raynaud’s syndrome [36].
Figure 5.

FIR emitting garments and fabrics manufactured from fibers impregnated with ceramic nanoparticles (Celliant®, Hologenix, Santa Monica, CA, USA). (A) fibers, (B) yarns, (C) fabrics, (D) knee bandage brace, (E) socks, (F) gloves, (G) elbow bandage brace, (H) multi-purpose bandage, (I) performance apparel, (J) mattress, and (K) puppy blanket.
Belts made out of these fabrics have been used for weight reduction. In one study, Conrado and Munin [37] investigated whether the use of a garment made with synthetic fibers embedded with powdered ceramic led to a reduction in body measurements. The study population comprised 42 women divided into two groups: active and placebo. The volunteers used clothing either impregnated or not impregnated with ceramic powder for at least 8 h/day for 30 days. The experimental data showed a reduction in body measurements, which may be a consequence of an increment in microcirculation and peripheral blood flow, and these changes might promote improved general health.
A belt containing FIR-emitting sericite mineral (a fine grained mica) was used to study the relief of menstrual pain [38]. In this study, 104 patients with primary dysmenorrhea were randomized to wear a sericite or placebo belt during sleep for three menstrual cycles, and then followed up for two additional menstrual cycles with no belt. Hot packs were used to heat the ceramics and ensure slight pain relief in both groups. Although the severity of dysmenorrhea decreased during the treatment period in both groups, it was found that during the follow-up period, the decreased VAS (pain) score was maintained in the experimental group, whereas the VAS score gradually returned to baseline in the control group, which resulted in significant difference between the groups (p = 0.0017).
In their recent clinical study, Liau et al. [39] looked into the benefits of using an FIR emitting belt for managing the discomfort of primary dysmenorrhea in female patients. Taking into account several parameters, such as body temperature, abdominal blood flow, pain assessment, and heart rate variability, they showed that FIR belts used increased the local surface body temperature as well as the abdominal blood flow; in addition to reducing the pain and the discomfort from it. In this particular study, a THERMEDIC FIR belt (LinkWin Technology Co., Ltd., Taiwan) with the capability to generate 11.34 mW/ cm2 at 50°C was used.
Rao et al. [40] used garments made out of bioceramic-coated neoprene in conjunction with a “topical cream” to treat cellulite of the legs. Each subject was randomized to receive occlusion by the garment on either the right or left leg, with the contralateral side serving as a control with no occlusion. Of the 17 subjects who completed the study, 76% noticed an overall improvement in their cellulite, with 54 % reporting greater improvement in the thigh that received garment occlusion. Further, the evaluators found the occluded thighs to show greater improvement than the non-occluded thighs in 65 % of subjects. Bioceramic-coated neoprene garment occlusion potentiated the effect of the topical agent in cellulite reduction. A follow up two-center, double-blinded, randomized trial found similar results [41].
Celliant® (Hologenix, Santa Monica, CA, USA) is a polyethylene terephthalate (PET) fiber that incorporates FIR emitting ceramic nanoparticles. York and Gordon [42] studied socks manufactured from Celliant® fiber material in patients with chronic foot pain resulting from diabetic neuropathy or other disorders. A double-blind, randomized trial with 55 subjects (38 men, 17 women, average age 59.7 ± 11.9 years) enrolled 26 patients with diabetic neuropathy and 29 with other pain etiologies. Subjects twice completed the VAS, brief pain inventory (BPI), McGill pain questionnaire (MPQ), and a multipurpose, short form health survey with 36 questions (SF-36) a week apart [W(1+2)] before receiving either control or Celliant® socks. The same questionnaires were answered again 1 and 2 weeks later [W(3+4)]. The questionnaires provided nine scores for analyzing pain reduction: one VAS score, two BPI scores, five MPQ scores, and the bodily pain score on the SF-36. Mean W(1+2) and W(3+4) scores were compared to measure pain reduction. More pain reduction was reported by Celliant® subjects for eight of the nine pain questions employed, with a significant (p = 0.043) difference between controls and Celliant® for McGill question III. In neuropathic subjects, Celliant®; caused greater pain reduction in six of the nine questions, but not significantly. In non-neuropathic subjects eight of nine questions showed better pain reduction with the Celliant® socks.
3 Hypothesis for molecular and cellular mechanisms of FIR effects
Despite all these different uses of FIR in medical applications, the exact mechanisms of the hyperthermic effects and biological activities of FIR irradiation are still poorly understood. It is clear that two kinds of FIR therapy may exist. The first type (FIR saunas and some FIR generators powered by electricity) uses irradiances or power densities (tens of mW/cm2) that are sufficient to heat up the tissue, while others such as ceramic discs, powders, and fabrics (that use no external power but rely on energy from the body) have such low irradiances that they do not heat the tissue (0.1–5 mW/cm2). The question arises to what extent are the fundamental mechanisms of these two forms of FIR therapy the same, and to what extent are they different ? Furthermore, the question may be posed as to what degree of similarity that FIR therapy has with the reasonably well-established therapy called low level laser (light) therapy (LLLT) also known as photobiomodulation (PBM). Pertinent to this question is the fact that many devices used to deliver therapeutic visible or NIR light were approved by the US Food and Drug Administration as being equivalent to an “ infrared heat lamp ”. The cellular and molecular mechanisms of LLLT/PBM are to some extent understood and involve absorption of red or NIR light by mitochondrial chromophores such as cytochrome c oxidase (CCO, unit IV of the mitochondrial respiratory chain) [43]. This photon absorption activates the enzyme possibly by photo-dissociating the inhibitory molecule, NO, from the copper B (CuB) site [44]. This loss of NO allows electron transport, oxygen consumption, and adenosine triphosphate (ATP) to rapidly increase and results in a marked rise in mitochondrial membrane potential (MMP) that gives rise to a brief burst of ROS [45]. Signaling pathways are activated by ATP, NO, and ROS and these lead to activation of transcription factors (such as NF-κB) [46] that lead to the long-term effects on tissue (healing, anti-inflammatory and pain relief [47]) seen after relatively transient periods of illumination.
Since the principle chromophore at FIR wavelengths is not CCO but rather water, we must ask ourselves how can the biological effects of red and NIR absorption be so similar to those seen with FIR ? Perhaps some clue can be obtained by considering the difference between the two types of FIR therapy (heating and non-heating). While heating FIR therapy is reported to increase blood flow, this result may be the simple response of increased thermoregulation that is known to occur when tissue is warmed. However, it is possible that the increase in blood flow, seen in non-heating FIR therapy, may be similar in nature to that seen in LLLT, in other words, a vasodilation due to NO release from stores in CCO [48] as well as from NO bound to hemoglobin and myoglobin [49]. How are we to explain cellular responses from low fluences of FIR that are insufficient to produce bulk heating of water in the tissue ? Perhaps the answer lies in the concept of nanostructured water layers [50]. These are thin (nano meters) layers of water that build up on hydrophobic surfaces such as cellular membranes, and they can be considered as “concentrated water ” [51]. If this description is correct, it is reasonable to assume that relatively small amounts of vibrational energy delivered by non-heating FIR could perturb the structure of the membrane underlying the nanoscopic water layer without bulk heating. Small perturbations in membrane structure could have big effects at the cell level if the membrane contains an ion channel. Ion channels (many kinds for both cations and anions [52]) are present in all cell membranes, but are particularly common in mitochondrial membranes (both inner and outer [53]). If mitochondrial ion channels (particularly calcium channels [54]) could be opened by non-heating FIR, thus increasing mitochondrial respiration, it would explain how the overall therapeutic outcomes of LLLT and non-heating FIR therapy are so similar.
It cannot be excluded that FIR could itself have effects on CCO activity. A recent study has elucidated the existence of weakly H-bonded water molecules in bovine CCO that might change during catalysis [55]. Fitting with Gaussian components indicated the involvement of up to eight waters in the photolysis transition. The fact that Fourier transform infrared (FTIR) spectroscopy is extensively employed to study the structure, function, and dynamics of CCO [56, 57] suggests that it is possible that the same wavelengths (FIR uses comparable wavelengths to FTIR) could produce changes in conformation affecting enzyme activity or binding of NO to the CuB site.
It must be emphasized that the above remains a hypothetical explanation at present, but is clearly a testable hypothesis. One could ask whether exposure of cells to non-heating FIR can affect mitochondria by for instance increasing ATP, increasing oxygen consumption, producing NO and ROS, affecting MMP and calcium levels. One could also ask whether cells that are rich in mitochondria respond well to non-heating FIR, in the same way as they do to LLLT.
4 Conclusion
If it can be proved that non-heating FIR has real and significant biological effects, then the possible future applications are wide ranging. Not only could bandages and dressings made out of NIR emitting fabrics be applied for many medical conditions and injuries that require healing, but there is a large potential market in lifestyle enhancing applications. Garments may be manufactured for performance enhancing apparel in both leisure activities and competitive sports areas. Cold weather apparel would perform better by incorporating FIR emitting capability and sleeping environments could be improved by mattresses and bedding emitting FIR.
Acknowledgments
This work was supported by the US NIH (R01AI050875 to MRH).
Contributor Information
Fatma Vatansever, Wellman Center for Photomedicine, Massachusetts General Hospital, Boston, MA, USA; and Department of Dermatology, Harvard Medical School, Boston, MA, USA.
Michael R. Hamblin, Department of Dermatology, Harvard Medical School, Boston, MA, USA; and Harvard-MIT Division of Health Sciences and Technology, Cambridge, MA, USA.
References
- 1.Plaghki L, Decruynaere C, Van Dooren P, Le Bars D. The fine tuning of pain thresholds: a sophisticated double alarm system. PLoS One. 2010;5(4):e10269. doi: 10.1371/journal.pone.0010269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Sheppard AR, Swicord ML, Balzano Q. Quantitative evaluations of mechanisms of radiofrequency interactions with biological molecules and processes. Health Phys. 2008;95(4):365–96. doi: 10.1097/01.HP.0000319903.20660.37. [DOI] [PubMed] [Google Scholar]
- 3.Lee MS, Baletto F, Kanhere DG, Scandolo S. Far-infrared absorption of water clusters by first-principles molecular dynamics. J Chem Phys. 2008;128(21):214506. doi: 10.1063/1.2933248. [DOI] [PubMed] [Google Scholar]
- 4.Hsu YH, Chen YC, Chen TH, Sue YM, Cheng TH, Chen JR, Chen CH. Far-infrared therapy induces the nuclear translocation of PLZF which inhibits VEGF-induced proliferation in human umbilical vein endothelial cells. PLoS One. 2012;7(1):e30674. doi: 10.1371/journal.pone.0030674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Yu SY, Chiu JH, Yang SD, Hsu YC, Lui WY, Wu CW. Biological effect of far-infrared therapy on increasing skin microcirculation in rats. Photodermatol Photoimmunol Photomed. 2006;22(2):78–86. doi: 10.1111/j.1600-0781.2006.00208.x. [DOI] [PubMed] [Google Scholar]
- 6.Toyokawa H, Matsui Y, Uhara J, Tsuchiya H, Teshima S, Nakanishi H, Kwon AH, Azuma Y, Nagaoka T, Ogawa T, Kamiyama Y. Promotive effects of far-infrared ray on full-thickness skin wound healing in rats. Exp Biol Med (Maywood) 2003;228(6):724–9. doi: 10.1177/153537020322800612. [DOI] [PubMed] [Google Scholar]
- 7.Akasaki Y, Miyata M, Eto H, Shirasawa T, Hamada N, Ikeda Y, Biro S, Otsuji Y, Tei C. Repeated thermal therapy up-regulates endothelial nitric oxide synthase and augments angiogenesis in a mouse model of hindlimb ischemia. Circ J. 2006;70(4):463–70. doi: 10.1253/circj.70.463. [DOI] [PubMed] [Google Scholar]
- 8.Ishibashi J, Yamashita K, Ishikawa T, Hosokawa H, Sumida K, Nagayama M, Kitamura S. The effects inhibiting the proliferation of cancer cells by far-infrared radiation (FIR) are controlled by the basal expression level of heat shock protein (HSP) 70A. Med Oncol. 2008;25(2):229–37. doi: 10.1007/s12032-007-9020-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Wang F, Liang J, Tang Q, Li L, Han L. Preparation and far infrared emission properties of natural sepiolite nanofibers. J Nanosci Nanotechnol. 2010;10(3):2017–22. doi: 10.1166/jnn.2010.2116. [DOI] [PubMed] [Google Scholar]
- 10.Liang J, Zhu D, Meng J, Wang L, Li F, Liu Z, Ding Y, Liu L, Liang G. Performance and application of far infrared rays emitted from rare earth mineral composite materials. J Nanosci Nanotechnol. 2008;8(3):1203–10. [PubMed] [Google Scholar]
- 11.Heald MA. Where is the “Wien peak”? Am J Phys. 2003;71(12):1322–3. [Google Scholar]
- 12.Meng J, Jin W, Liang J, Ding Y, Gan K, Yuan Y. Effects of particle size on far infrared emission properties of tourmaline superfine powders. J Nanosci Nanotechnol. 2010;10(3):2083–7. doi: 10.1166/jnn.2010.2072. [DOI] [PubMed] [Google Scholar]
- 13.Yoo BH, Park CM, Oh TJ, Han SH, Kang HH, Chang IS. Investigation of jewelry powders radiating far-infrared rays and the biological effects on human skin. J Cosmet Sci. 2002;53(3):175–84. [PubMed] [Google Scholar]
- 14.Leung TK, Lee CM, Tsai SY, Chen YC, Chao JS. A pilot study of ceramic powder far-infrared ray irradiation (cFIR) on physiology: observation of cell cultures and amphibian skeletal muscle. Chin J Physiol. 2011;54(4):247–54. doi: 10.4077/CJP.2011.AMM044. [DOI] [PubMed] [Google Scholar]
- 15.Leung TK, Lin YS, Lee CM, Chen YC, Shang HF, Hsiao SY, Chang HT, Chao JS. Direct and indirect effects of ceramic far infrared radiation on the hydrogen peroxide-scavenging capacity and on murine macrophages under oxidative stress. J Med Biol Eng. 2011;31(5):345–51. [Google Scholar]
- 16.Leung TK, Chan CF, Lai PS, Yang CH, Hsu CY, Lin YS. Inhibitory effects of far-infrared irradiation generated by ceramic material on murine melanoma cell growth. Int J Photoener. 2012 doi: 10.1155/2012/646845. [DOI] [Google Scholar]
- 17.Leung TK, Shang HF, Chen DC, Chen JY, Chang TM, Hsiao SY, Ho CK, Lin YS. Effects of far infrared rays on hydrogen peroxide-scavenging capacity. Biomed Eng Appl Basis Commun. 2011;23(2):99–105. [Google Scholar]
- 18.Leung TK, Chen CH, Lai CH, Lee CM, Chen CC, Yang JC, Chen KC, Chao JS. Bone and joint protection ability of ceramic material with biological effects. Chin J Physiol. 2012;55(1):47–54. doi: 10.4077/CJP.2012.AMM113. [DOI] [PubMed] [Google Scholar]
- 19.Leung TK, Lee CM, Wu CH, Chiou JF, Huang PJ, Shen LK, Hung CS, Ho YS, Wang HJ, Kung CH, Lin YH, Yeh HM, Hsiao WT. Protective effect of non-ionized radiation from far infrared ray emitting ceramic material (cFIR) against oxidative stress on human breast epithelial cells. J Med Biol Eng. 2012 doi: 10.5405/jmbe.1133. [DOI] [Google Scholar]
- 20.Taylor J. Recent pioneering cardiology developments in Japan: Japanese cardiologists have discovered Waon therapy for severe or refractory heart failure and extracorporeal cardiac shock wave therapy for severe angina pectoris. Eur Heart J. 2011;32(14):1690–1. [PubMed] [Google Scholar]
- 21.Miyata M, Tei C. Waon therapy for cardiovascular disease: innovative therapy for the 21st century. Circ J. 2010;74(4):617–21. doi: 10.1253/circj.cj-09-0939. [DOI] [PubMed] [Google Scholar]
- 22.Cho GY, Ha JW. Waon therapy, can it be new therapeutic modality in heart failure patients? J Cardiovasc Ultrasound. 2010;18(2):43–4. doi: 10.4250/jcu.2010.18.2.43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Sohn IS, Cho JM, Kim WS, Kim CJ, Kim KS, Bae JH, Tei C. Preliminary clinical experience with Waon therapy in Korea: safety and effect. J Cardiovasc Ultrasound. 2010;18(2):37–42. doi: 10.4250/jcu.2010.18.2.37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Kihara T, Miyata M, Fukudome T, Ikeda Y, Shinsato T, Kubozono T, Fujita S, Kuwahata S, Hamasaki S, Torii H, Lee S, Toda H, Tei C. Waon therapy improves the prognosis of patients with chronic heart failure. J Cardiol. 2009;53(2):214–8. doi: 10.1016/j.jjcc.2008.11.005. [DOI] [PubMed] [Google Scholar]
- 25.Miyata M, Kihara T, Kubozono T, Ikeda Y, Shinsato T, Izumi T, Matsuzaki M, Yamaguchi T, Kasanuki H, Daida H, Nagayama M, Nishigami K, Hirata K, Kihara K, Tei C. Beneficial effects of Waon therapy on patients with chronic heart failure: results of a prospective multicenter study. J Cardiol. 2008;52(2):79–85. doi: 10.1016/j.jjcc.2008.07.009. [DOI] [PubMed] [Google Scholar]
- 26.Shinsato T, Miyata M, Kubozono T, Ikeda Y, Fujita S, Kuwahata S, Akasaki Y, Hamasaki S, Fujiwara H, Tei C. Waon therapy mobilizes CD34+ cells and improves peripheral arterial disease. J Cardiol. 2010;56(3):361–6. doi: 10.1016/j.jjcc.2010.08.004. [DOI] [PubMed] [Google Scholar]
- 27.Tei C, Shinsato T, Miyata M, Kihara T, Hamasaki S. Waon therapy improves peripheral arterial disease. J Am Coll Cardiol. 2007;50(22):2169–71. doi: 10.1016/j.jacc.2007.08.025. [DOI] [PubMed] [Google Scholar]
- 28.Fujita S, Ikeda Y, Miyata M, Shinsato T, Kubozono T, Kuwahata S, Hamada N, Miyauchi T, Yamaguchi T, Torii H, Hamasaki S, Tei C. Effect of Waon therapy on oxidative stress in chronic heart failure. Circ J. 2011;75(2):348–56. doi: 10.1253/circj.cj-10-0630. [DOI] [PubMed] [Google Scholar]
- 29.Beever R. The effects of repeated thermal therapy on quality of life in patients with type II diabetes mellitus. J Altern Complement Med. 2010;16(6):677–81. doi: 10.1089/acm.2009.0358. [DOI] [PubMed] [Google Scholar]
- 30.Oosterveld FG, Rasker JJ, Floors M, Landkroon R, van Rennes B, Zwijnenberg J, van de Laar MA, Koel GJ. Infrared sauna in patients with rheumatoid arthritis and ankylosing spondylitis. A pilot study showing good tolerance, short-term improvement of pain and stiffness, and a trend towards long-term beneficial effects. Clin Rheumatol. 2009;28(1):29–34. doi: 10.1007/s10067-008-0977-y. [DOI] [PubMed] [Google Scholar]
- 31.Hu KH, Li WT. Clinical effects of far-infrared therapy in patients with allergic rhinitis. Conf Proc IEEE Eng Med Biol Soc. 2007;2007:1479–82. doi: 10.1109/IEMBS.2007.4352580. [DOI] [PubMed] [Google Scholar]
- 32.Lin CC, Chang CF, Lai MY, Chen TW, Lee PC, Yang WC. Far-infrared therapy: a novel treatment to improve access blood flow and unassisted patency of arteriovenous fistula in hemodialysis patients. J Am Soc Nephrol. 2007;18(3):985–92. doi: 10.1681/ASN.2006050534. [DOI] [PubMed] [Google Scholar]
- 33.Hausswirth C, Louis J, Bieuzen F, Pournot H, Fournier J, Filliard JR, Brisswalter J. Effects of whole-body cryotherapy vs. far-infrared vs. passive modalities on recovery from exercise-induced muscle damage in highly-trained runners. PLoS One. 2011;6(12):e27749. doi: 10.1371/journal.pone.0027749. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Inoué S, Kabaya M. Biological activities caused by far-infrared radiation. Int J Biometeorol. 1989;33(3):145–50. doi: 10.1007/BF01084598. [DOI] [PubMed] [Google Scholar]
- 35.Ogita S, Imanaka M, Matsuo S, Takebayashi T, Nakai Y, Fukumasu H, Matsumoto M, Iwanaga K. Effects of far-infrared radiation on lactation. Ann Physiol Anthropol. 1990;9(2):83–91. doi: 10.2114/ahs1983.9.83. [DOI] [PubMed] [Google Scholar]
- 36.Ko GD, Berbrayer D. Effect of ceramic-impregnated “thermoflow” gloves on patients with Raynaud’s syndrome: randomized, placebo-controlled study. Altern Med Rev. 2002;7(4):328–35. [PubMed] [Google Scholar]
- 37.Conrado LA, Munin E. Reduction in body measurements after use of a garment made with synthetic fibers embedded with ceramic nanoparticles. J Cosmet Dermatol. 2011;10(1):30–5. doi: 10.1111/j.1473-2165.2010.00537.x. [DOI] [PubMed] [Google Scholar]
- 38.Lee CH, Roh JW, Lim CY, Hong JH, Lee JK, Min EG. A multicenter, randomized, double-blind, placebo-controlled trial evaluating the efficacy and safety of a far infrared-emitting sericite belt in patients with primary dysmenorrhea. Complement Ther Med. 2011;19(4):187–93. doi: 10.1016/j.ctim.2011.06.004. [DOI] [PubMed] [Google Scholar]
- 39.Liau BY, Leung TK, Ou MC, Ho CK, Yang A, Lin YS. Inhibitory effects of far-infrared ray-emitting belts on primary dysmenorrhea. Int J Photoener. 2012 doi: 10.1155/2012/238468. [DOI] [Google Scholar]
- 40.Rao J, Paabo KE, Goldman MP. A double-blinded randomized trial testing the tolerability and efficacy of a novel topical agent with and without occlusion for the treatment of cellulite: a study and review of the literature. J Drugs Dermatol. 2004;3(4):417–25. [PubMed] [Google Scholar]
- 41.Rao J, Gold MH, Goldman MP. A two-center, double-blinded, randomized trial testing the tolerability and efficacy of a novel therapeutic agent for cellulite reduction. J Cosmet Dermatol. 2005;4(2):93–102. doi: 10.1111/j.1473-2165.2005.40208.x. [DOI] [PubMed] [Google Scholar]
- 42.York RM, Gordon IL. Effect of optically modified polyethylene terephthalate fiber socks on chronic foot pain. BMC Complement Altern Med. 2009;9:10. doi: 10.1186/1472-6882-9-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Chung H, Dai T, Sharma SK, Huang YY, Carroll JD, Hamblin MR. The nuts and bolts of low-level laser (light) therapy. Ann Biomed Eng. 2012;40(2):516–33. doi: 10.1007/s10439-011-0454-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Lane N. Cell biology: power games. Nature. 2006;443(7114):901–3. doi: 10.1038/443901a. [DOI] [PubMed] [Google Scholar]
- 45.Chen AC-H, Huang YY, Arany PR, Hamblin MR. Role of reactive oxygen species in low level light therapy. Proc SPIE. 2009 doi: 10.1117/12.814890. [DOI] [Google Scholar]
- 46.Chen AC, Arany PR, Huang YY, Tomkinson EM, Sharma SK, Kharkwal GB, Saleem T, Mooney D, Yull FE, Blackwell TS, Hamblin MR. Low-level laser therapy activates NF-κB via generation of reactive oxygen species in mouse embryonic fibroblasts. PLoS One. 2011;6(7):e22453. doi: 10.1371/journal.pone.0022453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Huang YY, Chen AC, Carroll JD, Hamblin MR. Biphasic dose response in low level light therapy. Dose Response. 2009;7(4):358–83. doi: 10.2203/dose-response.09-027.Hamblin. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Hamblin MR. The role of nitric oxide in low level light therapy. Proc SPIE. 2008 doi: 10.1117/12.764918. [DOI] [Google Scholar]
- 49.Zhang R, Mio Y, Pratt PF, Lohr N, Warltier DC, Whelan HT, Zhu D, Jacobs ER, Medhora M, Bienengraeber M. Near infrared light protects cardiomyocytes from hypoxia and reoxygenation injury by a nitric oxide dependent mechanism. J Mol Cell Cardiol. 2009;46(1):4–14. doi: 10.1016/j.yjmcc.2008.09.707. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Sommer AP, Zhu D, Mester AR, Försterling HD. Pulsed laser light forces cancer cells to absorb anticancer drugs – the role of water in nanomedicine. Artif Cells Blood Substit Immobil Biotechnol. 2011;39(3):169–73. doi: 10.3109/10731199.2010.516262. [DOI] [PubMed] [Google Scholar]
- 51.Sommer AP, Caron A, Fecht HJ. Tuning nanoscopic water layers on hydrophobic and hydrophilic surfaces with laser light. Langmuir. 2008;24(3):635–6. doi: 10.1021/la7032737. [DOI] [PubMed] [Google Scholar]
- 52.Ravna AW, Sylte I. Homology modeling of transporter proteins (carriers and ion channels) Methods Mol Biol. 2012;857:281– 99. doi: 10.1007/978-1-61779-588-6_12. [DOI] [PubMed] [Google Scholar]
- 53.Perez-Pinzon MA, Stetler RA, Fiskum G. Novel mitochondrial targets for neuroprotection. J Cereb Blood Flow Metab. 2012;32(7):1362–76. doi: 10.1038/jcbfm.2012.32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Calì T, Ottolini D, Brini M. Mitochondrial Ca(2+) as a key regulator of mitochondrial activities. Adv Exp Med Biol. 2012;942:53–73. doi: 10.1007/978-94-007-2869-1_3. [DOI] [PubMed] [Google Scholar]
- 55.Maréchal A, Rich PR. Water molecule reorganization in cytochrome c oxidase revealed by FTIR spectroscopy. Proc Natl Acad Sci USA. 2011;108(21):8634–8. doi: 10.1073/pnas.1019419108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Rich PR, Breton J. Attenuated total reflection Fourier transform infrared studies of redox changes in bovine cytochrome c oxidase: resolution of the redox Fourier transform infrared difference spectrum of heme a(3) Biochemistry. 2002;41(3):967–73. doi: 10.1021/bi0109717. [DOI] [PubMed] [Google Scholar]
- 57.Heitbrink D, Sigurdson H, Bolwien C, Brzezinski P, Heberle J. Transient binding of CO to Cu(B) in cytochrome c oxidase is dynamically linked to structural changes around a carboxyl group: a time-resolved step-scan Fourier transform infrared investigation. Biophys J. 2002;82(1 Pt 1):1–10. doi: 10.1016/S0006-3495(02)75368-X. [DOI] [PMC free article] [PubMed] [Google Scholar]