

Abstract
Freezing of gait (FOG) is a commonly observed phenomenon in Parkinson’s disease, but its causes and mechanisms are not fully understood. This paper presents the development of a virtual reality (VR)-based body-weight supported treadmill interface (BWSTI) designed and applied to investigate FOG. The BWSTI provides a safe and controlled walking platform which allows investigators to assess gait impairments under various conditions that simulate real life. In order to be able to evoke FOG, our BWSTI employed a novel speed adaptation controller, which allows patients to drive the treadmill speed. Our interface responsively follows the subject’s intention of changing walking speed by the combined use of feedback and feedforward controllers. To provide realistic visual stimuli, a three dimensional VR system is interfaced with the speed adaptation controller and synchronously displays realistic visual cues. The VR-based BWSTI was tested with three patients with PD who are known to have FOG. Visual stimuli that might cause FOG were shown to them while the speed adaptation controller adjusted treadmill speed to follow the subjects’ intention. Two of the three subjects showed FOG during the treadmill walking.
Keywords: BWSTI (body-weight supported treadmill interface), treadmill control, virtual reality, gait assessment, freeze of gait, Parkinson’s Disease
I. Introduction
Freezing of gait (FOG) is the most common yet poorly understood gait phenomenon found in Parkinson’s disease (PD). It is defined as an episodic inability to generate effective stepping [1]. To date no medication has proven to effectively treat FOG, however evidence exists showing that external environmental stimuli such as visual, auditory, and somatosensory cues can be used therapeutically to break the FOG cycle and improve gait-related mobility [2]. Adding treadmill training to external cues has been found to bring further benefits to walking in those with FOG [3]. Recently, repetitive robot-assisted treadmill training was found effective in reducing patient and clinician-reported FOG episodes [4]. Together, these studies suggest that a treadmill is a promising tool to treat FOG. However the causes and underlying mechanisms of this phenomenon are still unclear and remain critical in the development of any therapeutic intervention.
In order to investigate the causes and underlying mechanisms of FOG, we have developed a walking platform that closely simulates overground walking in a virtual environment and can simulate the same situations that cause FOG in the real world (e.g narrow corridors, or doorways). It was our premise that safety of patients is guaranteed without disturbing their natural walking patterns. Safety can be ensured with a harness that supports part of the patient’s body weight and protects them from stumbling while walking on a motorized treadmill. Evoking the FOG phenomenon in the laboratory is a challenging task. A recent experimental study successfully evoked FOG in patients using obstacles that appeared suddenly on the treadmill [5]. However, that study had a major limitation in that FOG was evoked during a situation that does not simulate real life FOG episodes. In real life, obstacles are used as external cues to overcome FOG [2]. Situations that commonly cause FOG in real life are narrow spaces such as doorways or spaces between furniture or more elaborate mobility tasks such as turning, starting or stopping movements [6]. Another limitation of this study is that although the kinematics and kinetics of the treadmill walking are proven to be similar to those of overground walking [7, 8], the control of speed on typical treadmill walking is fundamentally different from real world (or overground walking). In the real world, one voluntarily initiates and changes walking speed, whereas on a regular treadmill, the treadmill controls walking speed. If we are to simulate real-life events that provoke FOG, it is necessary to allow subjects to naturally and voluntarily initiate and change their walking speed while the treadmill responsively follows their intention.
This study aims at implementing a novel approach to the traditional Body Weight Support Treadmill (BWST) system allowing the subject to voluntarily control the treadmill speed. Along with our speed adaptation controller we have integrated a Virtual Reality (VR) system. There has been previous research showing different ways to control treadmill speed. In a BWSTI with a robotic exoskeleton, interaction force between the robotic device and the subject’s limb could be used to control the treadmill speed [9]; however, the physical interaction between subjects and the robot may interfere with implementing walking environment that allow patients to evoke FOG in a natural way. Others developed treadmill speed adaptation controller based on subject’s body positions measurement [10–12]. These studies have used pelvis [10, 11] or head [12] position in space for a feedback controller to keep the subject’s body near a reference position (typically set around the middle of treadmill or at the initial position of the subject). However, the problem with these approaches is that it either requires extra long treadmills to accommodate for delays in speed adaptation or a feedback controller to be tuned for more responsive reaction to subject’s intention, which sometimes results in instability of whole system. We are proposing a novel approach using feedforward and feedback controllers which allow for more responsiveness without sacrificing stability. Our proposed feedforward controller accurately estimates walking speed, and our feedback controller keeps the individual near the center of the treadmill track. In previous work, we have tested healthy individuals and found that, by using maximum velocity of swing foot for walking speed estimation, the feedforward control in combination with a feedback control allowed subjects to suddenly accelerate/decelerate in a natural way, while the controller was still able to keep subjects within 0.5m range of 1.5 m long treadmill track [13].
In this paper, we tested the safety and feasibility of our feedback/feedforward control scheme in patients with FOG. We present here the preliminary findings of 3 subjects with PD and FOG who were exposed to our BWST interface in association with a VR environment.
II. Treadmill Speed Adaptation Control Algorithm
A. System Setup
An instrumented treadmill (Bertec Co., Columbus, Ohio, USA) was interfaced with a VICON Nexus motion capture system (VICON Inc., Denver, Colorado, USA). Two reflective markers were attached to the lateral sides of each foot 20 mm below the ankle joint, and another two markers were placed on posterior superior iliac spine for pelvis tracking (Fig. 1). The subject wore a harness which was hooked to a body weight support system, the ZeroG system (Aretech LLC, Ashburn, Virgina, USA). The harness stayed above the subject’s head and followed them along the walking direction while supporting a constant amount of body weight.
Fig. 1.
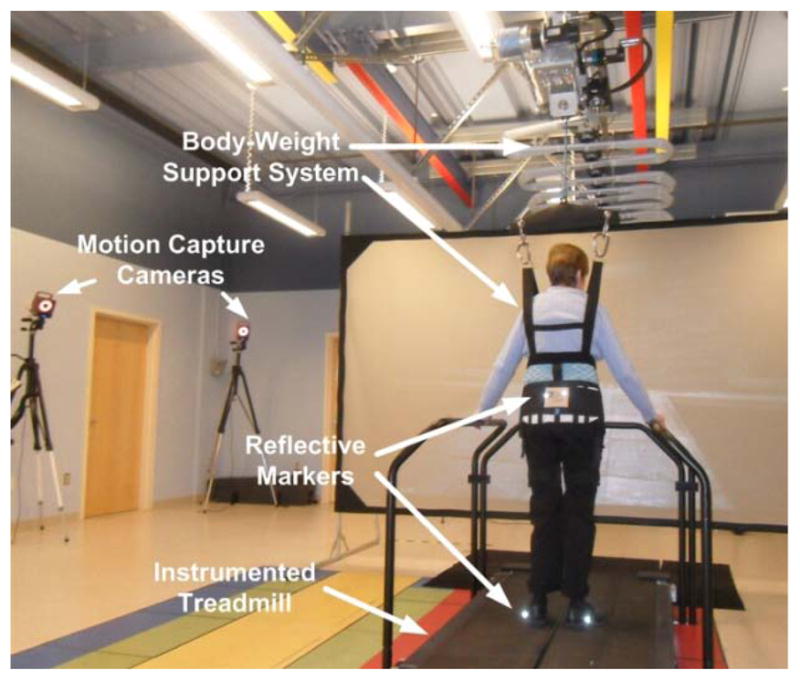
System Setup: the body-weight support treadmill interface
The VICON Nexus system captures four marker positions and sends data over the network to the treadmill controller at 120 Hz. The controller then estimates walking speed, and calculates feedback and feedforward control commands which are sent to the treadmill.
B. Treadmill Speed Adaptation Algorithm[13]
The speed adaptation controller consists of a feedforward controller and a feedback controller. In the feedforward controller, the walking speed is estimated from the maximum swing foot velocity. Assuming that the velocity profile of a swing foot during a swing phase resembles the first half period of a sine function (Fig. 2), the velocity of swing foot is represented by
Fig. 2.
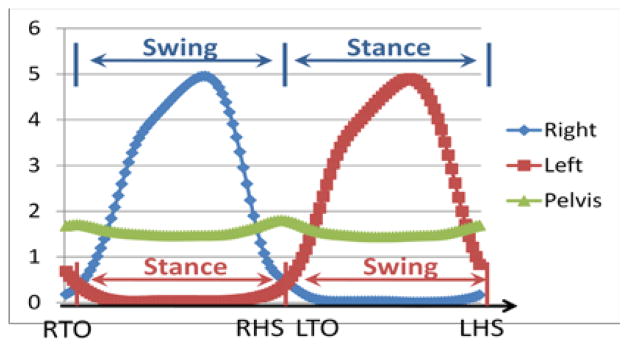
Foot velocity (right-blue, left-red) and pelvic velocity (green) while a subject walks at a constant speed. The foot velocity profile in swing phase resembles the first half period of a sine function.
| (1) |
where Vmax and T denote the maximum speed of the swing foot and swing time.
Since the distance traveled by pelvis during one step is half of the distance traveled by swing foot (Fig. 3)
Fig. 3.
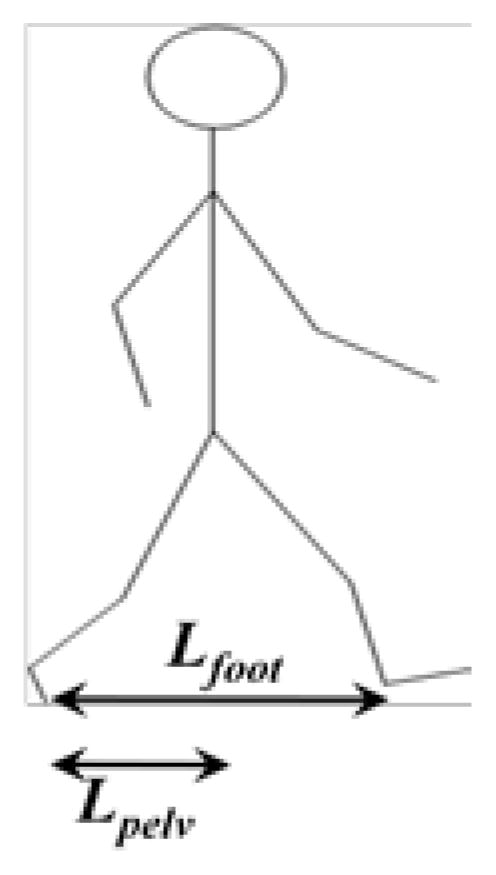
Schematic diagram showing distance traveled by foot and pelvis during one step. In a swing phase (from toe-off to heel-strike), the distance traveled by the swing foot (Lfoot) along the direction of walking is twice the distance traveled by the pelvis (Lpelv).
| (2) |
where Vavg,pelv denotes the average speed of pelvis which typically is same with the walking speed during a step. From the equations (1) and (2), we get
| (3) |
Eq. (3) applies to the overground walking and estimates walking speed from the maximum swing foot speed; however, in the treadmill walking, the equations need to be slightly modified.
When the treadmill is moving at Vtm, the swing foot velocity can be rewritten as
| (4) |
where, Vmax,tm denotes the maximum swing foot speed measured by the motion capture system when the subject walks on the treadmill. Vmax,tm is smaller than Vmax by the amount equal to the treadmill speed, Vtm. On the treadmill, the distance the subject walked during one step equals to Vtm T. Hence, Eq. (3) changes to
| (5) |
Eq. (5) estimates walking speed based on maximum swing foot speed, and updates treadmill speed in the middle of the swing phase (typically at the half of a swing phase), which makes the controller more responsive. Note that other gait parameters such as duration of stance phase [14] and average velocity of swing foot [15] could also estimate walking velocity; however, other gait parameter will not update walking velocity until one step is finished whereas the proposed method estimates at half step achieving quicker update.
In addition to the feedforward estimation, the pelvic position is used to generate a proportional feedback control command (Fig. 4). The feedback controller keeps the user near the reference position (which is usually set to the initial pelvis position), while the feedforward controller quickly estimates the walking speed. The weight factors of the feedforward and feedback controllers can be adjusted for optimal performance.
Fig. 4.
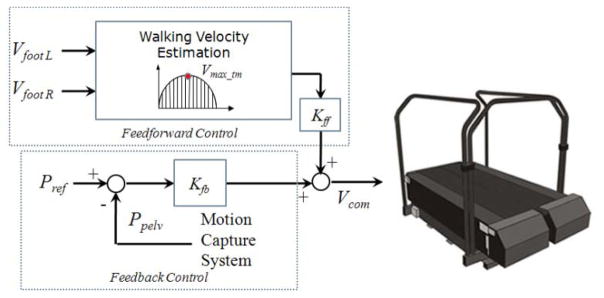
Control structure of the BWSTI
C. Integration of the BWSTI with VR System
The BWSTI was interfaced with the three dimensional VR display system (Headrehab LLC, Chicago, Illinois, USA), so that the subjects could visually perceive the virtual environment as if they were walking through it. For synchronous movement of the virtual environment, the VR display module receives the treadmill speed information at 60 Hz through the network by using TCP/IP protocol (Fig. 5).
Fig. 5.
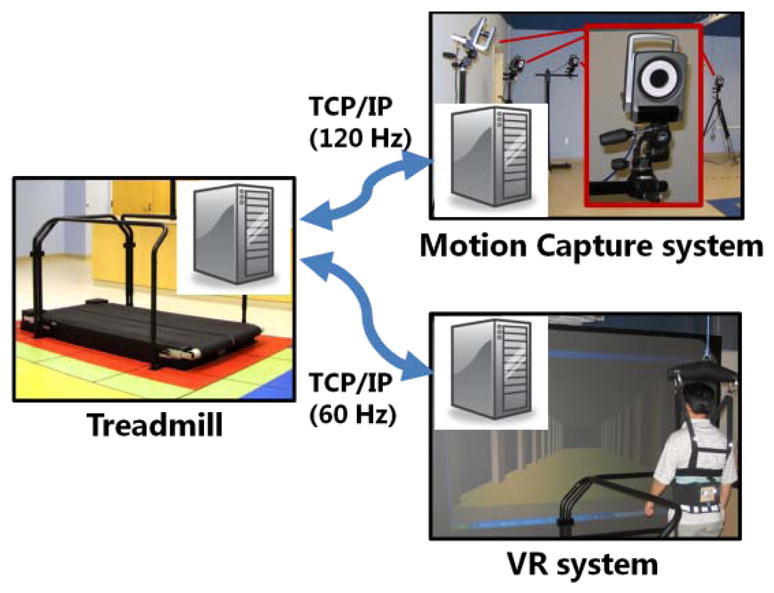
Communication structure: The motion capture system communicates with treadmill controller at 120 Hz, and the treadmill controller sends speed information to VR system at 60Hz.
III. Methods
The major purpose of this experiment was to investigate whether the speed adaptation controller and the VR system offer a safe and realistic walking environment allowing the patients to naturally walk and respond to visual stimuli. We also asked the subjects how they felt and studied reactions to different combinations of the feedforward or feedback gains.
A. Subjects
Three subjects diagnosed with PD and known to have FOG participated in the pilot experiments. All subjects gave written informed consent approved by the National Institutes of Health IRB. Average age was 63.7±2.1 yrs. Two subjects had been diagnosed with PD for five years and the other for two years. Average height and weight were 179±6.5 cm and 83.2±15.4 kg. All were tested in the off-medication condition.
B. Data Collection and Analysis
Subjects wore a ZeroG body-weight support harness which was programmed to constantly support 10 lbs of subject’s body weight. Four markers were placed on their feet and pelvis. Subjects wore goggles to accurately visualize the 3D VR display. The gains of feedback and feedforward controllers were tuned while they walked three minutes at different speeds. Subjects were then instructed to complete multiple one-minute walking trials to become familiar with the BWST and the VR display. After practice, they walked at their preferred speed (they were also able to stop and speed up voluntarily as they felt necessary) while different types of 3D corridors which may or may not elicit FOG were displayed.
IV. Results
All subjects could walk safely at their own preferred speed. They were also able to accelerate and decelerate as they wanted.
According to patients’ feedback, it was observed that decreasing feedforward gain made it difficult to initiate walking; therefore, we set the feedforward gain (Kff in Fig. 4) to unity – using the exact estimated speed without scaling it. The feedback controller guarantees that subjects stay near the reference position. Larger Kfb makes the feedback controller react quicker to move the subject back to the reference position. However, a Kfb greater than the stable margin causes instability. In practice, the stable range of Kfb was determined by monitoring the fluctuation in pelvic motion. As shown in Fig. 6, the feedback gain (Kfb) greater than 0.5 keeps the subject closer to the reference position at zero. However the quick reaction caused bigger fluctuation in pelvic movement which indicates that the subject did not walk naturally or comfortably. With Kfb=0.25, the deviation from the reference position increased (Fig. 6), but the magnitude of pelvic fluctuation is decreased. Note that, even though the deviation increased with smaller Kfb, the subject stayed within 20 cm of the reference position which is small enough to keep the subject within the treadmill track.
Fig. 6.
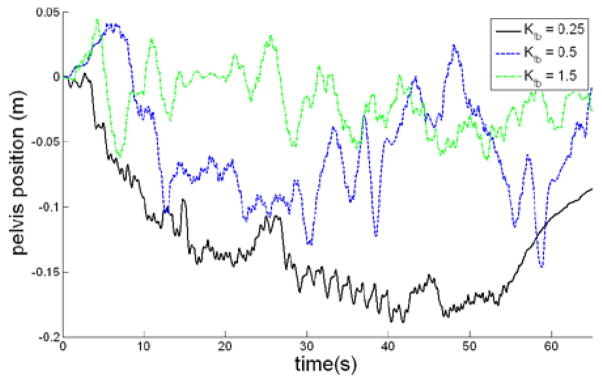
Pelvic movement along the walking direction in a 60 seconds walking trial at three different feedback gains.
According to the subjects’ feedback during the practice trials, they felt it was easier to walk with smaller Kfb; so, in the real trials, Kfb was set to 0.25 with which the feedback control term (Vfb) was much smaller than the feedforward control term (Vff) when the subject walked faster (Fig. 7). The feedback control became dominant only when the subject walked at very slow speed (<0.1 m/s) or stopped.
Fig. 7.
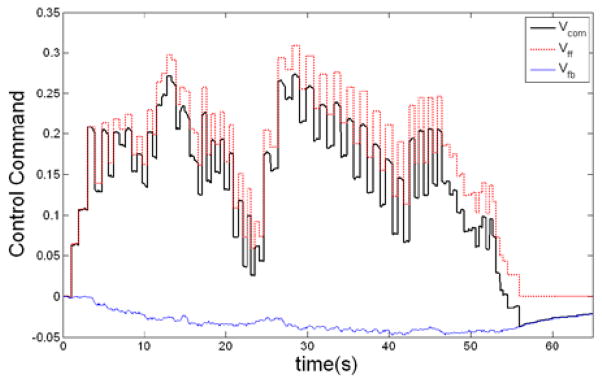
Control command profile during the 60 seconds of walking trial with Kff =1 and Kfb=0.25: (Vcom= Vff + Vfb)
Next, we observed whether FOG occurred while subjects walked on the BWST with the VR display. In the first two subjects who had PD for more than five years, FOG occurred as they approached to a virtual wall and went through narrow corridors. The other subject did not show FOG during the test. During the FOG phenomena, it was observed that the step length and walking speed decreased while the double support time increased (Fig. 8).
Fig. 8.

Temporal/Spatial Parameters from the three subjects. The upper figures show step time and step length and right figures show velocity and double support time. Three subjects walked through a corridor where a virtual wall blocked their passage about 10 meters from the initial position. The left (subject 1) and middle (subject 2) show FOG phenomena while the right (subject 3) does not.
We also found that depending on the severity of the impairment or familiarity with the treadmill, some subjects needed more practice than others to be accustomed to the new type of controller. For example, subject 3, who had more experience with treadmill exercise and who also had the least impairment was quicker to adjust to the new type of controller than the others. For the subject 1 and 2 who needed more practice trials, there was no instability observed during the test but they were hesitant to initiate walking because they were accustomed to typical treadmill walking where the treadmill drives first. These factors might have contributed for the subject not to show FOG in our system.
V. Conclusions and Discussions
The research presented in study is a novel approach to the development of a BWSTI system associated with a VR system. Our preliminary findings show that the BWSTI + VR system can safely and realistically reproduce real world overground walking conditions. In addition, our system was successfully able to evoke FOG in the laboratory, which shows this paradigm can potentially be used to investigate the causes and the underlying mechanisms of FOG in PD.
Instead of using typical treadmill platform where a treadmill drives a person to walk at a constant speed, we have implemented a speed adaptation controller for a more natural and real life-like walking. The controller allows subjects on the treadmill to initiate walking, freely change walking speed, and stop walking by themselves. The interface with a 3D VR system for synchronous display of a virtual environment allows subjects to experience walking conditions similarly to real-life conditions.
The novelty of our BWSTI + VR system is in the feedforward/feedback control structure. This is the first study to utilize this control structure for speed adaptation control of treadmill. Our feedforward controller estimates walking speed by using the maximum swing foot speed which allowed us to quickly respond to subjects’ intention. Our feedback controller keeps the subjects inside the treadmill track by moving them near the reference position (usually set near the middle of the treadmill). In addition, we have found an optimal feedforward/feedback gains for patients, which avoided sudden destabilizing body movements. Our BWSTI + VR evoked the FOG phenomenon in 2 out of 3 patients. The situations in which FOG was manifested were similar to real life situations (doors and corridor narrowing). However, no FOG was observed in subject 3, who happened to be familiar with using a treadmill and required less practice compared to the other two subjects. Therefore it is hard to distinguish whether the evoked FOG in subjects 1 and 2 was due to the unfamiliarity with the treadmill or the visual cues given to the subjects. Further investigation is necessary to clarify this issue and more importantly to explore the underlying mechanisms of FOG in PD.
Acknowledgments
This research is supported by the Intramural Research Program of NINDS and Clinical Center in NIH (protocol number 10-N-0009) and CNRM (Center for Neuroscience and Regenerative Medicine) program (grant number G1707C).
References
- 1.Giladi N, Nieuwboer A. Understanding and treating freezing of gait in parkinsonism, proposed working definition, and setting the stage. Mov Disord. 2008;23(Suppl 2):S423–5. doi: 10.1002/mds.21927. [DOI] [PubMed] [Google Scholar]
- 2.Nieuwboer A, et al. Cueing training in the home improves gait-related mobility in Parkinson’s disease: the RESCUE trial. J Neurol Neurosurg Psychiatry. 2007;78(2):134–40. doi: 10.1136/jnnp.200X.097923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Frazzitta G, et al. Rehabilitation treatment of gait in patients with Parkinson’s disease with freezing: a comparison between two physical therapy protocols using visual and auditory cues with or without treadmill training. Mov Disord. 2009;24(8):1139–43. doi: 10.1002/mds.22491. [DOI] [PubMed] [Google Scholar]
- 4.Lo AC, et al. Reduction of freezing of gait in Parkinson’s disease by repetitive robot-assisted treadmill training: a pilot study. J Neuroeng Rehabil. 7:51. doi: 10.1186/1743-0003-7-51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Snijders AH, et al. Obstacle avoidance to elicit freezing of gait during treadmill walking. Mov Disord. 25(1):57–63. doi: 10.1002/mds.22894. [DOI] [PubMed] [Google Scholar]
- 6.Okuma Y, Yanagisawa N. The clinical spectrum of freezing of gait in Parkinson’s disease. Mov Disord. 2008;23(Suppl 2):S426–30. doi: 10.1002/mds.21934. [DOI] [PubMed] [Google Scholar]
- 7.Alton F, et al. A kinematic comparison of overground and treadmill walking. Clin Biomech (Bristol, Avon) 1998;13(6):434–440. doi: 10.1016/s0268-0033(98)00012-6. [DOI] [PubMed] [Google Scholar]
- 8.Riley PO, et al. A kinematic and kinetic comparison of overground and treadmill walking in healthy subjects. Gait Posture. 2007;26(1):17–24. doi: 10.1016/j.gaitpost.2006.07.003. [DOI] [PubMed] [Google Scholar]
- 9.von Zitzewitz J, Bernhardt M, Riener R. A novel method for automatic treadmill speed adaptation. IEEE Trans Neural Syst Rehabil Eng. 2007;15(3):401–9. doi: 10.1109/TNSRE.2007.903926. [DOI] [PubMed] [Google Scholar]
- 10.Minetti AE, et al. A feedback-controlled treadmill (treadmill-on-demand) and the spontaneous speed of walking and running in humans. J Appl Physiol. 2003;95(2):838–43. doi: 10.1152/japplphysiol.00128.2003. [DOI] [PubMed] [Google Scholar]
- 11.Lichtenstein L, et al. A feedback control instrument for treadmill locomotion in virtual environments. ACM Trans. Applied Perception. 2007;4(1) doi: 10.1145/1227134.1227141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Souman JL, et al. Making virtual reality real: perceptual evaluation of a new treadmill control algorithm. ACM Trans. Applied Perception. 2010;7 [Google Scholar]
- 13.Yoon JW, Damiano DL, Park H-S. Walking Velocity Estimation by Swing Foot Velocity and Its Application to Velocity Adaptation Control of a Treadmill. International Conference on Applied Bionics and Biomechanics; 2010. [Google Scholar]
- 14.Noma H, Miyasato T. Design for locomotion interface in a large scale virtual environment ATLAS: ATR locomotion interface for active self motion. IEEE 7th Annual Symposium on Haptic Interface for Virtual Environment and Teleoperated Systems; Los Alamitos, CA. 1998. [Google Scholar]
- 15.Yoon JW, Ryu J. A novel locomotion interface with two 6-dof parallel manipulators for human walking on various virtual terrains. International Journal of Robotics Research. International Journal of Robotics Research. 2006;27(07):689–708. [Google Scholar]