

Dear Editor,
Abnormal Uterine Bleeding (AUB) affects 10-30% of menstruating women at any one time and may occur at some time during the perimenopause in up to 50% of women.[1] We would like to project the circumstances peculiar to the hill state of Himachal Pradesh, which at times necessitate management decisions to be taken because of peculiar topographic and geographical location of this state. Out of 20,784 new patients who attended the gynecology outpatient department at Kamla Nehru Hospital, Indira Gandhi Medical College, Shimla from November 2011 to October 2012, 3554 women (17.09%) presented with complaints of AUB. Most of the women in reproductive age group had irregular cycles and excessive flow during periods. Women at the extreme of reproductive age presented mainly with anovulatory cycles. Statistics of AUB in Kamla Nehru State Hospital, Indira Gandhi Medical College, Shimla are: Menorrhagia: 812 (3.9%), puberty menorrhagia: 92 (0.44%), metrorrhagia: 1301 (6.25%), oligomenorrhea: 215 (1.03%), hypomenorrhea: 138 (0.66%), polymenorrhea: 267 (1.28%), anovulatory cycles including perimenarchal: 151 (0.72%) and perimenopausal: 295 (1.41%), post-coital bleeding: 20 (0.09%), post-menopausal bleeding: 130 (0.62%) and leiomyoma: 133 (0.63%).
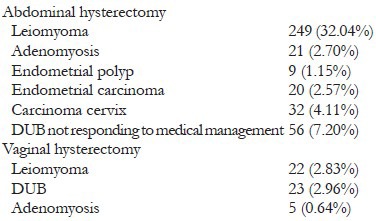
Incidence of hysterectomy: Total 777 hysterectomies, abdominal and vaginal, were performed during November 2011 to October 2012 for gynecological causes, both benign and malignant at Kamla Nehru State Hospital. 453 (58.3%) were attributable to AUB. Rest of the statistics for hysterectomies in our institute include:
WHY HYSTERECTOMY?
Hysterectomy is one of the most prevalent surgeries worldwide. Menorrhagia is the primary indication and is not always a response to an anatomical disease. New and improved alternatives are increasingly employed for this indication and are responsible for the fall in the rate of hysterectomies performed in the last decade include endometrial ablation, the progestin intrauterine device, myomectomy and uterine embolization. These alternatives can reduce the need for anesthetics, long hospital stays and lengthy recovery times. Unfortunately, we in Shimla are still devoid of all these new alternatives and are still managing AUB with drugs and hysterectomies. There are several causes for this; some of them are enlisted below:
Health care delivery system and geographic background: Shimla is surrounded by hills all around. Due to hilly terrain it is difficult for patients to reach specialists sitting in district Hospitals or Medical Colleges for their regular follow ups. Hence to start conservative alternatives is impossible for the patients coming from far flung areas.
Climate and weather: Shimla district experience excessive rains in the rainy season and most of the areas are snow clad in the winters. These conditions make accessibility of patients to the health institutes poor. Again a significant factor why follow-up is poor for the patients residing in Shimla district, thus making hysterectomy one of the primary management choices for AUB.
Socio-economic status: Most of the patients are from a rural background with low socio-economic status generally prefer surgical method as cost effective as it is difficult for them to afford long and costly conservative treatments. Hysterectomy appears to be cost effective when compared with alternative conservative therapies.
Education: Education level of the patients attending the gene out patient department is generally extremely low. Most of them are poorly educated and want themselves to get rid of the disease completely. These kinds of patients are also less compliant and are more prone to side effects of sexual steroids, which make hysterectomy their favorite choice. Not only this, these patients are full of myths regarding their condition. They are worried that if started with medical management for AUB could lead to the development of cancers.
Health seeking behavior: Since most of the patients belong to rural background, they prefer to tolerate their reproductive ill health. Even if they decide to seek treatment they either manage themselves or have been approaching unqualified health personal. Such perceptions and beliefs constitute a “lay health culture” which would raise their morbidity in the form of severe anemia, thus leading to terminal surgical treatment in the form of hysterectomy. The other half of women who did not seek treatment opine that it would bring disgrace on them if they disclosed their illness.
Limitations of equipment or supplies: Hysteroscopic endometrial resection or newer endometrial ablation procedures are not available because of limitation of acquisition costs and support personnel to maintain the equipment in government set up. Limitations of equipment or supplies directly impact the ability of health-care practitioners to implement the systematic approaches. Lack of resources, therefore, often lead to empirical treatments including hysterectomies.
Surgeon's training with respect to the different possible approaches to manage AUB: Continuous training programs must be offered to residents and gynecologic surgeons with the intention of developing effective guidelines for the management of AUB and other more conservative alternatives that can be offered to patients.
REFERENCE
- 1.Livingstone M, Fraser IS. Mechanisms of abnormal uterine bleeding. Hum Reprod Update. 2002;8:60–7. doi: 10.1093/humupd/8.1.60. [DOI] [PubMed] [Google Scholar]