

Abstract
Background:
Main suggested theories about patients’ adherence to treatment regimens recognize the importance of motivation in positive changes in behaviors. Since cardiac diseases are chronic and common, cardiac rehabilitation as an effective prevention program is crucial in management of these diseases. There is always concern about the patients’ adherence to cardiac rehabilitation. The aim of this study was to describe the motivational factors affecting the patients’ participation and compliance to cardiac rehabilitation by recognizing and understanding the nature of patients’ experiences.
Materials and Methods:
The participants were selected among the patients with cardiac diseases who were referred to cardiac rehabilitation in Isfahan Cardiovascular Research Center, Iran. The purposive sampling method was used and data saturation achieved after 8 semi-structured interviews.
Findings:
The three main concepts obtained from this study are “beliefs”, “supporters” and “group cohesion”.
Conclusions:
In cardiac rehabilitation programs, emphasis on motivational factors affects the patient’s adherence. It is suggested that in cardiac rehabilitation programs more attention should be paid to patients’ beliefs, the role of patients’ supporters and the role of group-based rehabilitation.
Keywords: Heart diseases, rehabilitation, motivation, patient compliance, qualitative research
INTRODUCTION
In recent years, one of the main challenges of human society is dealing with life-style related conditions such as cardiovascular diseases (CVD). Based on information from American Heart Association, heart diseases remain as a first cause of mortality in the world.[1] CVD has significant potentials to affect all dimensions of patients’ lives, and consequently, they can reduce the patients’ quality of life (QOL).[2,3] Therefore, like other chronic conditions, progression of cardiac diseases, by improving the health promotion and disease prevention programs, should be decreased.[4] Furthermore, cardiac patientss must have a long-standing commitment to complex regimens that highlight patient self- management.[5] Comprehensive cardiac rehabilitation (CR) as a prevention program which affect all aspects of patients’ lives, involve a multidisciplinary team, and nurses as core members of this team have always had essential roles.[3,6,7] These programs designed to prevent the diseases’ progression, to promote patients’ QOL and to decrease the disease-related disabilities and mortality. Despite all the efforts and emphasis that have been put on prevention programs by the health care professionals, several barriers have been limiting the success of these programs. Based on a lot of reports, tertiary prevention of coronary heart diseases is often inadequately managed and only a small group of patients with heart diseases benefit from it.[7] Although, so far lots of studies focused on this problem and also several factors related to non-adherence have been found, but patient’s adherence to CR remain low.[8,9] These studies have revealed that due to multidimensional characteristics of CR, various factors can affect patients’ compliance.[8] Despite all of these findings, efforts to recognize socio-demographic or clinical predictors, which influence the patients’ attendance, have not been successful. In contrast, individuals’ viewpoints and patient’s perceptions about their diseases seems to play a pivotal role in health behaviors such as medications compliance and the level of patients’ functioning.[9] The qualitative studies allow the researchers to consider all of these indeterminate interventional factors and conditions jointly. Although motivation does not have a fixed definition and it is a debatable term, it generally means the internal force that instigates one to engage in a particular behavior. Many studies refer to motivation as a significant psychological factor that correlates with patients’ treatability, and they show that however motivation is not a statistical predictor, it can reflect the patients’ readiness for changes.[10] In other words, being aware of the factors that motivate behavioral change is essential to every health promotion efforts.[11] All of the common theories and models that are related to patient adherence to treatment regimen and healthy behaviors such as Social learning theory (social cognitive theory), Theory of Reasoned Action/Theory of Planned Behavior, Protection Motivation Theory, Health Belief Model, Self- Regulatory Model of Illness, Trans theoretical Model and Precaution Adoption Process Model recognize the value of motivation to change behavior and emphasize the importance of strengthening the factors or processes that prompt behavioral change.[5] Therefore, identifying motivational factors that motivate patients’ adherence to CR program can be used to improve the CR acceptance and compliance in cardiac patients.
Aims
The aim of this study is also to describe the motivational factors behind the patients’ participation in CR programs by deep understanding of participants’ experiences in attending CR programs.
MATERIALS AND METHODS
Participants
Study participants were selected among CR participants referred to Isfahan Cardiovascular Research Center from Oct. 2006 to Dec 2007. A purposive sampling method was used. Inclusion criteria were: having history of cardiac accidents, participating in CR program in Isfahan Cardiovascular Research Center, and completing all of the counseling sessions and at last 5 sessions of physical exercises. The patients with disability in verbal communication, unstable conditions, and/or reluctance for participation were excluded. After 8 semi-structure interviews the data saturation was achieved. The 8 participants included 6 men and 2 women who were between 49 to 66 years old. Among participants, 7 of them had undergone coronary artery bypass graft, and 1 had had angioplasty. The minimum number of rehabilitation sessions attended by these participants was 11 and the maximum was a 3-year attendance. The participants’ level of education varied from less than a high school diploma to PhD.
Rehabilitation Setting
The CR center mentioned in this research is a part of Isfahan Cardiovascular Research Center that is linked to Isfahan University of Medical Sciences in Iran. This rehabilitation center provides variety of services to its cardiac patients such as dietary counseling, smoke cessation counseling, stress management classes, first aid and resuscitation classes, heart health classes, diagnostic and paraclinic facilities and exercise rooms. The patients referred to the center by hospitals or physicians enrolled in the program, and they completed a counseling session. Then, they were advised to participate in a minimum of 20-session in-group physical exercise course, which was monitored by nurses. Each exercise session lasted for 2 hours, and patients’ vital signs were monitored by cardiac monitors. The cost of one rehabilitation course was about $100-150, and some of the health insurances cover a part of it.
Procedure
This research is a qualitative study with descriptive phenomenological approach. Data gathering was done using deep semi-structure interviews directed with open- ended questions. Each interview lasted between 30 to 60 minutes, and it took place in a private place before or after participants’ exercise based on patients’ preference. After selection of 8 participants based on inclusion and exclusion criteria and obtaining consent from them, the face-to-face interviews, deep and semi-structured interviews were done, and the interviews were recorded by audiotape. The focus of these interviews was on the “experience of heart event”, “life quality after event”, “the reason for compliance and attendance” and “effective experiences related to participation in CR”.
Ethical considerations
University Research Board approved the study. The participants were informed on the study both orally and in writing and were assured of the privacy and confidentiality. They were assured that they can leave the study at any time.
Analysis Framework
After each interview and listening to the recorded interviews for several times by researchers, the data were transcribed verbatim and they were analyzed base on Collizzi method. Each written interview was read and reviewed over and over, and noteworthy statements were recognized. Then, these statements were formulated based on similarity of their meanings. These statements and terms were rechecked and were approved by participants and were corrected if needed. Then, those terms that had a parallel meaning were grouped as a sub-theme. After that, major themes were extracted from coordinated sub- themes. Finally from 8 sub-themes, 3 main themes were formed that were: “beliefs”, “supporters” and “group cohesion”, all of which reflected a comprehensive view of motivational experiences of CR. (Figure 1)
Figure 1.
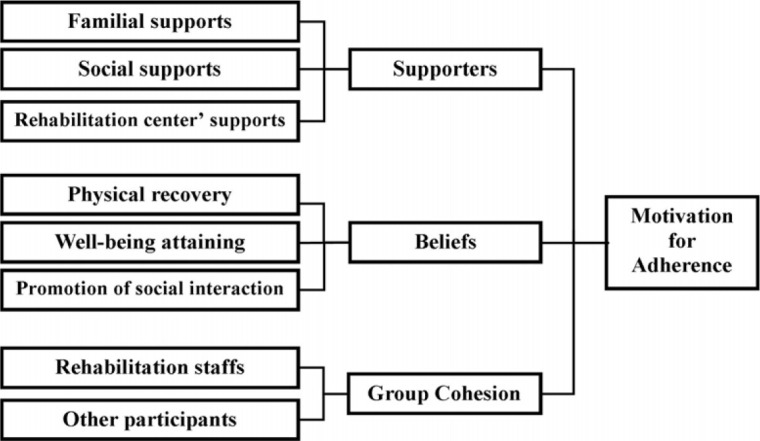
Sub-themes and themes of motivation for adherence to cardiac rehabilitation
In qualitative studies, credibility, dependability, conformability and transferability are 4 criteria to evaluate the data trustworthiness.[12] In this study, to achieve these criteria, engaging in data collection and data analysis for near a year by researchers, peer-debriefing by people who did not participate in the study, rechecking the extracted meanings with the participants after data analysis, inquiry audit, and bracketing were considered.
FINDINGS
Base on the data analysis in this study, three obtained themes were “beliefs”, “group cohesion”, and “supporters”. These themes reflect the patient’s apprehension of program’s values, the encouraging role of group exercises, and the helpful and supporting roles of families, and rehabilitation team that could influence the participants’ experiences of rehabilitation programs.
Beliefs
Patients’ faith and beliefs in the positive effects of CR on their recovery and on maintenance of their health in all aspects of their lives play a pivotal role in patients’ motivation in program acceptance and adherence. This strong trust has led to the formation of a psychological need to CR as a source of well living.
When participants accept to pay rehabilitation fees, it reveals that they believe in it, and this helps them to pay the fees more easily.
“Yes, it is expensive for me, but I think if patients really understand the value of rehabilitation and its positive effects on their health, they would easily invest in it. (pn.1)
Thus believing in the importance of CR for their health, results in this belief that non-attendance and non- adherence to such programs is equal to being at risk.
“It had been useful for me. I continue it because I see and feel huge differences between my condition now and my condition on my first days here. I’m doing okay because I take this program seriously and I follow the instructions very well, my son has the same condition as me but unlike me, he does not attend this program and does not take his condition seriously, so he has been admitted to the hospital many times”. (pn.5)
The formation of such beliefs in the patients has resulted in the continuation of the instructions and activities of the rehab even when the patients are not in the rehabilitation center.
“When I don’t come here, I certainly go for a walk because I don’t want to have an interruption in my program”. (pn.6)
“I can do it like everybody” is a corner stone of each rehabilitation program that if the participants believe in it, it can result in goal attainment. This belief directs the participants from dependency to self-assurance. Therefore, it is very important in patients’ motivation.
“What happens when I step on the treadmill? I realize that I can regain the ability that I lost due to my illness …” (pn.5)
Group Cohesion
Group cohesion reflects the interaction, empathy and sympathy that are formed between participants themselves and participants and the members of rehabilitation team, and it acts as an important motivational factor. An emotional, friendly, and joyful environment that is shaped by participants and health staff in these programs motivate each member to participate and contribute even more.
“Here, we all have same kind of problems, same concerns and same world…here I see other participants are like me, and I feel I ’m like them…when I exercise alone, I easily give up …but when I am here and exercise with the other participants, I enjoy it and I feel powerful…” (pn.3)
“At home, I’m alone in a small place, I have exercise equipment, and I can listen to music while exercising like here, but it is not just that, here I can talk to others and I love it. Here when I see others who are like me, and they can exercise very well I am not afraid of exercising anymore …” (pn.7)
The encouraging behavior of rehabilitation team members also can affect this friendly and motivational setting positively and encourage the participants to stick to the program.
“Here, the rehabilitation staffs are very good, they are often pleasant and they encourage the participants to participate, I like them… I have asked the staff to give me a copy of the music that they play for us here, so when at home, I can feel I am in this environment and I stick to my exercise, but I have to tell you that I get bored very easily and I postponed my exercise to tomorrow, so I think the group exercise is very effective…” (pn.8)
Supporter
This concept extracted from the constructive role of familial, social and rehabilitation team support on informant’s acceptance. The participant’s family role includes helping and encouraging him/her to complete the rehabilitation program.
“My wife is my main supporter that cooks for me, she cooks for me particularly” (pn.4)
The social support in form of advising the clients to participate in rehabilitation especially by health care team, introducing the rehabilitation centers in hospital and media, informing the people about the CR benefits in media, and helping the patients to pay the cost by sufficient insurance have motivational role for participants.
“My health service insurance accepted nearly 90% of my rehabilitation cost and helps me for participation …” (pn.2)
“My doctor referred me to here and he strongly advises me to continue my participation…” (pn.6)
Typically, the patients’ support arises from rehabilitation center as a motivational factor in participants’ program adhesion is marked by; these supports in form of rigor supervising during the patient’s exercise, quick support in emergent situations, tailored program base on participant conditions, clinician accessibility, persistence to program completion, exercise equipment, music and other facilities such as recreation with other participants, patient support in paying the rehabilitation cost, and involving the family of patients in the program play a pivotal role in formation of participants motivation.
“The nurses and physicians are here, we have confident to them, and we exercise under their supervision…” (pn.5)
“The center has a special discipline that is compulsive…all the parts of this center such as medicine, nutrition, psychology and other parts are associated, but in other exercise centers, only an amateur staff supervise the participants…” (pn.4)
DISCUSSION
The gained experiences from participating in the cardiac rehabilitation internally affect the participants which is a powerful motivating factor to follow the program intensively. Nearly all of the suggested theories and models about patient’s adherence to treatment regimens recognize the importance of motivation in positive changes in patients’ behaviors.[5] The foundation of this internal force is on the patient interaction with different aspect of CR program characteristics, with family members, society and rehabilitation team.
The motivational role of patient’s belief and credence
The physical, psychological and social effects of rehabilitation participation led to reconstruction of patient attitude and belief about possibility of overcoming the healthy needs by involving his/herself in this program. Base on participation experiences, the patient toward maintenance of own health in all dimensions and consequently toward promotion of own quality of life internalize values of involving to CR. This reconstructed belief and credence about CR directs the patient’s behavior in form of self-control and self-directions that improve the participation and adherence.[13–15] Base on well-known Locus of Control theory, people who are high in internal locus of control believe health rewards are contingent on healthy behavior.[5] Rehabilitation adherence is predicted positively by autonomous motivation (β = 0.64, p < 0.05) and negatively predicted by controlled motivation (β = -0.28, p < 0.05).[16]
Learning about healthy life style, recognizing one’s own weakness and ability, and the recovery of physical capability in performing activities are effective results of participation affecting psychosocial aspect of patient’s life that consequently improve the patient’s quality of life.
The positive changes in patient’s attitude which is reflected in this phrase “my ability is just like the other healthy people” help the patient to surmount the disease induced limitations. Clark et al. based on a qualitative study notifies that the patients who do not participate in CR program do not recognize their own physical limitation boundary, so often in daily living activities they experience debilitative fear and doubt.[17] On the other hand, the positive effects of rehabilitation on patient’s health can be influenced by the level of access to social assurance and patient capacity to recognize, interpret and make judgments about their own physical limitations.[17] Participation in CR program improves all aspects of patients life.[18,19]
The motivational role of synergism in group cohesion
Foundation of “group cohesion” is upon its synergic effect. Synergism refers to improving the ability arising from working together, so this factor can positively direct goal achievements. Synergic effect in group-based exercise and doing the program together in CR can play a motivational role that improves the adherence. Group cohesion has shown a positive correlation with adherence in some studies.[5] Working and interacting together generates the empathy and sympathy between the participants. Emotional dependencies that are shaped through group cohesion motivate more commitment in participants. The participants find themselves through a congruent group with similar needs, conditions, and also purposes. Therefore, each gained positive experience can be shared between them and can affect their goal achievement. Everyone who is feeling the ability in response to rehabilitation’s participation transmit their feeling to other participants.[20] The members of group- based CR move from “be a foreign” to “be a member”, they gain a common identity arising from interaction with other participants and rehabilitation staffs which can encourage their participation, decrease their fears, and promote their confidence.[17,21,22]
The role of supporter to shape the patient’s motivation
Participant’s supporters that may be including family members and relatives, friends, members of rehabilitation team, other members of health care team, other patients, social organization and etc. are a valuable source for changing patient’s behaviors.
Everyone directly and continually interacts with his/her environment and also for upholding of internal and external balance requires that. If interaction is supportive, it can help the patient’s development. And factors that help the patient’s development can play a motivational role. For CR participants, the feeling of being supported can have a motivational function to program adherence. The related studies revealed that patient’s interactions with treatment team members including administrative staff and nurses influence adherence,[5] and also showed that across referred patients to CR, who have more support also have more participation and adherence.[23]
The supportive role of family members especially spouses that is a powerful motivational factor to program adherence is reflected in form of helping and encouraging participant to more commitment to CR.[24–26]
The value of social supports in stimulating the participants to program allegiance implies that the cardiac patients for active participation and compliance need to be informed about the importance and the necessity of CR by media, hospital and medical centers and also must be referred to CR in correct time by physicians or other medical team members.[3,23,27,28]
In addition, the patients should be financially supported by organizations and social institutes such as insurance.[29,30] Also existing evidences reveal that physician influence and social support have been stronger and consistent correlates of physical activity level and adherence.[5]
The quality and quantity of services that is provided by rehabilitation centers can prompt participants for following the program intensely. The participants must be reassured that the rehabilitation centers can meet all of their needs about cardiac health. And also they need to be reassured about adequate expertise and experience of CR staffs that monitor participants’ condition through exercise. Doing exercise under supervision of well-trained staffs reduce participant’s fear and doubt. Studies showed that through initial steps of exercise the CR participants require more attention and supervision from rehabilitation staffs.[1,7,9] Studies also mentioned that CR programs that is tailored individually and planned comprehensively can be more adopted by participants.[31,32] Existing evidences also emphasize on necessity of staffs’ positive attitude toward CR,[15] and also stress on importance of arranging a happy and respectful climate in rehabilitation’s site. The CR center should be well prepared with exercise equipment, medical and emergency facilities, and location’s condition.[33] Involving the family members in participant’s CR program is an important responsibility and must be considered by all CR centers.[34,35]
CONCLUSION
This study carried out in Isfahan CR center, so the type and quality of delivered services by this center indisputably can affect the results of this study. Thus the results should be applied with these considerations. However the core concepts in this study are well supported by findings of other studies but carrying out the similar studies with both quantitative and qualitative approach on all aspects of CR process are needed to identify all factors affecting patients’ participation and attendance.
The findings of recent study show that during the performing of CR program, emphasizing on and considering to factors that promote the patients’ participation and adherence based on motivational effects can enhance the chance of CR goals achievement. The patients should be informed and referred to CR by all related sources, and need to be supported by related social institutes, the CR centers must be provided with a variety of facilities and specialties, and also should involve the patient’s family in performing the program. Along with satisfaction of utilizing CR facilities, created empathy and sympathy in group cohesion lead to form patient’s faith in CR as health maintenance way and can motivate patient to program participation and adherence. Since patients with high level of motivation accept the CR as a main way in achieving recovery and actively participate and adherence to it.[36]
Therefore for appropriately achieving the goals of CR program the researchers suggest that health care providers pay more attention to restructuring the patient’s belief and attitude as modifiable factors[37] and also consider patient’s support and group-based program as effective factors in motivating CR adherence.
ACKNOWLEDGMENT
The authors acknowledge the valuable advices of Mr. Mohsen Rafieian. We would like to thank all study participants and Isfahan Cardiovascular Research Center staffs, and also Dr. Atefeh Azad and Mrs. Zahra Zare for their contribution in providing this article. We also extend our gratitude to Isfahan University of Medical Sciences for financial support.
Footnotes
Research Article of Isfahan University of Medical Sciences, No: 385002
Source of Support: Isfahan University of Medical Sciences
Conflict of Interest: None declared.
REFERENCES
- 1.Rosamond W, Flegal K, Furie K, Go A, Greenlund K, Haase N, et al. Heart disease and stroke statistics--2008 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2008;117(4):e25–146. doi: 10.1161/CIRCULATIONAHA.107.187998. [DOI] [PubMed] [Google Scholar]
- 2.Chan DS, Chau JP, Chang AM. Acute coronary syndromes: cardiac rehabilitation programmes and quality of life. J Adv Nurs. 2005;49(6):591–9. doi: 10.1111/j.1365-2648.2004.03334.x. [DOI] [PubMed] [Google Scholar]
- 3.Tod AM, Lacey EA, McNeill F. ‘I’m still waiting: barriers to accessing cardiac rehabilitation services. J Adv Nurs. 2002;40(4):421–31. doi: 10.1046/j.1365-2648.2002.02390.x. [DOI] [PubMed] [Google Scholar]
- 4.KARCH AM, Smeltzer SC, Bare GG, Hinkle JL, Cheever KH. Brunner & Suddarth’s Textbook of Medical-Surgical Nursing. 11th ed. Philadelphia: Lippincott Williams & Wilkins; 2007. [Google Scholar]
- 5.Bosworth HB, Oddone EZ, Weinberger M. Patient Treatment Adherence: Concepts, Interventions, And Measurement. New York: Routledge; 2005. [Google Scholar]
- 6.Fridlund B. The role of the nurse in cardiac rehabilitation programmes. Eur J Cardiovasc Nurs. 2002;1(1):15–8. doi: 10.1016/S1474-5151(01)00017-2. [DOI] [PubMed] [Google Scholar]
- 7.Clark AM, Barbour RS, McIntyre PD. Preparing for change in the secondary prevention of coronary heart disease: a qualitative evaluation of cardiac rehabilitation within a region of Scotland. J Adv Nurs. 2002;39(6):589–98. doi: 10.1046/j.1365-2648.2002.02328.x. [DOI] [PubMed] [Google Scholar]
- 8.Carlon R, Maiolino P. Cardiac rehabilitation and secondary prevention. Monaldi Arch Chest Dis. 2003;60(4):321–3. [PubMed] [Google Scholar]
- 9.Cooper A, Lloyd G, Weinman J, Jackson G. Why patients do not attend cardiac rehabilitation: role of intentions and illness beliefs. Heart. 1999;82(2):234–6. doi: 10.1136/hrt.82.2.234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Sainsbury L, Krishnan G, Evans C. Motivating factors for male forensic patients with personality disorder. Crim Behav Ment Health. 2004;14(1):29–38. doi: 10.1002/cbm.558. [DOI] [PubMed] [Google Scholar]
- 11.Fleury J, Sedikides C. Wellness motivation in cardiac rehabilitation: the role of self-knowledge in cardiovascular risk modification. Res Nurs Health. 2007;30(4):373–84. doi: 10.1002/nur.20225. [DOI] [PubMed] [Google Scholar]
- 12.Polit DF, Beck CT. Nursing Research: Principles and Methods. 7th ed. Philadelphia: Lippincott Williams & Wilkins; 2004. [Google Scholar]
- 13.Berkhuysen MA, Nieuwland W, Buunk BP, Sanderman R, Rispens P. Change in self-efficacy during cardiac rehabilitation and the role of perceived overprotectiveness. Patient Educ Couns. 1999;38(1):21–32. doi: 10.1016/s0738-3991(98)00115-3. [DOI] [PubMed] [Google Scholar]
- 14.Beswick AD, Rees K, Griebsch I, Taylor FC, Burke M, West RR, et al. Provision, uptake and cost of cardiac rehabilitation programmes: improving services to under-represented groups. Health Technol Assess. 2004;8(41):iii–x, 1. doi: 10.3310/hta8410. [DOI] [PubMed] [Google Scholar]
- 15.Jackson L, Leclerc J, Erskine Y, Linden W. Getting the most out of cardiac rehabilitation: a review of referral and adherence predictors. Heart. 2005;91(1):10–4. doi: 10.1136/hrt.2004.045559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Chan DK, Lonsdale C, Ho PY, Yung PS, Chan KM. Patient motivation and adherence to postsurgery rehabilitation exercise recommendations: the influence of physiotherapists’ autonomy-supportive behaviors. Arch Phys Med Rehabil. 2009;90(12):1977–82. doi: 10.1016/j.apmr.2009.05.024. [DOI] [PubMed] [Google Scholar]
- 17.Clark AM, Whelan HK, Barbour R, MacIntyre PD. A realist study of the mechanisms of cardiac rehabilitation. J Adv Nurs. 2005;52(4):362–71. doi: 10.1111/j.1365-2648.2005.03601.x. [DOI] [PubMed] [Google Scholar]
- 18.Aude T, Hill PD, Anderson MA. Quality of life after participation in a rural phase II cardiac rehabilitation program. J Nurs Care Qual. 2006;21(1):56–62. doi: 10.1097/00001786-200601000-00012. [DOI] [PubMed] [Google Scholar]
- 19.Kardis P, Bruce A, Michaels J, Barnett SD. Quality-of-life changes following the completion of phase II cardiac rehabilitation. J Nurs Care Qual. 2005;20(2):161–6. doi: 10.1097/00001786-200504000-00012. [DOI] [PubMed] [Google Scholar]
- 20.Clark AM, Barbour RS, White M, MacIntyre PD. Promoting participation in cardiac rehabilitation: patient choices and experiences. J Adv Nurs. 2004;47(1):5–14. doi: 10.1111/j.1365-2648.2004.03060.x. [DOI] [PubMed] [Google Scholar]
- 21.Midtgaard J, Rorth M, Stelter R, Adamsen L. The group matters: an explorative study of group cohesion and quality of life in cancer patients participating in physical exercise intervention during treatment. Eur J Cancer Care (Engl) 2006;15(1):25–33. doi: 10.1111/j.1365-2354.2005.00616.x. [DOI] [PubMed] [Google Scholar]
- 22.Mooney M, Fitzsimons D, Richardson G. No more couch-potato Patients’ experiences of a pre-operative programme of cardiac rehabilitation for those awaiting coronary artery bypass surgery. European Journal of Cardiovascular Nursing. 2007;6(1):77–83. doi: 10.1016/j.ejcnurse.2006.05.002. [DOI] [PubMed] [Google Scholar]
- 23.King KM, Humen DP, Smith HL, Phan CL, Teo KK. Psychosocial components of cardiac recovery and rehabilitation attendance. Heart. 2001;85(3):290–4. doi: 10.1136/heart.85.3.290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Evenson KR, Fleury J. Barriers to outpatient cardiac rehabilitation participation and adherence. J Cardiopulm Rehabil. 2000;20(4):241–6. doi: 10.1097/00008483-200007000-00005. [DOI] [PubMed] [Google Scholar]
- 25.Franks MM, Stephens MA, Rook KS, Franklin BA, Keteyian SJ, Artinian NT. Spouses’ provision of health-related support and control to patients participating in cardiac rehabilitation. J Fam Psychol. 2006;20(2):311–8. doi: 10.1037/0893-3200.20.2.311. [DOI] [PubMed] [Google Scholar]
- 26.Greenberg S, Almaro N, Keren G, Sheps D. The effect of spouse participation in cardiac rehabilitation program on patients’ compliance and exercise level. Harefuah. 2004;143(2):99–102, 168, 167. [PubMed] [Google Scholar]
- 27.Mak YM, Chan WK, Yue CS. Barriers to participation in a phase II cardiac rehabilitation programme. Hong Kong Med J. 2005;11(6):472–5. [PubMed] [Google Scholar]
- 28.Mochari H, Singh D. Personal factors, rather than health status, may predict referral for cardiac rehabilitation. Evid Based Cardiovasc Med. 2006;10(2):130–1. doi: 10.1016/j.ebcm.2006.04.051. [DOI] [PubMed] [Google Scholar]
- 29.Adair R, Greminger A, Post B. Access to health care: differences between insured and uninsured patients in south Minneapolis. Minn Med. 2006;89(4):46–7. [PubMed] [Google Scholar]
- 30.Knowles E, Munro J, O’Cathain A, Nicholl J. Equity of access to health care. Evidence from NHS Direct in the UK. J Telemed Telecare. 2006;12(5):262–5. doi: 10.1258/135763306777889091. [DOI] [PubMed] [Google Scholar]
- 31.Paquet M, Bolduc N, Xhignesse M, Vanasse A. Re-engineering cardiac rehabilitation programmes: considering the patient’s point of view. J Adv Nurs. 2005;51(6):567–76. doi: 10.1111/j.1365-2648.2005.03544.x. [DOI] [PubMed] [Google Scholar]
- 32.Parfitt G, Rose EA, Burgess WM. The psychological and physiological responses of sedentary individuals to prescribed and preferred intensity exercise. Br J Health Psychol. 2006;11(Pt 1):39–53. doi: 10.1348/135910705X43606. [DOI] [PubMed] [Google Scholar]
- 33.Kamke W, Dovifat C, Schranz M, Behrens S, Moesenthin J, Voller H. Cardiac rehabilitation in patients with implantable defibrillators. Feasibility and complications. Z Kardiol. 2003;92(10):869–75. doi: 10.1007/s00392-003-0997-1. [DOI] [PubMed] [Google Scholar]
- 34.Giallauria F, Paragliola T, Pilerci F, Del FD, De LA, Manakos A, et al. Role of smokers in the household and of cardiac rehabilitation in smoking behaviour after acute myocardial infarction. Monaldi Arch Chest Dis. 2005;64(2):110–5. doi: 10.4081/monaldi.2005.596. [DOI] [PubMed] [Google Scholar]
- 35.Yoshida T, Kohzuki M, Yoshida K, Hiwatari M, Kamimoto M, Yamamoto C, et al. Physical and psychological improvements after phase II cardiac rehabilitation in patients with myocardial infarction. Nurs Health Sci. 1999;1(3):163–70. doi: 10.1046/j.1442-2018.1999.00021.x. [DOI] [PubMed] [Google Scholar]
- 36.Maclean N, Pound P, Wolfe C, Rudd A. Qualitative analysis of stroke patients’ motivation for rehabilitation. BMJ. 2000;321(7268):1051–4. doi: 10.1136/bmj.321.7268.1051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Johnson NA, Heller RF. Prediction of patient nonadherence with home-based exercise for cardiac rehabilitation: the role of perceived barriers and perceived benefits. Prev Med. 1998;27(1):56–64. doi: 10.1006/pmed.1997.0235. [DOI] [PubMed] [Google Scholar]