

Abstract
Injuries to the medial side of the knee can occur in isolation or in conjunction with multiple other ligaments about the knee. In addition, medial knee injuries can involve isolated injury to the medial collateral ligament or include the posteromedial structures of the knee. Treatment strategies differ greatly depending on injury pattern. In order to select an appropriate treatment strategy, one must accurately diagnose the injury pattern based on clinical examination and the use of appropriate imaging studies. The fundamental basis for diagnosis of a medial sided knee injury stems from understanding the static and dynamic stabilizing structures that compose the medial side of the knee. It is our aim to define the anatomic roles of medial sided structures, their importance in protecting the biomechanical stability of the knee, as well as provide indications and our preferred procedures for surgical management of these complex injuries.
Keywords: Posteromedial corner, Medial collateral ligament, Multiligamentous knee injury
Introduction
The medial side of the knee is significantly complex. Understanding the complicated relationship between anatomic structures and their unique biomechanical function provides an insight on how best to treat injuries involving the posteromedial corner (PMC). Recognizing the difference between injuries involving the medial collateral ligament and the structures of the PMC has important clinical implications. Failure to recognize this difference has been implicated as a potential reason for failure of reconstructed cruciate ligaments in combined injuries [1–3]. This article provides information based on review of recent literature that describes the anatomy, biomechanical function, and current treatment principles regarding the PMC. In addition, we will provide our current preferred method for reconstruction of the PMC based on outcomes in patients treated with multiligamentous knee injuries.
Anatomic considerations
Although the lateral side of the knee has often been referred to as the “dark side of the knee” [4], until recently there has been considerably less literature devoted to the PMC. The medial collateral ligament (MCL) is not one discrete structure, but is actually a complex of multiple structures that exist in continuity and work in conjunction with the structures of the posteromedial corner to provide stability. Over the years, the MCL has been referred to under various names with varying definitions, which has added to the confusion in the literature. Palmer in 1938 described the MCL as having superficial and deep parts [5]. Less than a decade later Brantigan and Voshell referred to this structure as the tibial collateral ligament [6]. In their early anatomical description they divided it into an anterior portion with fibers running parallel, and a posterior portion with fibers running in an oblique fashion. Later, Warren and Marshall divided the medial side into 3 distinct layers which included a fascial layer, a superficial layer, and a deep layer; however, little emphasis was placed on the structures that exist posterior to the MCL [7]. Eventually, Houghston and Eilers described the posterior oblique ligament as a “discrete anatomical thickening of the capsular ligament” [8]. Over time our understanding of the knee’s medial structures has evolved and the most current accepted anatomic definitions are listed below.
The MCL
The first layer described by Warren is the fascial layer that wraps around the knee in a circumferential layer [7]. Because this layer is not distinct to the collateral ligament, recent authors have discontinued describing it as a functional layer of the MCL. Layer II in Warren’s description contains the superficial MCL. According to LaPrade, the origin of the superficial MCL lies in a depression 3.2 mm proximal and 4.8 mm posterior to the medial femoral epicondyle [9]. The superficial MCL attaches approximately 4.6 to 6 cm distal to the articular surface of the tibia, remaining extracapsular and eventually blending with the periosteum of the tibia, bridged by the pes anserinus [5, 10]. The reinforcement provided by the pes prevents excessive tibial rotation during knee flexion [10]. It is approximately 10 mm wide at its proximal insertion, fanning out to a width of 20 mm at its widest point as it crosses the medial joint line [5]. Warren’s third layer included a thickening of the medial joint capsule that lies directly deep to the superficial MCL [7]. The deep MCL has an intimate association with the medial meniscus, including the meniscotibial and meniscofemoral ligaments.
More recent literature has moved away from the 3 layer approach when describing the medial knee and has instead moved toward dividing the medial side of the knee in thirds—the anterior third, the middle third, and the posterior third [11]. The anteromedial third of the knee involves thin capsular ligaments that lie deep to the extensor retinaculum. The middle third are the deep medial capsular ligament (or deep MCL including the attachment of the medial meniscus) and the superficial MCL. The superficial and deep components of the MCL are separated by loose bursal tissue, which allows the superficial component to slide anterior to posterior during knee flexion [6]. The posteromedial third is comprised of the posterior oblique ligament, semimembranosus expansions, posterior horn of the medial meniscus, and the oblique popliteal ligament [11].
The Posterior Oblique Ligament (POL)
As described by Brantigan and Voshell, the superficial MCL fans out obliquely at its posterior portion [6]. This was later described by Hughston and Eilers as the posterior oblique ligament (POL), arising from the adductor tubercle just posterior to the medial epicondyle and anterio-inferior to the medial head of the gastrocnemius muscle, thereby having a distinct origin from the superficial MCL [8]. It attaches to the tibia just inferior to the articular surface. The POL has been shown in some dissections to have 3 separate arms: a tibial or central arm, a capsular arm which blends with the oblique popliteal ligament, and a superficial arm that blends with the superficial MCL [9, 12]. The primary component is the central arm, which arises from the semimembranosus tendon and attaches directly to the posterior meniscus and joint capsule [9, 10, 13]. One third of the POL is firmly attached to the medial meniscus, whereas the remaining 2 thirds of its fibers pass freely from their femoral and tibial attachments [12]. The POL is distinctly biomechanically different in its function despite often being thought of as an extension of the superficial MCL.
The Posteromedial Corner (PMC)
The structures of the PMC include those that lie posterior to the border of the longitudinal fibers of the superficial MCL to the medial border of the posterior cruciate ligament. If following the model of dividing the knee into thirds, this would be the posterior third [11]. As previously described this includes the POL, the semimembranosus expansions, the posteromedial horn of the meniscus, and the oblique popliteal ligament. Mueller previously described the PMC as the “semimembranosus corner” as this structure has a significant functional contribution to the dynamic stability of the PMC [14]. The expansions of the semimembranosus referred to above have been divided into 5 separate components including: the pars reflexa that inserts directly on the tibia, the direct posteromedial insertion on the tibia, the oblique popliteal ligament insertion, the POL insertion, and the popliteus aponeurosis [11, 12]. The tendonous attachment of the semimembranosus muscle to the tibia allows it to act as a dynamic stabilizer of the PMC [11–13]. The biomechanical function of these structures will be discussed in the next section.
Biomechanics
Biomechanical analysis has shown motion at the knee to be significantly complex. As the knee flexes and extends thru its arc of motion, the tibia rotates with respect to the distal femur, adding to the complexity. In order to understand the biomechanical function of the structures of the PMC, one must also be aware of the role the MCL complex plays. In Warren’s initial works, the superficial MCL was described as the “prime static stabilizer of the medial side of the knee” [7]. Valgus forces are resisted by the superficial MCL with the knee in the flexed position; however, it does not seem to affect medial stability at full extension based on early studies that evaluated isolated sectioning of the ligament [15, 16]. More advanced biomechanical studies have recently shown the superficial MCL to provide the primary restraint to valgus force at all angles through the arc of motion at its proximal end [17•, 18•]. In contrast, the restraint provided by the distal extent of the superficial MCL is affected by the amount of flexion of the joint, with 60° providing the greatest valgus load [10, 17•]. The deep MCL acts as a secondary static stabilizer, providing resistance to valgus stress at all angles of flexion [10, 17•]. A secondary function of the MCL is resistance to anterior and posterior stress, supplementing the primary function of the cruciate ligaments [16, 19]. In addition, the MCL provides static restraint for rotational stability. The load seen by the superficial MCL is highest in external rotation [18•], therefore an increase in tibial external rotation is seen with isolated sectioning of the ligament, especially at 90° of flexion [16]. This is in contrast to the posterior oblique ligament where the load is highest in internal rotation at full extension [17•, 18•].
The structures of the PMC are taut in full extension, providing stability and resistance to valgus stress in the fully extended position [15, 20]. These structures begin to slacken as the knee flexes. At this point the superficial MCL becomes tight and provides the stability in the coronal plane [13]. The POL also acts as in concert with the MCL to resist rotational forces [17•, 18•]. When the MCL complex and PMC are both no longer competent, external rotation of the tibia is significantly increased. It is most likely with combined MCL and PMC injuries that patients develop anteromedial rotatory instability (AMRI) [21]. Sims and Jacobson reviewed injury patterns in patients who demonstrated AMRI. In their series 88 % had sustained combined injuries to the POL and MCL [12]. They demonstrated that the medial tibial plateau undergoes an anterior rotator subluxation around the central axis of the posterior cruciate ligament (PCL). In a study in 2006 Robinson demonstrated that the phenomenon of AMRI seems to be increased with increasing degrees of knee flexion, and found it highest at 90o [20]. Furthermore, biomechanical studies have shown that the POL acts as a secondary stabilizer preventing posterior tibial translation at full extension. This has significant effects if the PCL is injured as well, since the posterior tibial translation is significantly increased in a combined injury at both neutral and external rotation of the tibia [19, 22].
Diagnosis
Understanding the complex anatomy of the medial side of the knee is an integral part of developing the diagnosis. In order to achieve successful outcomes in patients with complex knee injuries, it is important that the surgeon properly differentiate between isolated injuries of the MCL and those that involve the PMC structures. As with all patients with orthopedic injuries, the first step in diagnosing a knee injury is obtaining a clear history that includes the mechanism of injury. A direct force to the outside of the leg produces a valgus stress and can result in isolated injuries to the MCL, as can be seen in athletes involved with contact sports [10]. If an external rotation force is coupled with that valgus stress it is more likely to result in an injury that also involves PMC structures. Higher energy mechanisms can lead to knee dislocations, resulting in injuries to multiple ligaments about the knee [23, 24•]. After obtaining a thorough history from the patient, an extensive physical examination is performed to further investigate the suspected diagnosis.
The physical examination begins with evaluation of the soft tissues surrounding the knee. Note any areas of ecchymosis or effusion involving the knee joint. Isolated edema medially is often indicative of an isolated MCL injury. An effusion of the knee often results from intra-articular pathology, such as injury to the cruciate ligaments, or meniscus [10, 13]. High energy trauma can occasionally result in open injuries and should be treated according to the guidelines for open fractures. The neurovascular status of the limb should also be evaluated, especially in those patients with multiligamentous knee injuries, as the popliteal artery and common peroneal nerve can be injured [25–28]. Injury to the popliteal artery can be limb threatening and should be addressed promptly. An ankle-brachial index (ABI) should be performed if any concern of arterial injury arises following physical examination. Mills et al. reported a 100 % sensitivity and specificity with ABIs <0.9 for patients with a clinically significant arterial injury [27]. If the vascular physical examination is normal the patient should be admitted and observed for at least 48 hours to make certain a late vascular occlusion does not occur [25].
When an injury to the medial knee is suspected specific physical examination maneuvers are used to determine if this is isolated to the MCL complex, or if the structures of the PMC are involved. Distinguishing between the 2 is the key step to developing the proper treatment algorithm. The examiner applies a valgus stress to the knee at both 0° and 30° of flexion. Valgus laxity with the knee flexed at 30° is the most sensitive test for medial knee injuries [29]. This, however, does not differentiate between PMC and isolated MCL injuries. The hallmark of injury to the PMC is the presence of anteromedial rotary instability (AMRI). AMRI is defined as external rotation with anterior subluxation of the medial tibial plateau relative to the distal femur [11, 21]. The PCL acts as the central axis during this translation. To diagnose AMRI, an anterior drawer test is performed with the knee flexed at 90° and the foot held in 10° of external rotation [30]. The degree of translation is noted and is compared with an anterior drawer test with the foot in neutral rotation. Increased translation with the tibia in external rotation is indicative of AMRI. When a coexisting PCL injury is suspected a posterior drawer test is performed with the foot in neutral and internal rotation. The PMC acts as a secondary stabilizer with an isolated PCL injury, thereby decreasing tibial translation when the foot is held in internal rotation, if intact. With a combined PCL-PMC injury translation during posterior drawer testing is increased when the tibia is internally rotated, since these secondary stabilizers are no longer competent [19].
Imaging studies are used to support the physical examination findings, but are not to be used to replace a thorough examination. Plain radiographs of the knee are first obtained to evaluate osseous structures for fracture, subluxation, or dislocation. A recent article by LaPrade recommends the use of valgus stress radiographs at 0° and 20° of flexion to evaluate for medial injury as well as monitoring postoperative follow up [31•]. Medial joint space widening greater than 3.2 mm when compared with the unaffected knee at 20° of flexion indicates a probable grade III MCL complex sprain [31•]. Significant medial gapping with the knee at full extension may indicate a coexisting anterior cruciate ligament (ACL) or PCL injury [31•]. Garavaglia et al. describe the use of posterior stress radiographs to evaluate combined PCL and PMC injuries, where >12 mm of posterior translation at 80° of flexion is considered a positive test [32].
Magnetic resonance imaging (MRI) is likely the most useful imaging study to evaluate the extent of injury. If an MRI is to be performed, it should be done prior to fixation of any co-existing peri-articular fractures, as metal artifacts can affect the quality of the study. MRI is particularly useful when evaluating patients with multiligamentous knee injuries; however, it has been shown that MRI tends to overestimate injury to ligamentous structures [33]. It is for this reason that the MRI should be used to supplement the physical examination, and not replace it as the only tool used for surgical planning. Injuries to the MCL complex are best seen on coronal images. Bony edema of the lateral condyle of the femur and lateral tibial plateau are seen in up to 45 % of patients with medial sided injuries [10, 34]. Co-existing injury to the menisci or osteochondral surfaces are best evaluated by MRI or diagnostic arthroscopy. Examination under anesthesia continues to be the most accurate tool when diagnosing a complex knee injury and should be performed in detail using the examination maneuvers listed above prior to any surgical reconstruction.
Treatment
Isolated injury to the MCL complex will typically heal with favorable results without operative intervention, especially in the instance of grade I or grade II injuries [29, 35–38]. The extra-articular location of the MCL allows the superficial MCL the potential to heal primarily, without repair or reconstruction [10, 39]. This is thought to be in contrast to the ACL, which is constantly bathed in synovial fluid and has limited blood supply due to its intra-articular location, thereby limiting its healing potential [10, 39]. Complete disruption of the MCL (grade III injury) is often associated with injury to another ligament, most often the ACL [10, 13, 29, 38]. There is significant controversy when dealing with combined ACL and MCL injuries among the literature. Often the ACL is reconstructed and the MCL is left to heal primarily with some success [38–40]. Some recent concern has developed with following this method. Multiple studies have shown patients to have greater anterior to posterior translation at 90° and increased valgus laxity at 30° with these combined injuries when compared with isolated ACL patients [38, 41]. In addition, increased valgus laxity with incomplete healing of the MCL complex has been shown to increase stress across the reconstructed ACL [1, 42•, 43]. For this reason, some have proposed addressing these injuries separately [10, 13]. These patients undergo a 4- to 6-week period of bracing to allow healing of the MCL, while simultaneously doing rehabilitation exercises to increase range of motion in preparation of the ACL reconstruction. Finally, at the time of ACL reconstruction an examination under anesthesia is performed. Any significant residual valgus laxity is addressed at the same time as the ACL reconstruction; with reconstruction of the MCL in an effort to decrease the likelihood of late graft failure [10, 13].
Injury to the PMC becomes more common in higher energy bicruciate knee injuries and knee dislocations [24•]. Due to increased posterior translation of the tibia encountered with coexisting injuries to the PCL and PMC (specifically the POL) [19, 22, 44], this injury pattern is best treated with operative management consisting of reconstruction of both anatomic structures [19, 24•]. Patients with multiple ligament injuries and evidence of AMRI on physical examination benefit from stabilization and reconstruction of the PMC [24•, 45•]. There is a difference of opinion on what order to address the injured structures. Some authors recommend addressing injuries to both cruciate and collateral ligaments in the same surgery [29]. Our preference is to reconstruct the PCL and PMC in 1 setting, and addressing the ACL in a delayed fashion [24•]. This is felt to maximize the rehab protocols for each cruciate ligament, and allows the patient to recover range of motion prior to reconstructing the ACL. This way if motion is still limited at the time of the ACL reconstruction either a manipulation under anesthesia or lysis of adhesions can be performed to improve motion. Still others recommend addressing the cruciate ligaments while allowing time to see if the medial sided knee structures will heal nonoperatively [40, 46]. This is now thought to have less favorable results: recent studies have proven the significant role that the POL and PMC play as a stabilizer of internal rotation and valgus stress [22].
Surgical technique: authors preferred treatment
When multiple ligaments are to be reconstructed, our preferred order of treatment is as follows: examination under anesthesia, diagnostic arthroscopy, repair or resection of meniscus tear as indicated, reconstruction of the PCL using an inlay technique without tensioning or fixation of the graft on the femur, followed by reconstruction of the MCL/PMC without tensioning on the tibia [24•, 47]. Once the PMC graft is in place, the PCL is tensioned and fixed. The final step is fixation of the PMC graft. The same reconstruction procedure is performed in instances of MCL injuries and of those involving the PMC. If the ACL is to be reconstructed we prefer to do this as a staged procedure 6 weeks following reconstruction of the PMC/PCL to optimize the rehab protocols for each ligament. In this section we will describe only the preferred technique for reconstruction of the PMC. Primary repair of the PMC has been utilized; however, in a recent study published by the senior author we noted a significantly higher failure rate with repair (20 %) vs reconstruction (4 %) [24•]. We recommend using a technique for ACL and PCL reconstruction that the operating surgeon feels comfortable with to allow for best results of complex injuries.
Either allograft or autograft may be used when reconstructing the PMC. When multiple ligaments are to be addressed, it is often beneficial to use allograft to limit morbidity to the patient. Currently the authors’ preference is to use 2 semitendinosus allografts for reconstruction [47]. Each end of the graft is prepared for passage with a permanent number 2 suture passed in a locking fashion. A biotenodesis screw (Arthrex, Naples, FL) is fixed to the 2 grafts, forming 2 limbs. The graft is then placed aside while the approach to the medial side of the knee is performed.
Following a diagnostic arthroscopy, the patient’s leg is placed in the figure-4 position. An incision is made longitudinally following the posteromedial border of the tibia. The insertion of the semitendinosus tendon marks the distal aspect of the incision. The distal aspect of the femur is exposed in the proximal aspect of the incision. Fluoroscopy is used to obtain a perfect lateral of the distal femur. The isometric point of the distal femur is then found where Blumenstaat’s line intersects a line extended along the anterior aspect of the posterior cortex of the femoral shaft [24•, 47]. Once the isometric point is identified a threaded guide pin is inserted in the femur from medial to lateral. A cannulated reamer is used to drill a socket over the guide pin the appropriate size to accommodate the diameter of the biotenodesis screw used for fixation. The socket is drilled to a depth of 25 mm. The screw with the attached graft is inserted in the socket at the isometric point. The 2 semitendinosus grafts are positioned where the anterior graft will recreate the MCL and the posterior graft reconstructs the POL providing stability to the PMC.
Just proximal to the insertion of the semitendinosus tendon on the medial tibia, a 3.2 mm drill bit is used to create a bicortical drill hole. A 4.5 mm screw with a spiked ligament washer is placed in the drill hole. Prior to fully seating the screw, the anterior limb of the graft is taken directly inferior from its femoral insertion in line with the MCL. The posterior graft tunnels under the semimembranosus in a posterior to anterior direction toward the tibial screw (Fig. 1). This graft recreates the POL as well as the direct insertion of the semimembranosus. The knee is flexed to 30° and the tibial screw with spiked washer is fully seated, securing the graft in place as a very gentle varus stress is applied to the knee while at neutral rotation.
Fig. 1.
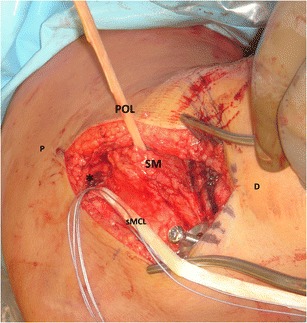
A biotenodesis screw (Arthrex, Naples, FL) has been anchored at the isometric point (*) with the 2 semitendinosus grafts attached. The anterior graft (sMCL) is oriented longitudinally and reconstructs the superficial MCL. The posterior graft (POL) has been tunneled obliquely under the semimembranosis (SM) to reconstruct the course of the posterior oblique ligament. Both limbs of the graft will be anchored to the tibia with the screw and spiked ligament washer at the distal aspect of the incision. (P = proximal; D = distal)
Outcomes
The senior author of this review has previously published outcomes using the above described technique for reconstruction [24•]. Patients were treated for knee dislocations and a total of 71 patients with 73 injuries to the PMC were reviewed. Patients were divided in 3 groups: primary repair, autograft reconstruction, and allograft reconstruction. Of the 25 patients who underwent repair, 5 failures occurred (20 %). This is in contrast to the reconstruction groups where 48 reconstructions were performed with 2 failures (4 %). The difference between repair vs reconstruction was found to be statistically significant. There was one failure in the autograft group and one in the allograft group, which was not statistically different. This data supports our preference for reconstruction of the PMC [24•, 47]. A brief review of the most recent studies describing outcomes of surgical treatment of MCL and PMC injuries are summarized in the Table 1.
Table 1.
Outcomes of MCL/PMC repairs or reconstructions
| Number of patients | Repair vs reconstruction | Graft used | Follow-up | Outcomes measures | |
|---|---|---|---|---|---|
| Kim et al. 2008 [48] | 24 MCL + POL | Reconstruction MCL/PMC | Semitendinosus autograft with preserved tibial attachment | Mean 52.6 mo | Lysholm score 91.9 |
| (range 25–92) | (range 80–100) | ||||
| 2 mm medial joint space opening in 22 of 24 | |||||
| Lind et al. 2009 [45] | 13 isolated MCL | Reconstruction | Ipsilateral semitendinosus autograft with preserved pes attachment | Median 40 mo | KOOS score improved average of 10 points |
| 34 ACL + MCL | MCL/PMC | (range 26–68) | 91.2 % satisfied or very satisfied | ||
| 14 multiple ligaments | IKDC 98 % grade A or B medial laxity | ||||
| Yoshiya et al. 2005 [49] | 12 MCL + ACL | Reconstruction | Semitendinosus and gracilis autograft | Mean 27 mo | 83 % stable to valgus stress |
| 7 MCL + PCL | sMCL only | (range 24–48) | 17 % mild valgus instability | ||
| 3 MCL + PCL + ACL | Side to side difference of 2 mm or less in 100 % | ||||
| 2 isolated MCL | IKDC normal or near normal in 88 % | ||||
| Stannard et al. 2012 [24•] | 25 patients with direct repair of PMC | Repair vs Reconstruction | Semitendinosus allograft and autograft reconstructed MCL and POL | Mean 43 mo | 20/25 stable to valgus stress in repair group (80 %) |
| 48 patients with reconstruction of MCL/PMC | 46/48 stable to valgus stress in reconstruction group (96 %) | ||||
| *all patients sustained knee dislocations with multiligamentous injuries |
MCL medial collateral ligament, PMC posteromedial corner, ACL anterior cruciate ligament, PCL posterior cruciate ligament
Conclusion
Recent anatomic and biomechanical studies have provided important insight to the structure and function of the PMC and MCL complex. It is important to use a thorough physical examination to differentiate between injuries involving the MCL and PMC. PMC injuries appear to be more common in higher energy, multiple ligament injuries, whereas isolated MCL injury is more common when combined with an ACL disruption. Failure to recognize and treat an injury to the PMC can lead to residual valgus laxity, as well as produce a significant increase in posterior tibial translation that puts added stress on ACL and/or PCL reconstructions. Primary repair of the PMC structures appear to have a significantly higher failure rate when compared with reconstruction when treating multiple ligament injuries. Our preferred technique of reconstruction reestablishes the biomechanically important triangle of the MCL, POL, and semitendinosus sling to recreate the stability provided by the PMC.
Disclosure
KL Bauer: none; JP Stannard: consultant for KCI, Medtronic, Sonoma, Smith and Nephew, receives royalties from Thieme.
Contributor Information
Kathryn L. Bauer, Email: bauerkl@health.missouri.edu
James P. Stannard, Email: stannardj@health.missouri.edu
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
- 1.Ichiba A, Nakajima M, Fujita A, Abe M. The effect of medial collateral ligament insufficiency on the reconstructed anterior cruciate ligament. Acta Orthop Scand. 2003;74:196–200. doi: 10.1080/00016470310013950. [DOI] [PubMed] [Google Scholar]
- 2.Carson EW, Anisko EM, Restrepo C, Panariello RA, O’Brien SJ, Warren RF. Revision anterior cruciate ligament reconstruction: etiology of failures and clinical results. J Knee Surg. 2004;17:127–32. doi: 10.1055/s-0030-1248210. [DOI] [PubMed] [Google Scholar]
- 3.Noyes FR, Barber-Westin SD. Revision anterior cruciate surgery with use of bone-patellar tendon-bone autogenous grafts. J Bone Joint Surg. 2001;83:1131–43. doi: 10.2106/00004623-200108000-00001. [DOI] [PubMed] [Google Scholar]
- 4.Andrews JB, Baker CL, Curl WW, et al. Surgical repair of acute and chronic lesions of the lateral capsular ligamentous complex of the knee. In: Fergin JA Jr, et al., editors. Injuries about the knee. New York: Churchill Livingstone; 1988. pp. 425–38. [Google Scholar]
- 5.Palmer I. On the injuries to the ligaments of the knee joint. Acta Orthop Scand Suppl. 1938;53:283. [Google Scholar]
- 6.Brantigan OC, Voshell AF. The tibial collateral ligament: its function, its bursae, and its relation to the medial meniscus. J Bone Joint Surg. 1943;25:121–31. [Google Scholar]
- 7.Warren LF, Marhall JL, Girgis F. The prime static stabilizer of the medial side of the knee. J Bone Joint Surg. 1974;56–A:665–74. [PubMed] [Google Scholar]
- 8.Hughston JC, Eilers AF. The role of the posterior oblique ligament in repairs of acute medial (collateral) ligament tears of the knee. J Bone Joint Surg. 1973;55–A:923–40. [PubMed] [Google Scholar]
- 9.LaPrade RF, Engebresten AH, Ly TV, Johansen S, Wentorf FA, Engebresten L. The Anatomy of the Medial Part of the Knee. J Bone Joint Surg. 2007;89:2000–10. doi: 10.2106/JBJS.F.01176. [DOI] [PubMed] [Google Scholar]
- 10.Marchant Jr MH, Tibor LM, Sekiya JK, Hardaker Jr WT, Garrett Jr WE, Taylor DC. Management of medial-sided knee injuries, Part 1: medial collateral ligament. Am J Sports Med. 2011;39–5:1102–13. [DOI] [PubMed]
- 11.Robinson JR, Sanchez-Ballester J, Bull AM, Thomas Rde W, Amis AA. The posteromedial corner revisited: an anatomical description of the passive restraining structures of the medial aspect of the human knee. J Bone Joint Surg Br. 2004;86–B:674–81. doi: 10.1302/0301-620X.86B5.14853. [DOI] [PubMed] [Google Scholar]
- 12.Sims WF, Jacobson KE. The posteromedial corner of the knee: medial-sided injury patterns revisited. Am J Sports Med. 2004;32:337–45. doi: 10.1177/0363546503261738. [DOI] [PubMed] [Google Scholar]
- 13.Tibor LM, Marchant Jr MH, Taylor DC, Hardaker Jr WT, Garrett Jr WE, Sekiya JK. Management of medial-sided knee injuries, Part 2: posteromedial corner. Am J Sports Med. 2011;39–6:1332–40. [DOI] [PubMed]
- 14.Mueller W. The knee: form, function, and ligament reconstruction. Berlin: Springer-Verlag; 1983. [Google Scholar]
- 15.Grood ES, Noyes FR, Butler DL, Suntay WJ. Ligamentous and capsular restraints preventing medial and lateral laxity in intact human cadaver knees. J Bone Joint Surg. 1981;63:1257–69. [PubMed] [Google Scholar]
- 16.Haimes JL, Wroble RR, Grood ES, Noyes FR. Role of the medial structures in the intact and anterior cruciate ligament-deficient knee. Am J Sports Med. 1994;22:402–9. doi: 10.1177/036354659402200317. [DOI] [PubMed] [Google Scholar]
- 17.Griffith CJ, Wijdicks CA, LaPrade RF, Armitage BM, Johansen S, Engebresten L. Force measurements on the posterior oblique ligament and superficial medial collateral ligament proximal and distal divisions to applied loads. Am J Sports Med. 2009;37:140–8. doi: 10.1177/0363546508322890. [DOI] [PubMed] [Google Scholar]
- 18.Griffith CJ, LaPrade RF, Johansen S, Armitage BM, Wijdicks CA, Engebresten L. Medial knee injury: Part 1, static function of the individual components of the main medial knee structures. Am J Sports Med. 2009;37:1762–70. doi: 10.1177/0363546509333852. [DOI] [PubMed] [Google Scholar]
- 19.Ritchie JR, Bergfeld JA, Kambic H, Manning T. Isolated sectioning of the medial and posteromedial capsular ligaments in the posterior cruciate ligament-deficient knee: influence on the posterior tibial translation. Am J Sports Med. 1998;26:389–94. doi: 10.1177/03635465980260030801. [DOI] [PubMed] [Google Scholar]
- 20.Robinson JR, Bull AMJ, Thomas RR, Amis AA. The role of the medial collateral ligament and posteromedial capsule in controlling knee laxity. Am J Sports Med. 2006;34:1815–23. doi: 10.1177/0363546506289433. [DOI] [PubMed] [Google Scholar]
- 21.Hughston JC, Barrett GR. Acute anteromedial rotatory instability: long-term results of surgical repair. J Bone Joint Surg. 1983;65:145–53. doi: 10.2106/00004623-198365020-00002. [DOI] [PubMed] [Google Scholar]
- 22.Peterson W, Loerch S, Schanz S, Raschke M, Zantop T. The role of the posterior oblique ligament in controlling posterior tibial translation in the posterior cruciate ligament-deficient knee. Am J Sports Med. 2008;36:493–501. doi: 10.1177/0363546507310077. [DOI] [PubMed] [Google Scholar]
- 23.Harner CD, Waltrip RL, Bennett CH, Rancis KA, Cole B, Irrgang JJ. Surgical management of knee dislocations. J Bone Joint Surg. 2004;86:262–73. doi: 10.2106/00004623-200402000-00008. [DOI] [PubMed] [Google Scholar]
- 24.Stannard JS, Black BS, Azbell C, Volgas DA. Posteromedial corner injury in knee dislocations. J Knee Surg. 2012;25:429–34. doi: 10.1055/s-0032-1322605. [DOI] [PubMed] [Google Scholar]
- 25.Stannard JP, Sheils TM, Lopez-Ben RR, McGwin G, Jr, Robinson JT, Volgas DA. Vascular injuries in knee dislocations: the role of physical examination in determining the need for arteriography. J Bone Joint Surg. 2004;86:910–5. [PubMed] [Google Scholar]
- 26.Levy BA, Fanelli GC, Whelan DB, Stannard JP, MacDonald PA, Boyd JL, et al. Knee Dislocation Study Group: controversies in the treatment of knee dislocation and multiligament reconstruction. JAAOS. 2009;17(4):197–206. doi: 10.5435/00124635-200904000-00001. [DOI] [PubMed] [Google Scholar]
- 27.Mills WJ, Barei DP, McNair P. The value of the ankle-brachial index for diagnosing arterial injury after knee dislocation: a prospective study. J Trauma. 2004;56:1261–5. doi: 10.1097/01.TA.0000068995.63201.0B. [DOI] [PubMed] [Google Scholar]
- 28.Niall DM, Nutton RW, Keating JF. Palsy of the common peroneal nerve after traumatic dislocation of the knee. J Bone Joint Surg Br. 2005;87:664–7. doi: 10.1302/0301-620X.87B5.15607. [DOI] [PubMed] [Google Scholar]
- 29.Fanelli GC, Harris JD. Surgical treatment of acute medial collateral ligament and posteromedial corner injuries of the knee. Sports Med Arthrosc. 2006;14(2):78–83. doi: 10.1097/01.jsa.0000212301.80496.dc. [DOI] [PubMed] [Google Scholar]
- 30.Jacobson KE, Chi FS. Treatment of chronic injuries to the medial side of the knee. Tech Knee Surg. 2007;6:106–11. doi: 10.1097/btk.0b013e3180644c22. [DOI] [Google Scholar]
- 31.LaPrade RF, Bernhardson AS, Griffith CJ, Macalena JA, Wijdicks CA. Correlation of valgus stress radiographs with medial knee ligament injuries: an in vitro biomechanical study. Am J Sports Med. 2010;38:331–8. doi: 10.1177/0363546509349347. [DOI] [PubMed] [Google Scholar]
- 32.Garavaglia G, Lubbeke A, Dubois-Ferriere V, Suva D, Fritschy D, Menetrey J. Accuracy of stress radiography techniques in grading isolated and combined posterior knee injuries: a cadaveric study. Am J Sports Med. 2007;35:2051–6. doi: 10.1177/0363546507306466. [DOI] [PubMed] [Google Scholar]
- 33.Lonner JH, Dupuy DE, Siliski JM. Comparison of magnetic resonance imaging with operative findings in acute traumatic dislocations of the adult knee. J Orthop Trauma. 2000;14:183–6. doi: 10.1097/00005131-200003000-00006. [DOI] [PubMed] [Google Scholar]
- 34.Miller MD, Osborne JR, Gordon WT, Hinkin DT, Brinker MR. The natural history of bone bruises: a prospective study of magnetic resonance imaging-detected trabecular microfractures in patients with isolated medial collateral ligament injuries. Am J Sports Med. 1998;26:15–9. doi: 10.1177/03635465980260011001. [DOI] [PubMed] [Google Scholar]
- 35.Holden DL, Eggert AW, Butler JE. The nonoperative treatment of grades I and II medial collateral ligament injuries to the knee. Am J Sports Med. 1983;11:340–4. doi: 10.1177/036354658301100511. [DOI] [PubMed] [Google Scholar]
- 36.Indelicato PA. Nonoperative treatment of complete tears of the medial collateral ligament of the knee. J Bone Joint Surg. 1983;65:323–9. [PubMed] [Google Scholar]
- 37.Indelicato PA, Hermansdorfer J, Huegel M. Nonoperative management of complete tears of the medial collateral ligament of the knee in intercollegiate football players. Clin Orthop Relat Res. 1990;256:174–7. [PubMed] [Google Scholar]
- 38.Halinen J, Lindahl J, Hirvensalo E, Santavirta S. Operative and non-operative treatments of medial collateral ligament rupture with early anterior cruciate ligament reconstruction: a prospective randomized study. Am J Sports Med. 2006;34:1134–40. doi: 10.1177/0363546505284889. [DOI] [PubMed] [Google Scholar]
- 39.Woo SLY, Vogrin TM, Abramowitch SD. Healing and repair of ligament injuries in the knee. JAAOS. 2000;6:364–72. doi: 10.5435/00124635-200011000-00004. [DOI] [PubMed] [Google Scholar]
- 40.Klimkiewicz JJ, Petrie RS, Harner CD. Surgical treatment of combined injury to anterior cruciate ligament, posterior cruciate ligament and medial structures. Clin Sports Med. 2000;19:479–92. doi: 10.1016/S0278-5919(05)70219-2. [DOI] [PubMed] [Google Scholar]
- 41.Zaffagnini S, Bignozzi S, Martelli S, Lopomo N, Marcacci M. Does ACL reconstruction restore knee stability in combined lesions? An in vivo study. Clin Orthop Relat Res. 2007;454:95–9. doi: 10.1097/BLO.0b013e31802b4a86. [DOI] [PubMed] [Google Scholar]
- 42.Battaglia MJ, 2nd, Lenhoff MW, Ehteshami JR, Lyman S, Provencher MT, Wickiewicz TL, et al. Medial collateral ligament injuries and subsequent load on the anterior cruciate ligament: a biomechanical evaluation in a cadaveric model. Am J Sports Med. 2009;37:305–11. doi: 10.1177/0363546508324969. [DOI] [PubMed] [Google Scholar]
- 43.Ma CB, Papageogiu CD, Debski RE, Woo SL. Interaction between the ACL Graft and MCL in a combined ACL + MCL knee injury using a goat model. Acta Orthop Scand. 2000;71:387–93. doi: 10.1080/000164700317393394. [DOI] [PubMed] [Google Scholar]
- 44.Noyes FR, Barber-Westin SD. Posterior cruciate ligament revision reconstruction, Part 1: causes of failure in 52 consecutive operations. Am J Sports Med. 2005;33:646–54. doi: 10.1177/0363546504271210. [DOI] [PubMed] [Google Scholar]
- 45.Lind M, Jakobsen BW, Lund B, Hansen MS, Abdallah O, Christiansen SE. Anatomical reconstruction of the medial collateral ligament and posteromedial corner of the knee in patients with chronic medial collateral ligament instability. Am J Sports Med. 2009;37:1116–22. doi: 10.1177/0363546509332498. [DOI] [PubMed] [Google Scholar]
- 46.Shelbourne KD, Carr DR. Combined anterior and posterior cruciate and medial collateral ligament injury: nonsurgical and delayed surgical treatment. Instr Course Lect. 2003;52:413–8. [PubMed] [Google Scholar]
- 47.Stannard JP, Bauer KL. Current concepts in knee dislocations: PCL, ACL, and medial sided injuries. J Knee Surg. 2012;25:287–94. doi: 10.1055/s-0032-1326998. [DOI] [PubMed] [Google Scholar]
- 48.Kim SJ, Lee DH, Kim TE, Choi NH. Concomitant reconstruction of the medial collateral and posterior oblique ligaments for medial instability of the knee. J Bone Joint Surg Br. 2008;90:1323–7. doi: 10.1302/0301-620X.90B10.20781. [DOI] [PubMed] [Google Scholar]
- 49.Yoshiya S, Kuroda R, Mizuno K, Yamamoto T, Kurosaka M. Medial collateral ligament reconstruction using autogenous hamstring tendons: technique and results in initial cases. Am J Sports Med. 2005;33:1380–5. doi: 10.1177/0363546504273487. [DOI] [PubMed] [Google Scholar]