

Description
A 57-year-old right-handed man (smoker, suffering from severe gastro-oesophageal reflux disease and operated 5 years earlier for left ear cholesteatoma) while sleeping at home suddenly developed right haemiparesis and aphasia associated with an autoscopic phenomenon for 10 min (out-of-body experience)1 because he was seeing his wife and his own right arm from above (video 1).
The patient giving details of his out-of-body sensation.
After 6 h in stroke unit, haemiparesis was improved, but a detailed neurological examination evidenced left–right disorientation, acalculia, agraphia and finger agnosia.2 No sensory loss coexisted. The MRI scan showed an ischaemic lesion in the left inferior parietal lobe (figure 1). After 48 h, the patient's haemiparesis fully recovered and left–right disorientation was clearly reduced, but other symptoms persisted (video 2).
Figure 1.
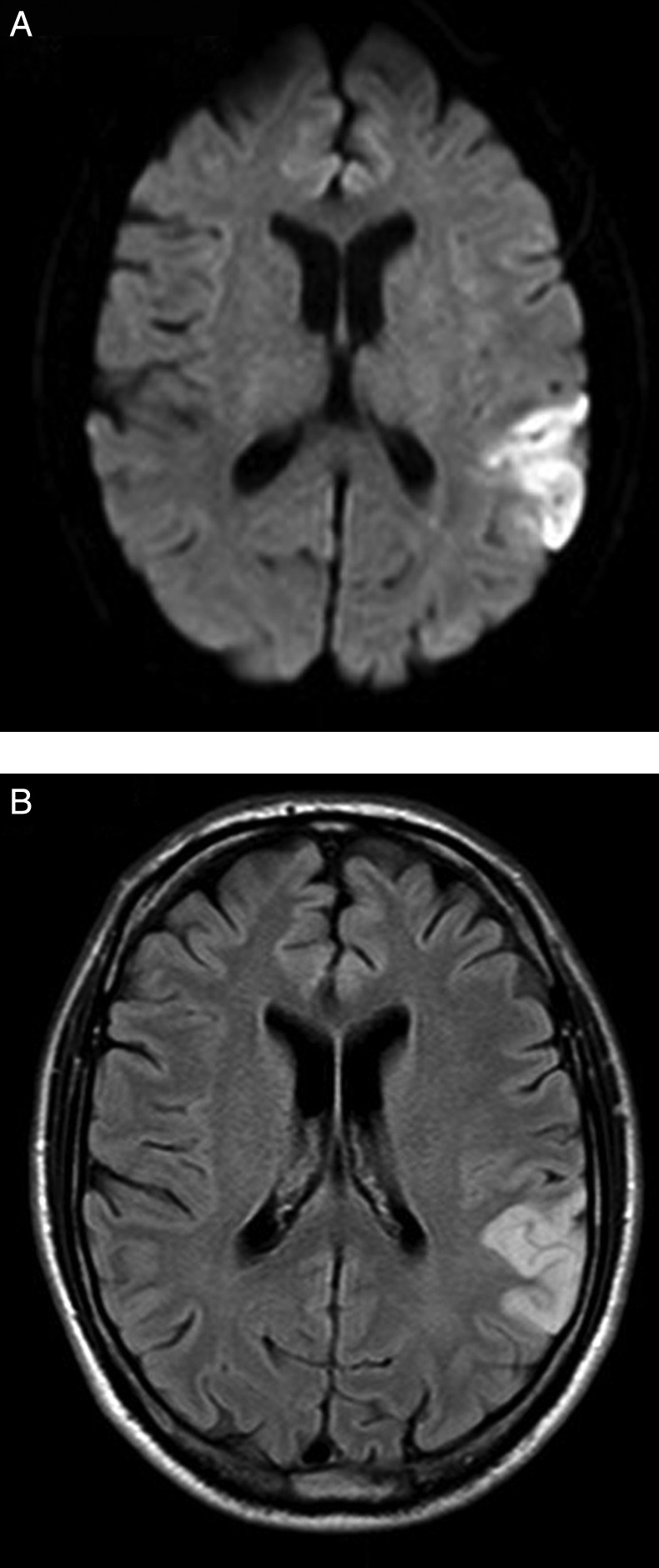
Ischemic stroke. The MRI scan performed in the acute setting documented hyperintensity in (A) DWI and (B) FLAIR sequences at the left temporo-parietal junction (angular gyrus, supramarginal gyrus, superior temporal gyrus).
The patient performing various tests to provide evidence of the selective neuropsychological impairment due to left angular gyrus lesion.
Learning points.
Selective lesions (brain tumour, stroke and trauma) in the lower left parietal lobe area could lead to four cardinal neuropsychological symptoms, that is, acalculia, left–right confusion, agraphia, finger and toe agnosia. Very rarely, all those symptoms appear together and usually other neurological deficits (such as aphasia and haemiparesis) coexist.
Autoscopia is a rare condition usually reported by patients of epilepsy when they see their body or part of their body from another perspective. In the ‘out-of-body experience’, usually people look at the ground from above.
An infarct in the area of the left angular gyrus area is the cause of finger agnosia, acalculia, agraphia, left–right confusion and autoscopia in this patient.
Footnotes
Contributors: PR was involved in the acquisition of data, video included; analysis and interpretation of data; writing and editing of the manuscript and the video. ET was involved in the analysis and interpretation of data. DM was involved in the analysis and interpretation of data. RC was responsible for study supervision.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Blanke O. Multisensory brain mechanisms of bodily self-consciousness. Nat Rev Neurosci 2012;2013:556–71 [DOI] [PubMed] [Google Scholar]
- 2.Rusconi E, Pinel P, Dehaene S, et al. The enigma of Gerstmann's syndrome revisited: a telling tale of the vicissitudes of neuropsychology. Brain 2010;2013(Pt 2):320–32 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
The patient giving details of his out-of-body sensation.
The patient performing various tests to provide evidence of the selective neuropsychological impairment due to left angular gyrus lesion.