

Abstract
Taurodont teeth are characterised by large pulp chambers at the expense of roots. An enlarged pulp chamber, apical displacement of the pulpal floor and no constriction at the level of the cement-enamel junction are the characteristic features of taurodont tooth. It appears more frequently as an isolated anomaly but its association with syndromes and other abnormalities have also been reported. Permanent dentition is more commonly affected than deciduous dentition. This paper presents a case report of taurodontism in relation to mandibular deciduous second molars.
Background
Taurodontism is a dental anomaly characterised by enlarged pulp chamber with more apical positioning of floor of pulp chamber and furcation of roots. The bifurcation or trifurcation may be few millimetres away from the radiographic apex. The distance from the trifurcation or bifurcation of the root to the cementoenamel junction (CEJ) is greater than the occlusocervical distance.1 Witkop2 defined taurodontism as teeth with large pulp chambers in which the bifurcation or trifurcation are displaced apically, so that the chamber has greater apicoocclusal height than in normal teeth and lacks the constriction at the level of CEJ. Feichtinger and Rossiwal reported that in taurodontism, the distance from the furcation to the CEJ should be greater than cervicoocclusal distance.2 Taurodontism affects permanent molar more commonly, but may be observed in both the dentitions. It may be unilateral or bilateral and in any combination of teeth or quadrants. Usually appears as an isolated, but its association with several syndromes and other abnormalities has also been reported. Most reports indicate a prevalence of 2.5–3.2%3 in permanent teeth while in deciduous teeth it is 0.54%. This paper presents a case report of taurodontism in relation to mandibular deciduous second molars.
Taurodont teeth show wide variation in the size and shape of pulp chambers, varying degrees of obliteration and canal complexity, low canal orifices and the potential for additional canal systems. Despite clinical challenges in endodontic therapy, taurodontism has received little attention from clinicians in performing root canal treatment on such teeth. One should appreciate the complexity of root canal system, canal obliteration and configuration, and the potential for additional root canal systems. Careful exploration of the grooves between all orifices particularly with magnification, use of ultrasonic irrigation; and a modified clinical technique are of particular importance.
Case presentation
A 5-year-old boy visited our department of paedodontics and preventive dentistry with pain in lower left back teeth region. Pain was dull, intermittent, localised and increased on lying down. On clinical examination there was deep carious lesion on 74 with sinus tract on buccal gingiva and deep caries with 84.
Radiographic examination revealed deep carious lesion in relation to 74 and 84 with rarefaction at furcation area and root resorption. Interestingly, there were large pulp chambers and small roots present in relation to teeth 75 and 85 (figures 1–3). The radiographs were taken by paralleling technique, traced on tracing paper and distance was measured placing the traced paper on the graph. The Shifman and Chanannel criteria were used for assessment of taurodontism. The a/b=0.32 for 75 when distal root was used and 0.25 when mesial root, a/b=0.33 for 85 when distal root was used and 0.25 when mesial root. The distance of CEJ from B point was 0.3 for both 75 and 85 (figures 4 and 5). It was confirmed that both the mandibular second deciduous molars were taurodonts. Paediatric endodontics was planned for the teeth 74 and 84. Professionally applied topical fluoride programme was planned for caries prevention.
Figure 1.

Intraoral periapical radiograph of right mandibular posterior teeth.
Figure 2.

Intraoral periapical radiograph of left mandibular posterior teeth.
Figure 3.

Orthopantomogram.
Figure 4.
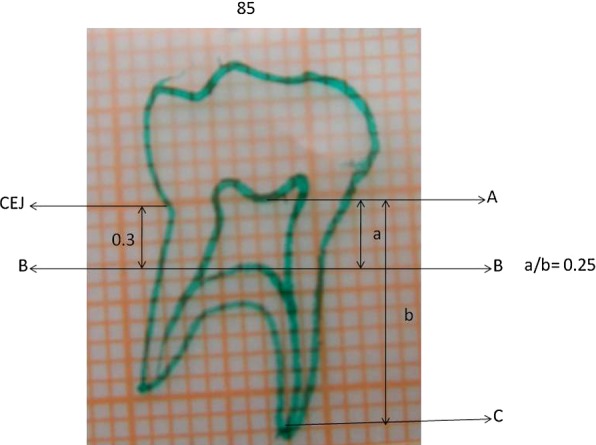
Tracing of the intraoral periapical radiograph showing tooth 85 confirming the taurodontic tooth according to Shifman and Chanannel criteria.
Figure 5.

Tracing of the intraoral periapical radiograph showing 75 confirming the taurodontic tooth according to Shifman and Chanannel criteria.
Discussion
Taurodontism is a rare condition where tooth is enlarged at the expense of the root. It is a Greek word meaning ‘bull like tooth’. It was first described by Gorjanovic-Kramberger (1908). Pickerill in 1909 used term radicular dentinoma.4 The term taurodontism was coined by Sir Arthur Keith5 1913 which means ‘bull-like’ tooth. The tooth does not demonstrate a cervical constriction and the roots usually show apical bifurcation or trifurcation.
There are various theories concerning the aetiology of taurodontism: (1) a specialised or retrograde character; (2) a primitive pattern; (3) a Mendelian recessive pattern; (4) an atavistic feature and (5) a mutation.1 Many explanations for the pathogenesis of taurodont formation have been put forward from time to time, they included (1) an unusual developmental pattern; (2) a delay in calcification of the pulp chamber floor; (3) an odontoblastic deficiency; (4) an alteration in Hertwig's epithelial root sheath, with an apparent failure of the epithelial diaphragm to invaginate at the normal horizontal levels; and (5) a delayed or incomplete union of the horizontal flaps of the epithelial diaphragm.6
Taurodontism may be genetically transmitted and could be associated with an increased number of X chromosomes.7 It has been proposed that taurodontism may be a genetically determined trait and more advantageous than cynodontism in people with heavy masticatory habits or in populations in which teeth were used as tools. In our case orthopantomograph of the patient's siblings and parents were taken but taurodontism was not evident.
Taurodontism is associated with many syndromes like Down syndrome8 Klinefelter syndrome9–11 Lowe syndrome (oculocerebrorenal syndrome), trichodento-osseous syndrome12 Williams syndrome,13 tricho-onychodental syndrome, Wolf-Hirschhorn syndrome14 van der Woude syndrome, hypophosphataemia, Seckel syndrome, Smith-Magenis syndrome, Mohr syndrome (oral-facial-digital II syndrome), Prader-Labhart-Willi syndrome, McCune-Albright syndrome, Ellis van Creveld syndrome, Apert syndrome, Lenz microphthalmia syndrome and Kabuki syndrome. DLX3 frame shift mutation was identified in the hypoplastic–hypomaturation variety of amelogenesis imperfecta with taurodontism syndrome.15
Identification of taurodontism may lead to early recognition of Klinefelter syndrome and could substantially improve quality of life.11 Some chromosomal studies on patients with an extra X chromosome such as 47, XXY males (Klinefelter’s syndrome) suggest that the X chromosome contains gene favouring the development of taurodontism. This implies that taurodontism should be more prevalent in women, as was found in a Chinese population.16 However, the expression of the condition may be influenced by other genetic or environmental factors.
The association between taurodontism and hypodontia has been found by Seow and Lai but recent study suggests no association.17 In our case, taurodontism was present with no tooth agenesis.
Taurodontism clinically appears as a normal tooth. Therefore, the diagnosis of taurodontism is usually a subjective determination made from diagnostic radiographs.18 Shaw classified taurodontism into hypo, meso and hyper taurodontism, on the basis of the apical placement of the pulp chamber floor.
In 1978, Shifman and Chanannel proposed the following criteria for determining the presence or absence of taurodontism. Taurodontism is confirmed, if the distance (a) from the lowest point (A) of the roof of the pulp chamber to the highest point of the pulpal floor (B), divided by the distance (b) from the lowest point of roof of pulp chamber to the apex (C) is 0.2 mm or greater, that is, (a/b=0.2 mm) and if the distance from the highest point of pulp chamber floor to CEJ is more than 2.5 mm (figure 5).19
Differential diagnosis of taurodontism includes pseudohypoparathyroidism, hypophosphatasia, dentinogenesis-imperfecta, hypophosphataemia and vitamin D-resistant dependent rickets. Young permanent tooth may be mistaken for taurodontism but can be differentiated as it has wide apical foramina.20
An endodontic procedure in taurodont teeth has been described as a complex and difficult procedure. Pulp therapy for taurodont teeth is a challenging treatment with increased incidence of haemorrhage during access opening which may be mistaken for perforation. The access for endodontic treatment can easily be gained but locating orifices of canal is difficult. Careful exploration of the grooves between all orifices, especially with magnification, has been recommended to reveal additional orifices and canals. Because the pulp of a taurodont is usually voluminous, in order to ensure complete removal of the pulp, 2.5% sodium hypochlorite has been suggested initially as an irrigant to dissolve pulp tissue. The material used for obturation is vitapex as in case of zincoxide eugenol, the rate of resorption is slower than the root which may lead to delayed exfoliation of deciduous teeth.21 22 The extraction of such teeth is easy as there is small surface area of tooth that is embedded in the alveolus.
Learning points.
Taurodont tooth may have an abnormal root canal system.
In performing paediatric endodontics on these teeth, one should appreciate complexity of root canal system.
Careful exploration of the grooves between all orifices, particularly with magnification, ultrasonic irrigation and a modified filling technique are recommended.
Footnotes
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Shafer WG, Hine MK, Levy MB. A textbook of oral pathology. 5th edn. Philadelphia: WB Saunders, 1999:60 [Google Scholar]
- 2.Witkop CJ. Manifestations of genetic diseases in human pulp. Oral Surg 1971;2013:278–83 [DOI] [PubMed] [Google Scholar]
- 3.Neville BW, Damm DD, Allen CM, et al. Oral & maxillofacial pathology. 5th edn. Philadelphia: WB Saunders, 2002:84–5 [Google Scholar]
- 4.Venugopal Reddy N, Rao VAP, et al. Endodontic treatment in primary molars with taurodontism—a case report. Ann Essences Dent 2010;2013:52–5 [Google Scholar]
- 5.Keith A. Problems relating to the teeth of the earlier forms of prehistoric man. Proc R Soc Med 1913;2013:103–24 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hammer IE III, Witkop CJ. Metro PS-taurodontism report a case. Oral Surg 1964;2013:409–18 [DOI] [PubMed] [Google Scholar]
- 7.Varrela J, Alvesalo L. Taurodontism in 47, XXY males: an effect of the extra X chromosome on root development. J Dent Res 1999;2013:501–2 [DOI] [PubMed] [Google Scholar]
- 8.Rajic Z, Mestrovic SR. Taurodontism in Down's syndrome. Coll Antropol 1998;2013:63–7 [PubMed] [Google Scholar]
- 9.Yeh SC, Hsu TY. Endodontic treatment in taurodontism with Klinefelter's syndrome: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999;2013:612–15 [DOI] [PubMed] [Google Scholar]
- 10.Komatz Y, Tomoyoshi T, Yoshida O, et al. Taurodontism and Klinefelter's syndrome. J Med Genet 1978;2013:452–4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Joseph M. Endodontic treatment in three taurodontic teeth associated with 48, XXXY Klinefelter syndrome: a review and case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;2013:670–77 [DOI] [PubMed] [Google Scholar]
- 12.Islam M, Lurie AG, Reichenberger E. Clinical features of tricho-dento-osseous syndrome and presentation of three new cases: an addition to clinical heterogeneity. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005;2013:736–42 [DOI] [PubMed] [Google Scholar]
- 13.Axelsson S. Variability of the cranial and dental phenotype in Williams's syndrome. Swedish Dent J 2005;2013:3–67 [PubMed] [Google Scholar]
- 14.Johnston NJ, Franklin DL. Dental findings of a child with Wolf-Hirschhorn syndrome. Int J Paediatr Dent 2006;2013:139–42 [DOI] [PubMed] [Google Scholar]
- 15.Dong J, Amor D, Aldred MJ, et al. DLX3 mutation associated with autosomal dominant amelogenesis imperfecta with taurodontism. Am J Med Genet A 2005;2013:138–41 [DOI] [PubMed] [Google Scholar]
- 16.MacDonald-Jankowski DS, Li TT. Taurodontism in a young adult Chinese population. Dentomaxillofac Radiol 1993;2013:140–4 [DOI] [PubMed] [Google Scholar]
- 17.Kuchler EC, De Andrade Risso P, De Castro Costa M, et al. Assessing the proposed association between tooth agenesis and taurodontism in 975 paediatric subjects. Int J Paediatr Dent 2008;2013:231–4 [DOI] [PubMed] [Google Scholar]
- 18.Jafarzadeh H, Azarpazhooh A, Mayhall JT. Taurodontism: a review of the condition and endodontic treatment challenges. Int Endod J 2008;2013:375–88 [DOI] [PubMed] [Google Scholar]
- 19.Shifman A, Chanannel I. Prevalence of taurodontism found in radiographic dental examination of 1,200 young adult Israeli patients. Community Dent Oral Epidemiol 1978;2013:200–3 [DOI] [PubMed] [Google Scholar]
- 20.White SC, Pharoah MJ. Oral radiology. principles and interpretation. 5th edn. St Louis, Missouri: Mosby, 2004:339–40 [Google Scholar]
- 21.Bhat SS, Sargod S, Mohammed SV. Taurodontism in deciduous molars—a case report. J Indian Soc Pedod Prev Dent 2004;2013:193–6 [PubMed] [Google Scholar]
- 22.Rao A, Arathi R. Taurodontism of deciduous and permanent molars: report of two cases. J Indian Soc Pedod Prev Dent 2006;2013:42–4 [DOI] [PubMed] [Google Scholar]