

Abstract
Background:
Obesity is common in patients with cardiovascular disease (CVD) and the vast majority of patients entering into cardiac rehabilitation program (CRP) are obese. Regarding the gender differences, the risk of developing coronary heart disease (CHD) is recognized to be different between obese men and women. So, the purpose of this study was to explore the effect of CRP in functional capacity (FC) and risk factors, such as obesity indexes, lipid profiles, and fasting blood sugar (FBS) in obese men and women with CHD.
Marterials and Methods:
In an observational study between 2000 and 2011, we evaluated a total of 156 obese men and women patients with CHD who were referred to cardiac rehabilitation of Isfahan Cardiovascular Research Institute. Before and after CRP, FC and risk factors were assessed and all the participants completed this period. Data were analyzed with SPSS software version 15. For comparing the mean of outcomes, independent t tests and paired sample t tests were used.
Results:
Data revealed, after CRP, obese women had significant improvement in most evaluated risk factors except total cholesterol (P = 0.05) and FBS (P = 0.09); and obese men had favorable changes in weight (P = 0.00) and body mass index (P = 0.00), FC (P = 0.00) and total cholesterol (P = 0.02); in spite of no significant differences in other lipid profiles. Comparing the 2 groups did not show any significant differences unless high-density lipoprotein cholesterol (P = 0.01) and low-density lipoprotein cholesterol/high-density lipoprotein cholesterol ratio (P = 0.02) had greater improvement in obese women.
Conclusion:
We concluded that CRP is an important step initiating the process of risk reduction and restoration of FC in obese men and obese women with CHD under attendance and supervision of physician, nurse, and exercise physiologist.
Keywords: Cardiac rehabilitation program, coronary heart disease, gender, obesity, risk factor
INTRODUCTION
Raised body mass index (BMI) is common in patients with cardiovascular disease (CVD) and obesity (BMI ≥30) has been known as a risk factor for hypertension, type 2 diabetes, functional capacity (FC), dislipidemia, and generally for coronary heart disease (CHD) that is the most frequent cause of death. The prevalence of obesity in patients with coronary artery disease (CAD) moves toward 40%.[1] Noticeably overall 80% of patients that referred to cardiac rehabilitation program (CRP) were overweight and obese.[2,3]
CRP is known as a way for enhancement and maintenance of cardiovascular health through individualized programs, designed to optimize physical, psychologic, social, vocational, and emotional status by improving coronary risk factors management.[4]
Regarding the gender differences, the risk of developing CVD is recognized to be obviously different between men and women. According to previous studies, CAD presents in women approximately 10 years later than in men;[5] and, the incidence of coronary events was 60% higher in men than in women.[6] Nevertheless, some studies revealed that women have similar improvements in FC and risk factors compared with men after CRP.[7,8]
Also, there are many contradictory results about similarity and dissimilarity between men and women. Kazuhiro et al confirmed gender differences in physiologic outcomes,[5] whereas in another study both the groups benefited in a similar way from CRP in most aspects.[9]
By paying attention to these investigations, there are limited studies comparing obese men with obese women after CRP. So, the purpose of this survey was to explore the effect of CRP on FC and risk factors, such as obesity indexes, lipid profiles, and fasting blood sugar (FBS) in obese men and women patients with CHD; also, to know whether obese men and obese women equally achieve the benefits of CRP or not.
MATERIALS AND METHODS
In an observational study between 2000 and 2011, a total of 156 eligible patients were identified as obese patients with CHD who were referred to phase II cardiac rehabilitation of Isfahan Cardiovascular Research Institute. It should be mentioned that phase II has taken the form of a structured and supervised exercise program in a hospital setting with educational and psychologic support and risk factors modification.[10] The patients’ cardiac diagnoses were defined as a history of at least one of the following: myocardial infarction, coronary artery bypass grafting, percutaneous coronary intervention, and chronic stable angina. For patients to enter a CRP, written informed consent was obtained from all the patients and then their heights and weights (after they had fasted overnight) were measured by a nurse in the morning and BMI was calculated by weight/height2(kg/m2). Also, blood samples were taken after 12-14 h of fasting for measuring FBS, serum lipids, including triglycerides (TG), total cholesterol (TC), high-density lipoprotein (HDL) using enzymatic methods, and low-density lipoprotein (LDL) were calculated.[11] These patients used usual angina treatment and the dose of those medications were not altered during the program. Moreover, the Naughton protocol was followed to conduct exercise tests. Exercise test which was performed by each patient under the supervision of a cardiologist and a nurse, provided an opportunity to identify body reaction by monitoring HR and blood pressure and observing the electrocardiogram. In fact, it determined FC by indicating the changes in hemodynamic responses and metabolic equivalent.[12] All the patients were divided into 2 groups: obese men and obese women; and they began CRP for 2 months, which consisted of 24 sessions and 3 times a week. CRP included exercise training sessions, nutritional and psychologic consultation, and risk factor management. Exercise sessions were similar in each group and exercise training consisted of combined aerobic and resistance training and it was performed in cardiac rehabilitation center under the supervision of a physician, a nurse, and an exercise physiologist by using treadmill, ergometer, stair climbing, rowing, step, jogging, and by using some resistance devices. Each session lasted 90 min, 10-min warm-up followed by 60 min aerobic and resistance training, and finally 20 min cooldown and relaxation. The intensity of training was established according to the clinical condition and calculated between 60% and 85% of maximum heart rate. Blood pressure and heart rate were controlled by the nurse during each session. In addition, personal information of each patient and their history of disease were registered by a nurse and were archived. Also, each patient had individual dietary instruction by a visiting dietitian during the program. After 2 months and completing the rehabilitation program, the tests were accomplished by each patient, again. The research protocol was taken under the medical ethics standards and approved by the Isfahan Cardiovascular Research Centre Ethics Committee, which is a member of the Office for Human Research Protections, U.S. Department of Health and Human Services, with the assurance number: FWA00008578. Independent sample t tests were used to identify baseline differences and comparing the changes between the 2 groups. For investigation about the changes between baseline and completion of CRP, we used paired t tests. Results were expressed as mean and standard deviation (SD) and the level of significance was set at P < 0.05.
RESULTS
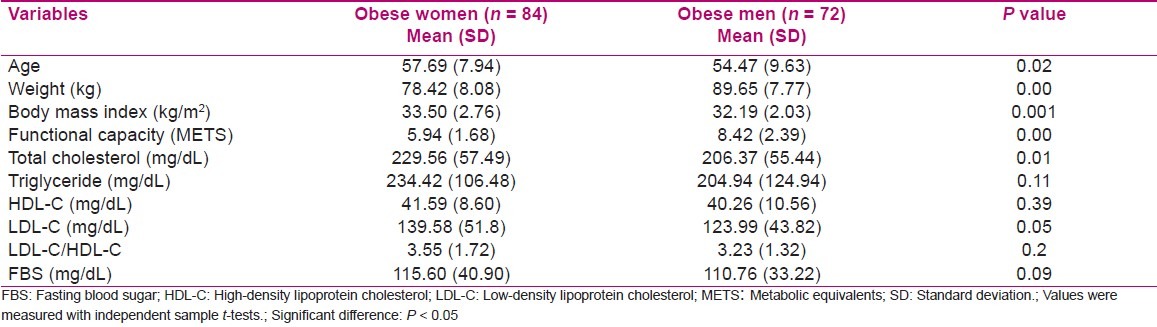
One hundred fifty-six obese patients with CHD were evaluated. They were separated into obese men group [n = 72, age = 54.47 (9.63) years] and obese women group [n = 84, age = 57.69 (7.94) years]. Independent sample t tests were used to identify baseline differences among obese men and obese women patients [Table 1]. At baseline obese men had higher FC (P = 0.001) and weight (P = 0.00); but, TC was higher in women (P = 0.01). Both groups did not have significant differences in other risk factors, such as TG, LDL cholesterol (LDL-C), HDL cholesterol (HDL-C), and FBS.
Table 1.
Comparison between obese women and obese men at baseline
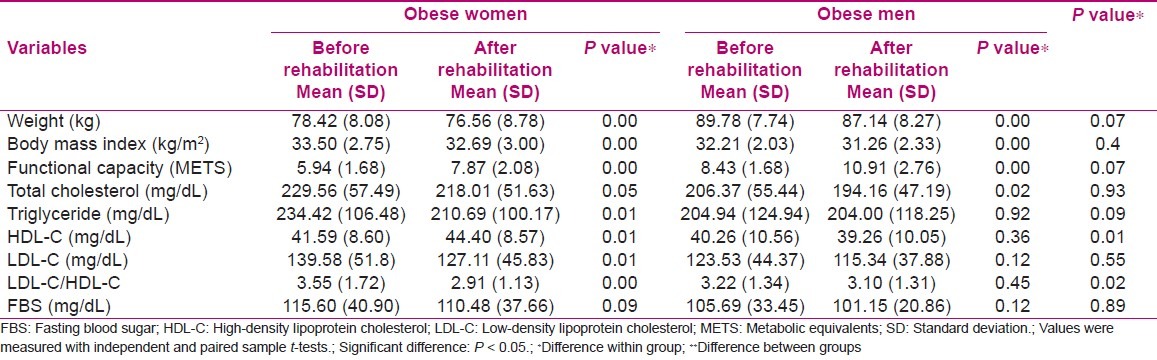
Also, for examination of the changes between baseline and completion of CRP, we used paired sample t tests. Obese women had significant improvements in all risk factors except TC and FBS, and obese men had positive improvement in weight, BMI, FC, and TC but we did not see any significant improvement in other risk factors. Again, for comparing the changes between the 2 groups, independent sample t tests were used. These data did not show any significant differences in FC and most evaluated risk factors except HDL-C and LDL-C/HDL-C, which showed more significant improvement in obese women [Table 2].
Table 2.
Comparison the changes within groups and between groups after cardiac rehabilitation program
DISCUSSION
It is proved that obesity is a major cause of mortality and morbidity and it is associated to CVD and its risk factors, including hyperlipidemia and diabetes mellitus.[2,3] Because the vast majority of patients entering into cardiac rehabilitation are overweight[13] and limited data are available regarding to the effects of CRP and exercise training in obese men and women with CHD, the present study was aimed at finding out the benefits of CRP in obesity indexes, FC, and some lipid profiles on obese men and women.
Our baseline finding showed women who participated in the CRP were 3 years older than men in comparison with 10 years in another study;[4] and, BMI was greater in women than in men, in spite of women’s lower weight; in this regard we can explain that heavier skeleton mass in men can be a cause of men being heavier compared with women. After CRP, both groups attained significant improvement in weight and BMI; but comparison of the 2 groups did not show any significant differences after intervention. Considerably, there are many studies which implied that CRP and exercise training had significant effects in obesity indexes in obese patients with CHD.[14–17] On the contrary, Kiat et al. observed no weight reduction in patients with CAD after 2 years of CRP.[18]
On the other hand, obesity is associated with lower exercise performance, which results in reduced FC after coronary events. In the present study, obese women had lower FC than obese men at baseline, but similar relative improvements were seen (32.49% and 29.41%, respectively) as a result of CRP. The difference between the 2 groups was not significant but data showed greater improvement in women. In this regard, it can be noted that lower baseline FC values may interpret this greater improvement in obese women. Like our results several studies suggested that women had lower FC than men and; also, there were statistical similarities in improvement between men and women.[5,8,19] Generally we can explain that weight reduction after CRP may be a cause for affirmative effects on FC and fitness level in both the groups.[20]
In our results, at baseline, no considerable differences were seen in lipid profiles between two groups except TC, which was higher in obese women than in obese men. After CRP, obese women had favorable changes in TG, HDL-C, LDL-C, and LDL-C/HDL-C; but, TC did not have any significant differences in them. According to a pervious study, there was a significant relationship between TC and obesity, which is due to an increase in cholesterol production with increased weight.[21] Conversely, in obese men improvement was seen just in TC but other lipid factors did not have any significant improvement. In fact, obese men had very modest overall lipid improvements after CRP. Also, comparing the 2 groups showed that among lipid profiles, substantial differences were seen only in HDL-C and LDL-C/HDL-C. In relation to TG, we can note that obese women had higher TG value at baseline that was the strongest predictor of improvement in TG level when compared with men after CRP. In addition, there are many investigations that have similarity or dissimilarity to our finding. Lavie and Milani showed significant improvement in HDL-C and LDL-C/HDL-C in obese patients but other lipid profiles did not have any changes during CRP.[17] Also, another study suggested improvement only in HDL-C in women after comprehensive CRP.[18] Williams et al. did not demonstrate significant reductions in LDL-C levels with obesity intervention, exercise training, and dietary therapy.[22] Some studies proposed weight reduction with exercise training, and dietary limitation has significant effects on increasing levels of HDL-C and reducing TG.[20] Another study showed that patients had improvement in TC, TG, HDL-C, LDL-C, and LDL-C/HDL-C after cardiac rehabilitation and exercise training.[14] Also, Sarrafzadegan et al. signified CRP as a cause of improvement in all lipid profiles without sex differences.[9] Brochu et al. reported that neither men nor women patients experienced a significant overall improvement in TC, LDL-C, and TG after the 3-month exercise training alone.[23] The present study did not show significant improvement in FBS in obese men and women after CRP. Brochu et al. confirmed our result,[23] but Ades et al. mentioned exercise and weight reduction prevent type II diabetes and increasing FBS.[15] About some disparities between our study and other investigations, we can mention that lower age difference between our groups and also the range of patients’ age and even the kind and level of exercise training and finally variation in their diets may be the cause for dissimilarities.
In general, it is understood that at baseline women had worse CVD risk factors than men. After CRP, both the groups achieved significant improvements in FC and most evaluated risk factors. And comparing the 2 groups demonstrated no significant differences between them except HDL-C and LDL-C/HDL-C. So, it should be noted that both obese men and obese women can benefit from CRP without any attention to gender differences.
There were several limitations in the present study. The first limitation was short-term intervention, which consisted of 24 sessions of CRP. It would be desirable to document long-term intervention changes in physiologic outcomes and risk profiles in patients with CHD. The second limitation was the lack of control group who did not participate in CRP after cardiac events, and comparing them to our groups. The third limitation was that a detailed evaluation of dietary adherence and exercise training outside of the formal CRP was not available. We can suggest for future researches to study, whether considerable weight reduction after CRP results in improved clinical outcomes in patients with CHD or not.
CONCLUSION
We conclude that CRP, which is accomplished under attendance and supervision of a physician, a nurse, and an exercise physiologist is an important step initiating the process of risk reduction and restoration of FC in obese men and women with CHD. It is an acceptable management for enhancement and maintenance of cardiovascular health through individualized programs designed to optimize physical condition and manage related risk factors, such as obesity indexes and lipid profiles.[24]
ACKNOWLEDGMENT
We thank all physicians and nurses and staffs in the Isfahan Cardiovascular Research Institute.
Footnotes
Source of Support: All physicians and nurses and staffs in the Isfahan Cardiovascular Research Institute
Conflict of Interest: None.
REFERENCES
- 1.Lavie CJ, Milani RV. Benefits of cardiac rehabilitation and exercise training. Chest. 2000;117:15–7. doi: 10.1378/chest.117.1.5. [DOI] [PubMed] [Google Scholar]
- 2.Gunstad J, Luyster F, Hughes J, Waechter D, Rosneck J, Josephson R. The effects of obesity on functional work capacity and quality of life in phase II cardiac rehabilitation. Prev Cardiol. 2007;10:64–7. doi: 10.1111/j.1520-037x.2007.05860.x. [DOI] [PubMed] [Google Scholar]
- 3.Al Orifan FH, Badr HE, Sabour Se’adah MA, Khadadah KE, Al Kordi B, Abass A. Obesity and cardiovascular risk factors in Kuwaiti adults. Kuwait Med J. 2007;39:162–6. [Google Scholar]
- 4.Eshah NF, Bond AE. Cardiac rehabilitation programme for coronary heart disease patients: An integrative literature review. Int J Nurs Pract. 2009;15:131–9. doi: 10.1111/j.1440-172X.2009.01738.x. [DOI] [PubMed] [Google Scholar]
- 5.Wake R, Yoshiyama M. Gender differences in ischemic heart disease. Recent Pat Cardiovasc Drug Discov. 2009;4:234–40. doi: 10.2174/157489009789152249. [DOI] [PubMed] [Google Scholar]
- 6.Izawa KP, Oka K, Watanabe S, Yokoyama H, Hiraki K, Morio Y, et al. Gender-related differences in clinical characteristics and physiological and psychosocial outcomes of Japanese patients at entry into phase II cardiac rehabilitation. J Rehabil Med. 2008;40:225–30. doi: 10.2340/16501977-0156. [DOI] [PubMed] [Google Scholar]
- 7.Mosca L, Manson JE, Sutherland SE, Langer RD, Manolio T, Barrett-Connor E. Cardiovascular disease in women: a statement for healthcare professionals from the American heart association. Writing Group. Circulation. 1997;96:2468–82. doi: 10.1161/01.cir.96.7.2468. [DOI] [PubMed] [Google Scholar]
- 8.Cannistra LB, Balady GJ, O’Malley CJ, Weiner DA, Ryan TJ. Comparison of the clinical profile and outcome of women and men in cardiac rehabilitation. Am J Cardiol. 1992;69:1274–9. doi: 10.1016/0002-9149(92)91220-x. [DOI] [PubMed] [Google Scholar]
- 9.Sarrafzadegan N, Rabiei K, Kabir A, Sadeghi M, Khosravi A, Asgari S, et al. Gender differences in risk factors and outcomes after cardiac rehabilitation. Acta Cardiol. 2008;63:763–70. doi: 10.2143/AC.63.6.2033395. [DOI] [PubMed] [Google Scholar]
- 10.Donker FJ. Cardiac rehabilitation: A review of current developments. Clin Psychol Rev. 2000;20:923–43. doi: 10.1016/s0272-7358(99)00016-1. [DOI] [PubMed] [Google Scholar]
- 11.Branchi A, Rovellini A, Torri A, Sommarva D. Accuracy of calculated serum low-density lipoprotein cholesterol for the assessment of coronary heart disease risk in NIDDM patients. Diabetes Care. 1998;21:1397–402. doi: 10.2337/diacare.21.9.1397. [DOI] [PubMed] [Google Scholar]
- 12.Morrow DA, Gersh BJ. Chronic coronary artery disease. In: Libby P, Braunwald E, Bonow RO, Zipes DP, editors. Braunwald’s heart disease: A textbook of cardiovascular medicine. Philadelphia: Saunders/Elsevier; 2008. pp. 1353–417. [Google Scholar]
- 13.Savage PD, Ades PA. The obesity epidemic in the United States: role of cardiac rehabilitation. Coron Artery Dis. 2006;17:227–31. doi: 10.1097/00019501-200605000-00004. [DOI] [PubMed] [Google Scholar]
- 14.Lavie CJ, Milani RV. Effects of cardiac rehabilitation and exercise training on low-density lipoprotein cholesterol in patients with hypertriglyceridemia and coronary artery disease. Am J Cardiol. 1994;74:1192–5. doi: 10.1016/0002-9149(94)90546-0. [DOI] [PubMed] [Google Scholar]
- 15.Ades AP, Savage PD, Toth MJ, Harvey-Berino J, Schneider DJ, Bunn JY, et al. High-calorie-expenditure exercise: a new approach to cardiac rehabilitation for overweight coronary patients. Circulation. 2009;119:2671–8. doi: 10.1161/CIRCULATIONAHA.108.834184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bader DS, Maguire TE, Spahn CM, O’Malley CJ, Balady GJ. Clinical profile and outcomes of obese patients in cardiac rehabilitation stratified according to National Heart, Lung, and Blood Institute criteria. J Cardiopulm Rehabil. 2001;21:210–7. doi: 10.1097/00008483-200107000-00003. [DOI] [PubMed] [Google Scholar]
- 17.Lavie CJ, Milani RV. Effects of cardiac rehabilitation and exercise training in obese patients with coronary artery disease. Chest. 1996;109:52–6. doi: 10.1378/chest.109.1.52. [DOI] [PubMed] [Google Scholar]
- 18.Kiat A, Cook E, Kiat H. Weight loss and fitness in patients with coronary artery disease through cardiac rehabilitation - A long term follow-up. Internet J Cardiovasc Res. 2011;7:32–38. [Google Scholar]
- 19.O’Farrel P, Murray J, Huston P, LeGrand C, Adamo K. Sex differences in cardiac rehabilitation. Can J Cardiol. 2000;16:319–25. [PubMed] [Google Scholar]
- 20.Lavie CJ, Milani RV. Effects of cardiac rehabilitation, exercise training, and weight reduction on exercise capacity, coronary risk factors, behavioral characteristics, and quality of life in obese coronary patients. Am J Cardiol. 1997;79:397–401. doi: 10.1016/s0002-9149(97)89239-9. [DOI] [PubMed] [Google Scholar]
- 21.Sadeghi M, Roohafza HR, Baghaei AM, Pourmoghaddas M, Shirani SH, Sadri GH, et al. Obesity and its association with other cardiovascular risk factors in women in central Iran. Women Healthy Heart Program. Arya journal is Iranian journal about cardiovascular disease. 2005;1:75–9. [Google Scholar]
- 22.Williams PT, Krauss RM, Vranizan KM, Wood PDS. Changes in lipoprotein subfractions during diet-induced and exercise-induced weight loss in moderately overweight men. Circulation. 1990;81:1293–304. doi: 10.1161/01.cir.81.4.1293. [DOI] [PubMed] [Google Scholar]
- 23.Brochu M, Poehlman ET, Savage P, Fragnoli-Munn K, Ross S, Ades PA. Modest effects of exercise training alone on coronary risk factors and body composition in coronary patients. J Cardiopulm Rehabil. 2000;20:180–8. doi: 10.1097/00008483-200005000-00006. [DOI] [PubMed] [Google Scholar]
- 24.Kennedy MD, Haykowsky M, Daub B, Van Lohuizen K, Knapik G, Black B. Effects of a comprehensive cardiac rehabilitation program on quality of life and exercise tolerance in women: A retrospective analysis. Curr Control Trials Cardiovasc Med. 2003;4:1. doi: 10.1186/1468-6708-4-1. [DOI] [PMC free article] [PubMed] [Google Scholar]